Hormonal regulation of blood glucose levels
Reading File
Finding Sources
Finding Sources
Searching the Web
hormonal regulation of blood glucose levels physiology insulin glucagon
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full response.
Hormonal Regulation of Blood Glucose Levels
Blood glucose (plasma glucose) is tightly maintained between 70-100 mg/dL (fasting) through a coordinated interplay of hormones, neural signals, and substrate effects. This is called glucose homeostasis or metabolic homeostasis.
- Basic Medical Biochemistry - A Clinical Approach, 6e, p. 694
- Biochemistry (Lippincott), 8e, p. 877
- Harrison's Principles of Internal Medicine, 22E, p. 3275
1. Overview: The Principal Hormones
| Hormone | Source | Net Effect on Blood Glucose |
|---|---|---|
| Insulin | Pancreatic β-cells | Decreases (hypoglycemic) |
| Glucagon | Pancreatic α-cells | Increases (hyperglycemic) |
| Epinephrine | Adrenal medulla | Increases (hyperglycemic) |
| Cortisol | Adrenal cortex | Increases (slow, transcriptional) |
| Growth hormone | Anterior pituitary | Increases (slow, transcriptional) |
The ratio of insulin to glucagon is what most directly controls blood glucose at any moment.
2. Insulin - The Anabolic Hypoglycemic Hormone
Source and Structure
Insulin is a polypeptide synthesized as proinsulin in the β-cells of the islets of Langerhans. Proinsulin is cleaved into mature insulin and C-peptide in storage vesicles. C-peptide is released in equimolar amounts with insulin and can be used as a clinical marker of endogenous insulin secretion.
Stimuli for Insulin Secretion
- Elevated blood glucose (primary stimulus) - glucose enters β-cells via GLUT-2 transporters
- Amino acids (especially arginine, leucine)
- GI hormones (GLP-1, GIP - incretin effect)
- Vagal stimulation (anticipatory, cephalic phase)
- Sulfonulyureas (pharmacologic, block K-ATP channels)
Mechanism of Glucose-Stimulated Insulin Secretion
Glucose enters β-cells → undergoes glycolysis → raises the ATP/ADP ratio → closes K-ATP channels → cell membrane depolarizes → voltage-gated Ca²⁺ channels open → Ca²⁺ influx → exocytosis of insulin granules.
Biphasic response:
- First phase - rapid, from pre-formed granules docked at the membrane; impaired early in type 2 diabetes
- Second phase - sustained, from deeper vesicles + newly synthesized insulin
Mechanism of Action
Insulin binds its receptor tyrosine kinase on target cell surfaces → autophosphorylation of the receptor → downstream phosphorylation cascades → promotes dephosphorylation of key metabolic enzymes (opposite to glucagon/cAMP-PKA effects).
Key effector: translocation of GLUT-4 to cell membranes in muscle and adipose tissue, greatly increasing glucose uptake.
Metabolic Effects of Insulin (Fed/Anabolic State)
In the liver:
- Promotes glycogen synthesis (activates glycogen synthase, inhibits glycogen phosphorylase)
- Promotes glycolysis and inhibits gluconeogenesis
- Promotes triglyceride synthesis (promotes lipogenesis)
- Inhibits ketogenesis
In skeletal muscle:
- Promotes glucose uptake via GLUT-4
- Promotes glycogen synthesis
- Promotes protein synthesis
In adipose tissue:
- Promotes glucose uptake via GLUT-4
- Promotes triglyceride synthesis and storage
- Inhibits hormone-sensitive lipase (anti-lipolytic)
Other effects:
- Promotes K⁺ uptake into cells (Na⁺-K⁺ ATPase activation) - clinically used in hyperkalemia treatment
- Promotes cell growth and protein synthesis
3. Glucagon - The Catabolic Hyperglycemic Hormone
Source and Stimuli for Secretion
- Low blood glucose (primary stimulus) - overnight or prolonged fasting
- Amino acids (arginine) from a protein meal - prevents hypoglycemia that would otherwise follow the insulin response to that meal
- Catecholamines (epinephrine, norepinephrine via sympathetic innervation) - especially during physiologic stress
Glucagon secretion is suppressed by: elevated blood glucose and by insulin (both rise after a carbohydrate meal).
