Describe the collateral circulation of female pelvis and its clinical significanc
Collateral Circulation of the Female Pelvis
Overview
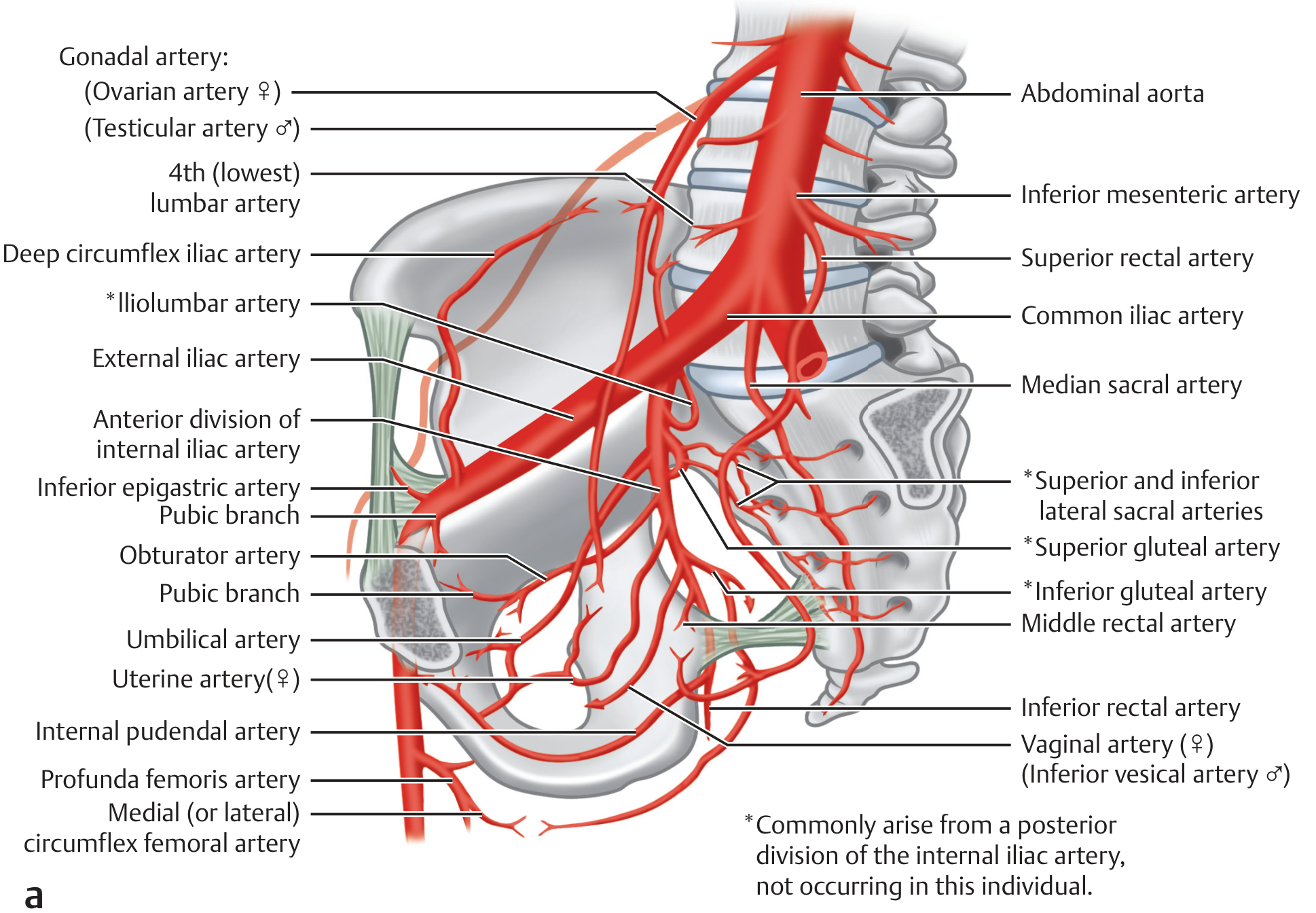
Primary Arterial Supply
- External iliac artery - passes under the inguinal ligament to become the femoral artery
- Internal iliac artery (hypogastric artery) - the dominant supply to pelvic viscera
| Division | Key Branches (Female) |
|---|---|
| Anterior | Uterine, vaginal, superior/inferior/middle vesical, middle rectal, obturator, inferior gluteal, internal pudendal |
| Posterior | Iliolumbar, lateral sacral, superior gluteal |
The Collateral Networks
1. Uterine Artery - Ovarian Artery Anastomosis
- Ligation of the uterine artery alone rarely fully devascularizes the uterus
- Embolization procedures targeting uterine fibroids must account for ovarian artery collateral supply
2. Bilateral Cross-Pelvic Anastomoses (Transverse Pelvic Collaterals)
- Right and left uterine arteries anastomose across the uterine body
- Right and left vaginal arteries form a vaginal plexus
- Right and left vesical arteries anastomose over the bladder
- Right and left middle rectal arteries anastomose over the rectum
3. Rectal Anastomotic Chain (Three-Level Rectal Supply)
- Superior rectal artery (from inferior mesenteric artery - IMA)
- Middle rectal artery (from anterior division of internal iliac)
- Inferior rectal artery (from internal pudendal artery)
4. Vesical Anastomotic Network
- Middle vesical artery
- Uterine artery (via vesicouterine anastomosis)
- Vaginal artery
5. Lumbar-Iliolumbar-Lateral Sacral Network (Parietal Collaterals)
