Bronchography full details for md exam answer 10 marks
Reading File
Finding Sources
Finding Sources
Searching the Web
bronchography procedure indications contraindications technique MD exam
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
I now have enough material from the textbooks combined with my knowledge to write a comprehensive MD exam answer. Let me compile it.
Bronchography - Comprehensive MD Exam Answer (10 Marks)
Definition
Bronchography is a radiological procedure in which a radio-opaque (contrast) medium is introduced into the tracheobronchial tree, following which serial radiographs are taken to outline the bronchi and their subdivisions. It produces an image called a bronchogram.
It has been largely replaced in modern practice by high-resolution CT (HRCT), fiberoptic bronchoscopy, and CT with 3D reconstruction, but remains of historical and conceptual importance in surgical and ENT examinations.
(Murray & Nadel's Textbook of Respiratory Medicine: "Contrast bronchography, formerly a fairly common thoracic examination, has been replaced by the performance of fiberoptic bronchoscopy or by imaging via either CT or high-resolution CT of the lungs.")
Contrast Media Used
The contrast agent must be:
- Radio-opaque (iodine-based)
- Viscid enough to coat bronchial walls
- Absorbable or removable by coughing
Agents used:
- Propyliodone (Dionosil) - oil-based suspension; most commonly described in classical texts
- Dionosil aqueous - water-miscible, less irritating
- Barium sulfate - rarely used due to retention risk
- Powdered tantalum - insoluble, used for radiographic contrast in some centres
The contrast causes chemical irritation of the bronchial mucosa, leading to exacerbation of symptoms - particularly important in patients with pre-existing infection.
Indications
Primary Indications:
- Bronchiectasis - the classical indication; to determine extent and localization of disease before surgical resection. Most disease affects the left lower lobe and lingula.
- Lung abscess - to delineate the cavity and draining bronchus
- Congenital anomalies of the bronchial tree - sequestration, bronchial atresia
- Suspected bronchial obstruction or stenosis - where bronchoscopy is not possible (e.g., lumen too narrow for bronchoscope)
- Tracheomalacia / bronchomalacia - when endoscopic access is limited
- Bronchobiliary fistula or bronchopleural fistula - to define the communication
- Foreign body localization - pre-operative planning
- Unresolved or recurrent pneumonia - to identify underlying structural abnormality
- Preoperative evaluation before pulmonary resection
- Selective bronchography - as an adjunct to fiberoptic bronchoscopy for segmental assessment
Contraindications
Absolute Contraindications:
- Known iodine hypersensitivity (iodism)
- Active haemoptysis - risk of flooding the airways
- Severely compromised respiratory reserve (cannot tolerate even unilateral lung filling)
Relative Contraindications (K.J. Lee's Essential Otolaryngology):
- Acute infection / active pulmonary tuberculosis
- Acute asthmatic attack (bronchospasm risk)
- Acute cardiac failure
- Pregnancy (radiation and contrast exposure)
- Recent myocardial infarction
- Severe pulmonary hypertension
Pre-Procedure Preparation
(Pye's Surgical Handicraft, 22nd Edition)
- Iodine sensitivity test must be performed and excluded before the procedure
- Physiotherapy - postural drainage and percussion to clear accumulated secretions before the procedure; reduces risk of mixing contrast with pus
- Fasting - patient kept nil-by-mouth
- Sputum culture and sensitivity - to assess baseline infection
- Respiratory function tests (spirometry) - baseline assessment
- Sedation / antibiotic prophylaxis as needed
- If children require the procedure - general anaesthesia, and only one lung at a time should be studied
Technique
Anaesthesia:
- Preferred: Local anaesthesia - so the patient can cough vigorously and help distribute contrast and clear it post-procedure
- General anaesthesia - used in children; only one lung per session
Steps:
- Topical anaesthesia of the larynx, trachea, and bronchi using 4% lignocaine (lidocaine) spray
- Patient positioned appropriately (supine, then tilted to fill dependent bronchi)
- Catheter introduction - a gum elastic catheter (Metras catheter) or cricothyroid injection needle is passed:
- Via translaryngeal (transglottic) route - catheter passed through the glottis
- Via cricothyroid puncture - needle introduced through cricothyroid membrane directly into trachea
- Via fiberoptic bronchoscope - for selective bronchography (most modern approach)
- Via nasotracheal route - in children
- Contrast injection: 10-20 mL of contrast introduced slowly under fluoroscopic guidance; patient is tilted in different positions (Trendelenburg, lateral decubitus) to fill specific bronchopulmonary segments
- Radiographs taken immediately in AP, lateral, and oblique projections
- Patient encouraged to cough forcibly to clear contrast
- Physiotherapy post-procedure to assist clearance
Findings on Bronchogram
The bronchogram outlines:
- Trachea, main bronchi, lobar, segmental, and sub-segmental bronchi
- Normal branching pattern ("tree in leaf" appearance)
Pathological findings:
| Condition | Bronchographic Appearance |
|---|---|
| Bronchiectasis (cylindrical) | Uniform dilatation of bronchi; tram-lining |
| Bronchiectasis (saccular/cystic) | Sac-like pooling of contrast; "bunch of grapes" |
| Bronchiectasis (varicose) | Irregular beaded dilatation |