Mechanism of Action
Glucagon binds G protein-coupled receptors (GPCRs) on hepatocyte membranes → activates adenylyl cyclase → raises cAMP → activates Protein Kinase A (PKA) → phosphorylation of key regulatory enzymes.
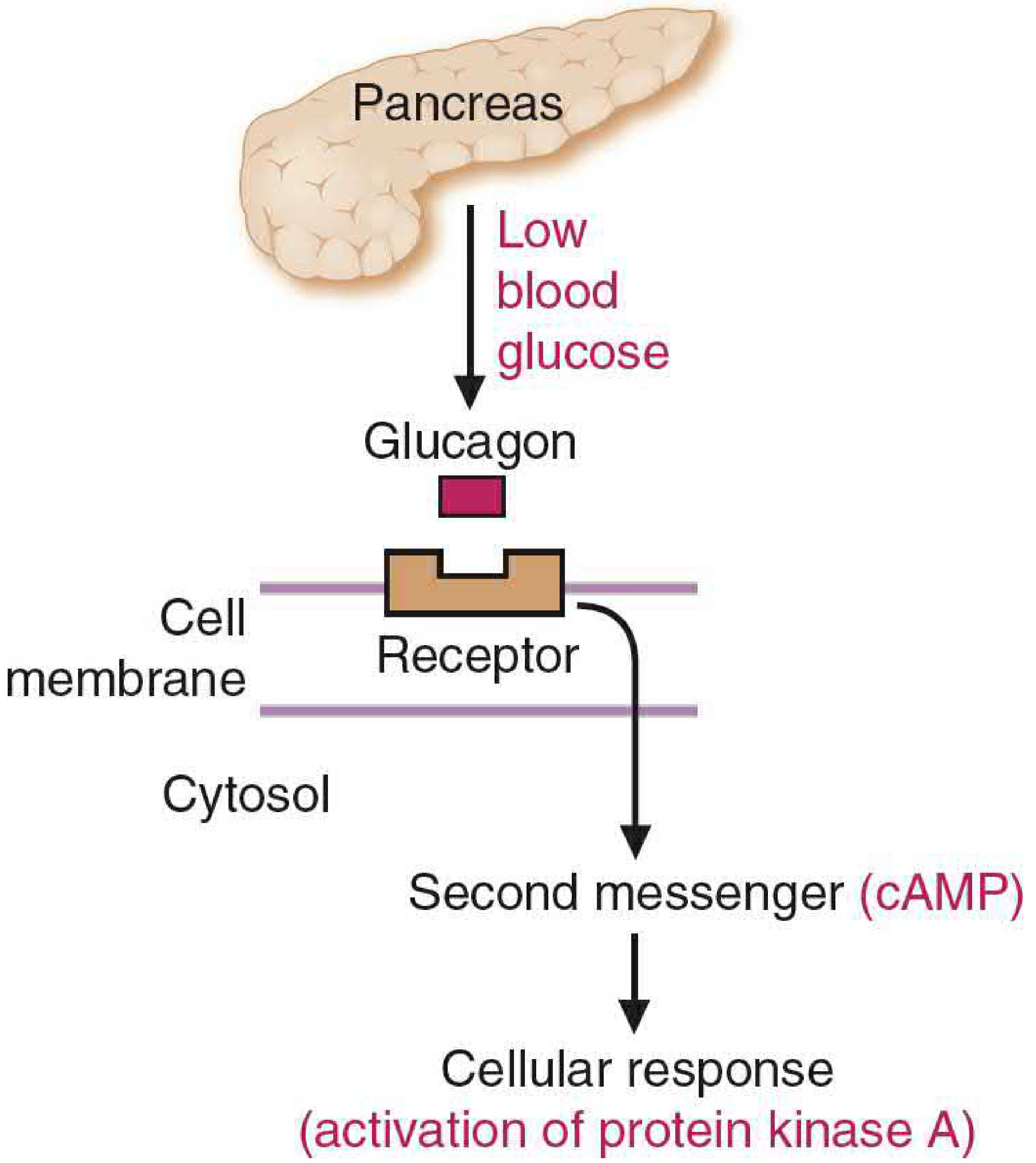
Metabolic Effects of Glucagon (Fasting/Catabolic State)
Carbohydrate metabolism (primary target: liver):
- Stimulates glycogenolysis (glycogen → glucose-1-phosphate → glucose)
- Stimulates gluconeogenesis (from amino acids, lactate, glycerol)
- Inhibits glycolysis (reduces PFK-1 activator fructose 2,6-bisphosphate)
- Daytime blood glucose maintained mainly by glycogenolysis; as the overnight fast lengthens, glycogen stores fall and gluconeogenesis becomes the dominant contributor