- Lumbar arteries anastomose with the iliolumbar artery (from posterior division of internal iliac)
- Iliolumbar anastomoses with lateral sacral and deep circumflex iliac arteries
- This allows reconstitution of internal iliac flow from above
6. Winslow Pathway (Thoraco-Epigastric Collateral)
7. Internal Iliac Occlusion Collaterals
- Transverse pelvic collaterals via contralateral lateral sacral, obturator, and internal pudendal arteries
- Median sacral artery (from aorta) provides midline sacral supply
- Ascending branch of lateral circumflex femoral and deep circumflex iliac provide retrograde flow to superior gluteal and iliolumbar territories
8. Trochanteric and Cruciate Anastomoses (Pelvic-Femoral Junction)
- Trochanteric anastomosis: superior and inferior gluteal arteries + deep circumflex iliac + medial and lateral circumflex femoral arteries
- Cruciate anastomosis: lateral and medial circumflex femoral + inferior gluteal + first perforating branch of profunda femoris
Clinical Significance
1. Internal Iliac (Hypogastric) Artery Ligation in Postpartum Hemorrhage
"Burchell described the pelvic vascular supply and demonstrated that the transient decreases in blood pressure and blood flow through regional vessels that occur at the time of internal iliac artery ligation are responsible for the control of hemorrhage. Because of the ample collateral circulation, there appear to be no long-term consequences of hypogastric artery ligation, and women have delivered normal infants in subsequent pregnancies after undergoing this procedure."