| Bronchial obstruction | Abrupt cut-off of contrast column |
| Bronchial stenosis | Narrowing of contrast-filled lumen |
| Tracheomalacia | Collapse of airway on expiration |
| Bronchopleural fistula | Contrast leaks into pleural space |
In bronchiectasis, the most common location is the left lower lobe and lingula - important surgical landmark for resection planning.
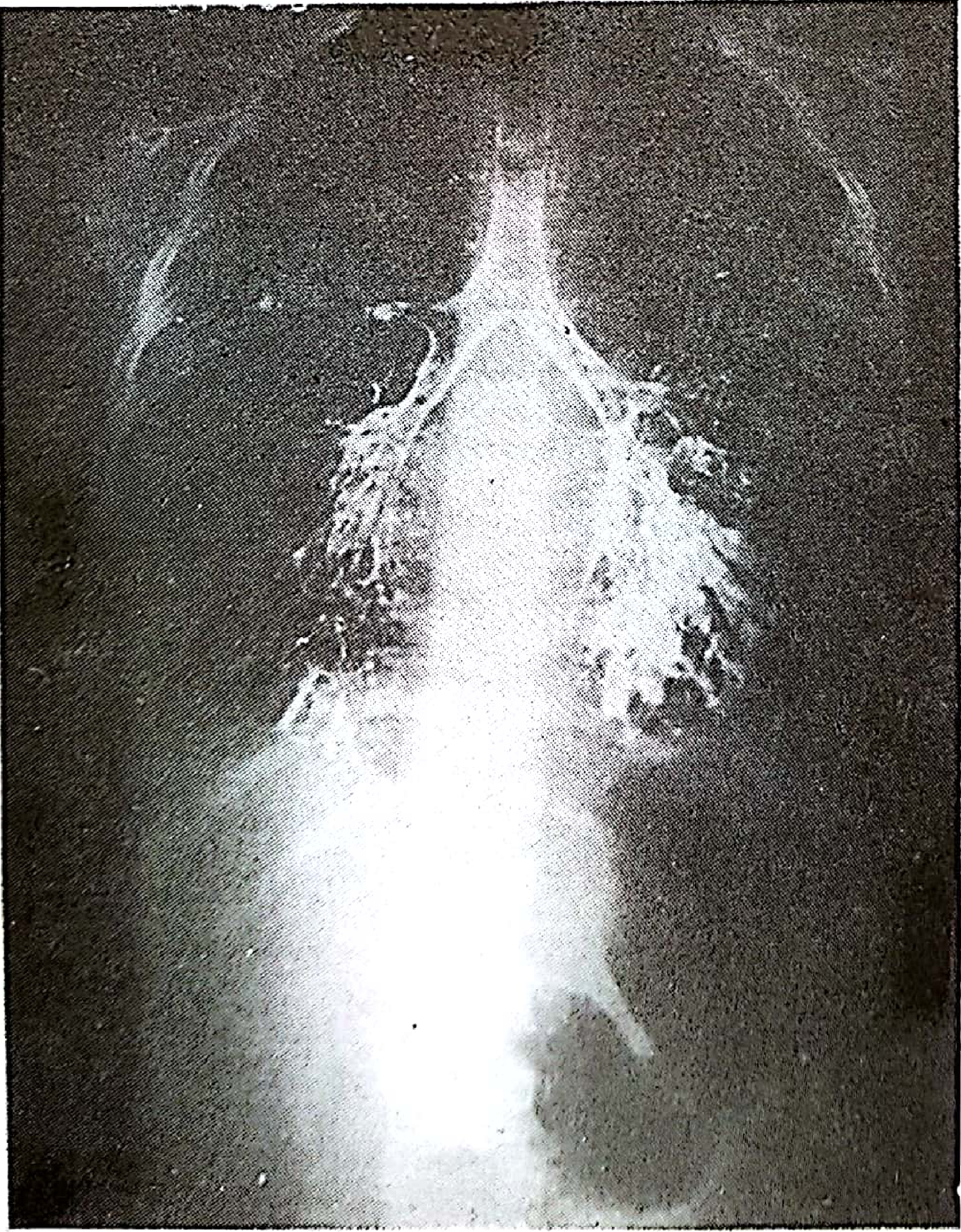
Bronchogram showing contrast outlining the bronchi - the pooling of contrast in dilated sac-like structures is characteristic of saccular bronchiectasis (Pye's Surgical Handicraft)
Complications
- Bronchospasm / laryngospasm - due to contrast irritation
- Exacerbation of pulmonary infection - chemical irritation precipitates acute flare
- Aspiration pneumonitis - if contrast floods alveoli
- Iodine hypersensitivity reaction - mild (urticaria) to severe (anaphylaxis)
- Respiratory failure - if bilateral filling done simultaneously in compromised patient
- Vagal reaction / vasovagal syncope - during catheter manipulation
- Haemoptysis - mucosal trauma from catheter
- Retention of oily contrast - granuloma formation (with oil-based agents)
Current Status / What Has Replaced It
| Investigation | Advantage Over Bronchography |
|---|---|
| HRCT chest | Non-invasive, no contrast into airways, equally sensitive for bronchiectasis |
| CT chest (3D multiplanar) | Virtual bronchoscopy, identifies stenosis and compression |
| Fiberoptic bronchoscopy | Direct visualization, allows biopsy and BAL |
| Selective bronchography via bronchoscope | Still used in special circumstances (tracheomalacia, fistula) |
According to Murray & Nadel: "In patients with suspected bronchiectasis, HRCT and CT are as sensitive and are safer, more easily obtained, and much more pleasant to undergo than bronchography."
Summary Table for Quick Recall
| Feature | Detail |
|---|---|
| Definition | Radiological outlining of bronchial tree with contrast |
| Contrast used | Propyliodone (Dionosil), iodized oils |
| Primary indication | Bronchiectasis (pre-surgical assessment) |
| Key contraindication | Iodine allergy, active haemoptysis |
| Common site of disease | Left lower lobe + lingula |
| Pre-op prep | Clear secretions by physiotherapy, exclude iodine sensitivity |
| Children | GA; one lung at a time |
| Adults | Local anaesthesia preferred |
| Replaced by | HRCT, fiberoptic bronchoscopy |
Sources:
- Pye's Surgical Handicraft, 22nd Edition - Bronchography section
- Murray & Nadel's Textbook of Respiratory Medicine - Chapter on Imaging
- K.J. Lee's Essential Otolaryngology - Contraindications and ENT perspective
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery - Tracheal stenosis evaluation
This is a shared conversation. Sign in to Orris to start your own chat.