Lipid metabolism:
- Stimulates lipolysis in adipose tissue (via protein kinase A activation of hormone-sensitive lipase)
- Inhibits fatty acid synthesis (phosphorylates and inactivates ACC)
- Removes inhibition on CPT-1, enabling fatty acid β-oxidation and ketogenesis
Protein metabolism:
- Increases hepatic uptake of amino acids from muscle → carbon skeletons for gluconeogenesis
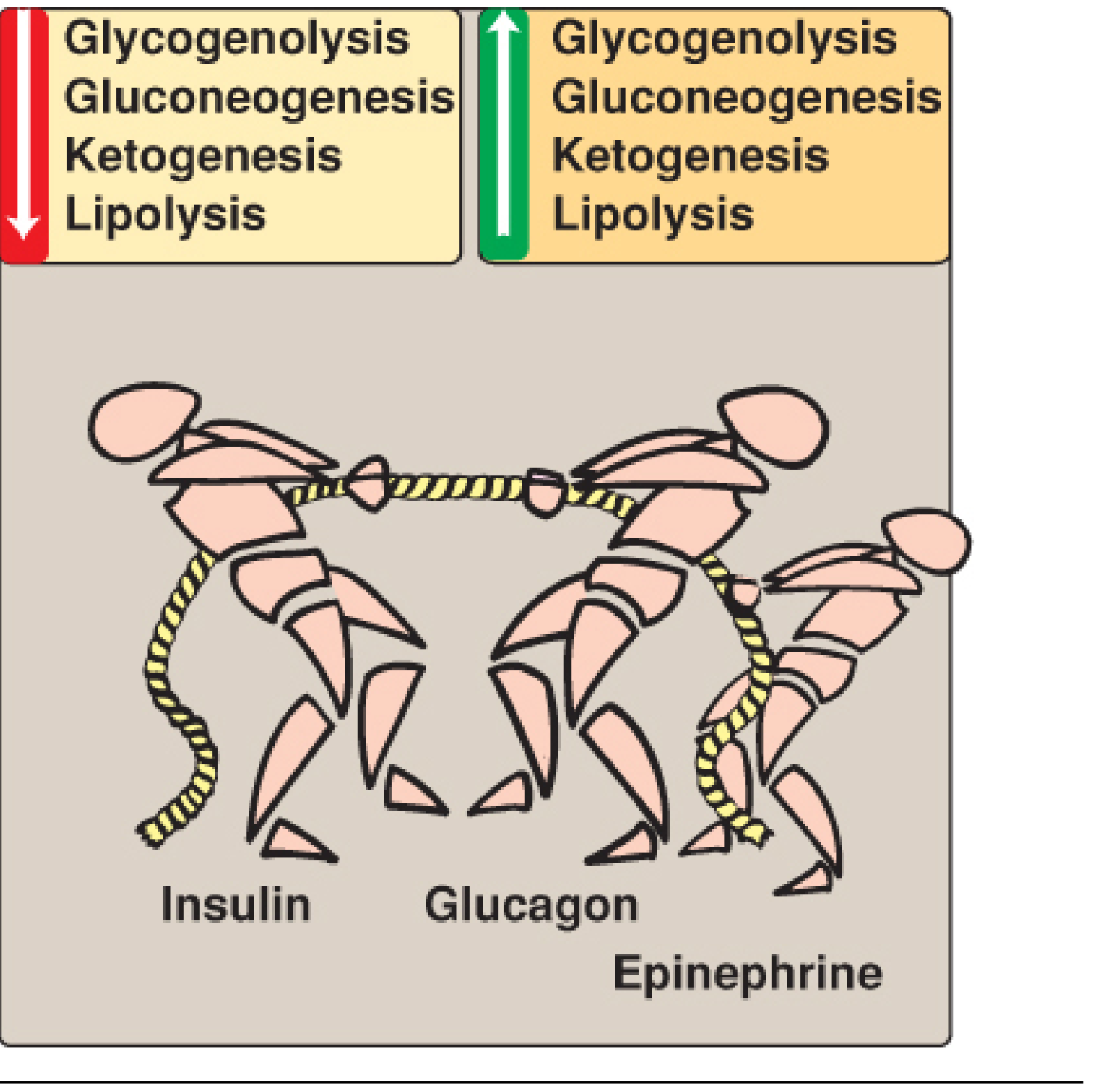
4. The Insulin-Glucagon Tug-of-War
The opposing actions of these hormones on hepatic metabolism are shown below. Insulin turns on glycolysis, glycogenesis, and lipogenesis; glucagon + epinephrine turn on glycogenolysis, gluconeogenesis, ketogenesis, and lipolysis.