- Ligation of the anterior division (distal to where the posterior division branches) is preferred to preserve gluteal and sacral supply
- Bilateral ligation is usually required due to extensive cross-pelvic anastomoses
- Uterine artery ligation (O'Leary sutures) is typically attempted first; hypogastric ligation follows if unsuccessful
2. Uterine Artery Embolization (UAE) for Fibroids
- Ovarian artery collaterals that reconstitute uterine blood supply after embolization, potentially leading to fibroid regrowth
- Non-target embolization risk to bowel and bladder via collateral connections
- In diagnostic radiology, cross-flow collateral is so robust that bilateral embolization is required (Grainger & Allison's)
3. Radical Pelvic Surgery (Hysterectomy, Wertheim's Operation)
- The uterine artery is ligated at its origin from the internal iliac
- The rich collaterals (ovarian-uterine, vaginal, vesicouterine) must be systematically controlled
- The ureter runs beneath the uterine artery ("water under the bridge") in close proximity to these anastomotic vessels - a key danger zone
4. Pelvic Fracture and Retroperitoneal Hemorrhage
5. Aortoiliac Occlusive Disease (Leriche Syndrome)
6. CABG Planning in Patients with Aortoiliac Disease
7. Ureteral Blood Supply Preservation
- Renal artery (upper ureter)
- Ovarian/gonadal artery (mid ureter)
- Uterine artery (lower ureter)
- Vesical arteries (juxtavesical ureter)
8. Bladder Preservation after Vessel Ligation
Summary Table: Key Anastomoses and Their Clinical Relevance
| Anastomosis | Vessels Involved | Clinical Relevance |
|---|---|---|
| Uterine-Ovarian | Uterine art. (IIA) + Ovarian art. (Aorta) | UAE failure, PPH control, fertility surgery |
| Bilateral midline | R + L uterine, vesical, rectal arteries | Bilateral IIA ligation needed for hemorrhage |
| Rectal triple supply | Superior + middle + inferior rectal | Rectal viability after pelvic surgery |
| Lumbar-Iliolumbar | Lumbar + iliolumbar + lateral sacral | Reconstitutes IIA in Leriche syndrome |
| Winslow pathway | Subclavian → thoracic → epigastric | CABG planning in aortoiliac disease |
| Trochanteric/Cruciate | Gluteal + circumflex femoral | Lower limb perfusion in iliac occlusion |
| Transverse pelvic | Contralateral lateral sacral, obturator | IIA occlusion compensation |
- Imaging Anatomy Text and Atlas Vol. 3 - Arterial Collateral Network of the Pelvis, p. 357-358
- Sabiston Textbook of Surgery, 10th ed. - Vascular Structures of the Female Pelvis, p. 2786
- Creasy & Resnik's Maternal-Fetal Medicine - Postpartum Hemorrhage, p. 948
- Hinman's Atlas of Urologic Surgery - General Vascular Surgical Principles
Give simple diagram of pelvic collateral for exam
Clean, simple medical exam diagram of pelvic collateral circulation in the female pelvis. White background, bold black labels, color-coded arrows. Show the abdominal aorta at top center branching into common iliac arteries on each side. Each common iliac splits into external iliac and internal iliac (hypogastric). Internal iliac splits into anterior division (uterine artery, vaginal artery, vesical arteries, middle rectal, obturator, inferior gluteal, internal pudendal) and posterior division (iliolumbar, lateral sacral, superior gluteal). Show ovarian artery arising directly from aorta anastomosing with uterine artery (highlight this in red as key anastomosis). Show bilateral cross-connections between left and right uterine arteries across the uterus. Show rectal anastomotic chain: superior rectal (from IMA) connecting to middle rectal (IIA) and inferior rectal (internal pudendal). Show Winslow pathway on one side as dotted line: subclavian to internal thoracic to superior epigastric to inferior epigastric to external iliac. Show lumbar artery to iliolumbar anastomosis. Use colored boxes or callout labels for key clinical points: "Bilateral ligation needed for PPH", "Key anastomosis for UAE failure", "Rectal triple supply". Simple, clean, exam-ready style with numbered labels.
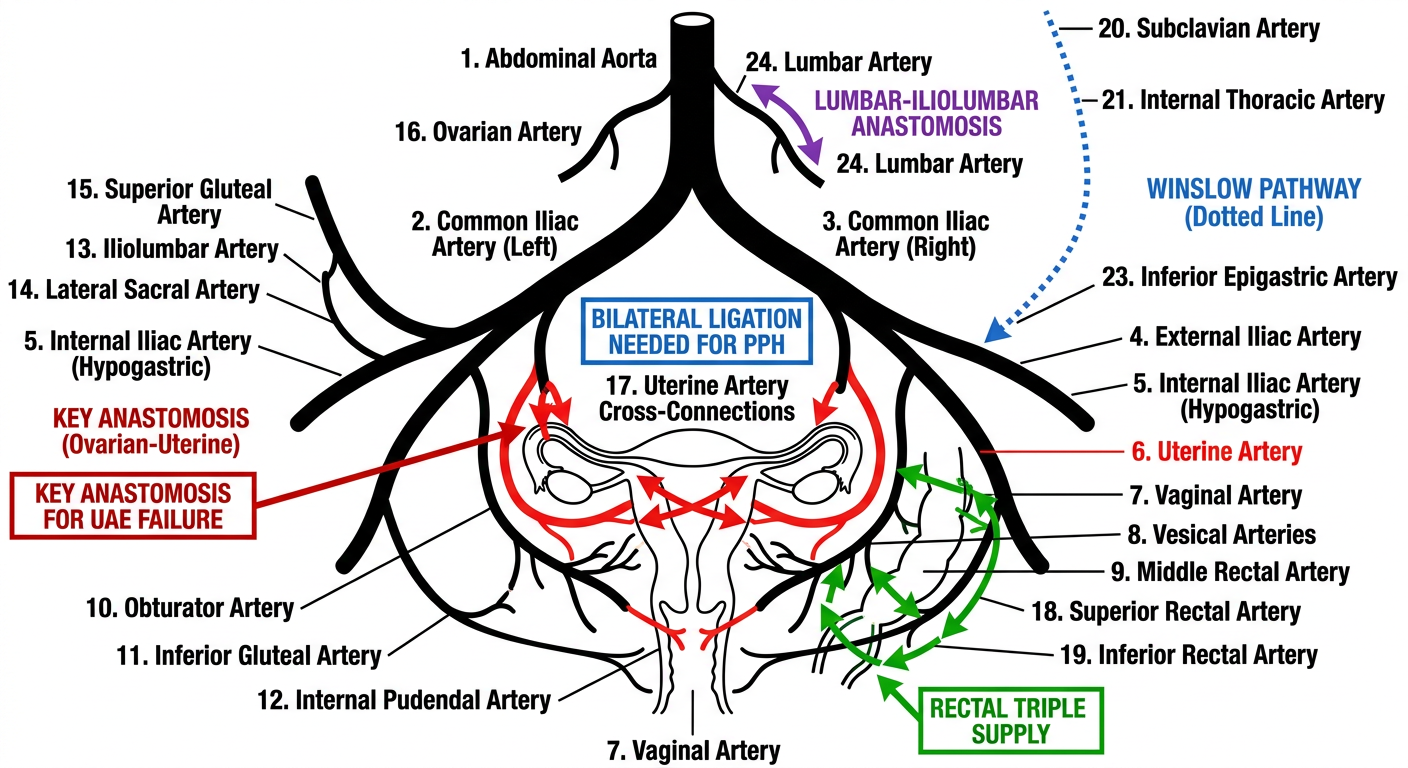
Exam Memory Points
- Uterine art. ↔ Ovarian art. - Most important; why UAE can fail (ovarian collateral reconstitutes fibroid supply)
- Right uterine ↔ Left uterine - Cross-midline; why bilateral IIA ligation is needed for PPH
- Superior rectal (IMA) ↔ Middle rectal (IIA) ↔ Inferior rectal (pudendal) - Protects rectum after pelvic surgery
- Lumbar art. ↔ Iliolumbar art. ↔ Lateral sacral - Reconstitutes internal iliac in Leriche syndrome
- Winslow pathway: Subclavian → Int. thoracic → Sup. epigastric → Inf. epigastric → Ext. iliac - Critical for CABG planning in aortoiliac disease
| Anastomosis | Remember as |
|---|---|
| Uterine-Ovarian | "UAE needs mapping" |
| Bilateral uterine cross | "PPH needs bilateral ligation" |
| Triple rectal | "Rectum rarely dies" |
| Lumbar-Iliolumbar | "Leriche reconstitution" |
| Winslow | "CABG danger in PAD" |