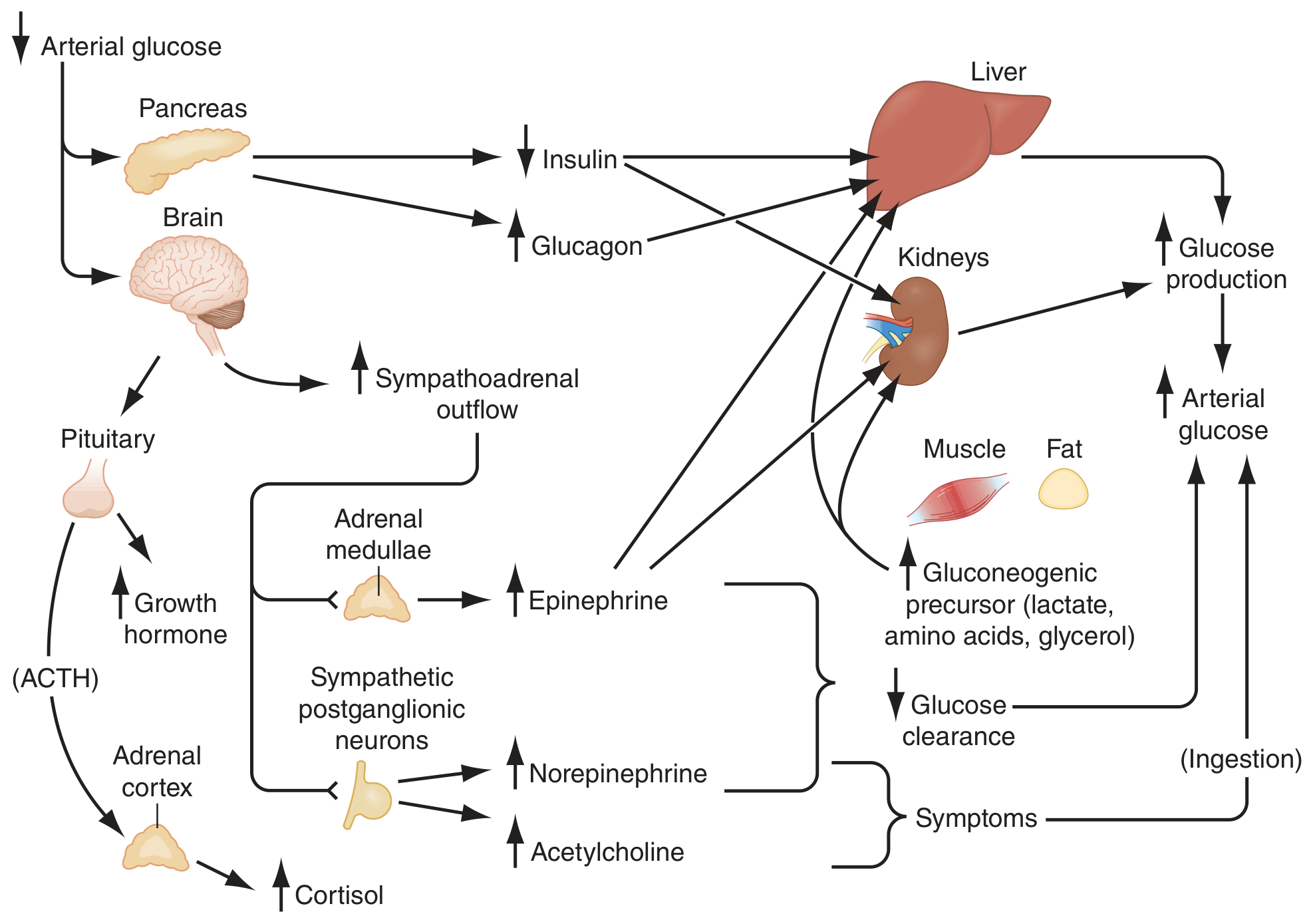
5. Counterregulatory Hormones
When blood glucose falls below the physiologic range, a hierarchical set of counterregulatory responses is activated. According to Harrison's (22E), the glycemic thresholds and response hierarchy are:
| Glycemic Threshold | Response | Role |
|---|---|---|
| ~4.4-4.7 mmol/L (80-85 mg/dL) | ↓ Insulin secretion | First defense - increases hepatic glucose output |
| Just below physiologic range | ↑ Glucagon secretion | Primary counterregulatory response - stimulates glycogenolysis + gluconeogenesis |
| ~3.8 mmol/L (~68 mg/dL) | ↑ Epinephrine (adrenal medulla) | Critical when glucagon deficient (e.g., late type 1 DM) |
| Below ~3.3 mmol/L (~60 mg/dL) | Cognitive impairment (CNS symptoms) | Neuroglycopenia |
| Prolonged (>4 hours) hypoglycemia | ↑ Cortisol, ↑ Growth hormone | Slow (transcriptional), minor acute role |
Epinephrine
- Stimulates hepatic glycogenolysis AND gluconeogenesis
- Stimulates renal gluconeogenesis
- Inhibits insulin secretion (preventing GLUT-4-mediated muscle/adipose uptake)
- Stimulates lipolysis → provides glycerol + fatty acids (gluconeogenic substrate + alternative fuel)
- Binds β-adrenergic receptors on liver/muscle (note: epinephrine receptors differ from glucagon receptors and are also present on skeletal muscle, whereas glucagon receptors are not)
Cortisol
- Stimulates gluconeogenesis (permissive effects via gene transcription)
- Promotes protein catabolism in muscle → provides amino acid precursors
- Antagonizes insulin action in peripheral tissues (insulin resistance)
- Acts slowly (hours-days); no meaningful role in acute hypoglycemia defense
Growth Hormone
- Stimulates lipolysis (provides fatty acids as alternative fuel, spares glucose)
- Inhibits insulin-stimulated glucose uptake in peripheral tissues
- Like cortisol, plays a role in prolonged (not acute) hypoglycemia
6. Postprandial vs. Fasting States Summary
| State | Key Hormones | Key Metabolic Events |
|---|---|---|
| Fed / Postprandial | High insulin, Low glucagon | ↑ Glucose uptake (GLUT-4), ↑ Glycogenesis, ↑ Lipogenesis, ↑ Protein synthesis |
| Early fasting (2-4 h) | Low insulin, High glucagon | Hepatic glycogenolysis → maintains blood glucose |
| Prolonged fasting (overnight) | Very low insulin, High glucagon | Gluconeogenesis increases (supplies ~60-70% of hepatic glucose output); lipolysis; ketogenesis |
| Stress / exercise | Catecholamines + glucagon dominant | Rapid glycogenolysis, lipolysis, gluconeogenesis; insulin suppressed |
7. Clinical Correlations
| Condition | Hormonal Disturbance | Result |
|---|---|---|
| Type 1 diabetes | Absolute insulin deficiency | Hyperglycemia, DKA, K⁺ shifts (hyperkalemia) |
| Type 2 diabetes | Insulin resistance + relative deficiency; impaired 1st-phase secretion | Hyperglycemia, dyslipidemia |
| Insulinoma | Excess insulin (tumor) | Fasting hypoglycemia (Whipple's triad) |
| Hypoglycemia in late T1DM | Absent glucagon + blunted epinephrine response | Loss of counterregulation → severe hypoglycemia unawareness |
| Glucagonoma | Excess glucagon | Hyperglycemia + necrolytic migratory erythema |
| Cushing's syndrome | Excess cortisol | Insulin resistance, hyperglycemia |
Key takeaway: Blood glucose regulation is a dynamic balance between insulin (the single hypoglycemic hormone) and multiple hyperglycemic counterregulatory hormones (glucagon, epinephrine, cortisol, growth hormone). Glucagon is the mirror-image of insulin and is the primary counterregulatory hormone; epinephrine becomes critical as a backup; cortisol and growth hormone act slowly and play no role in acute hypoglycemia defense.
This is a shared conversation. Sign in to Orris to start your own chat.