Best DPP 4 inhibitor?
Reading File
Searching PubMed
"DPP-4 inhibitor" comparison cardiovascular outcomes
Finding Sources
Searching PubMed
"DPP-4 inhibitor" comparison efficacy safety
Finding Sources
Searching PubMed
gliptin DPP4 inhibitor diabetes type 2
Reading File
Reading File
Reading File
Reading File
Here is a thorough, side-by-side breakdown of all clinically used DPP-4 inhibitors (gliptins):
DPP-4 Inhibitors: Class Overview
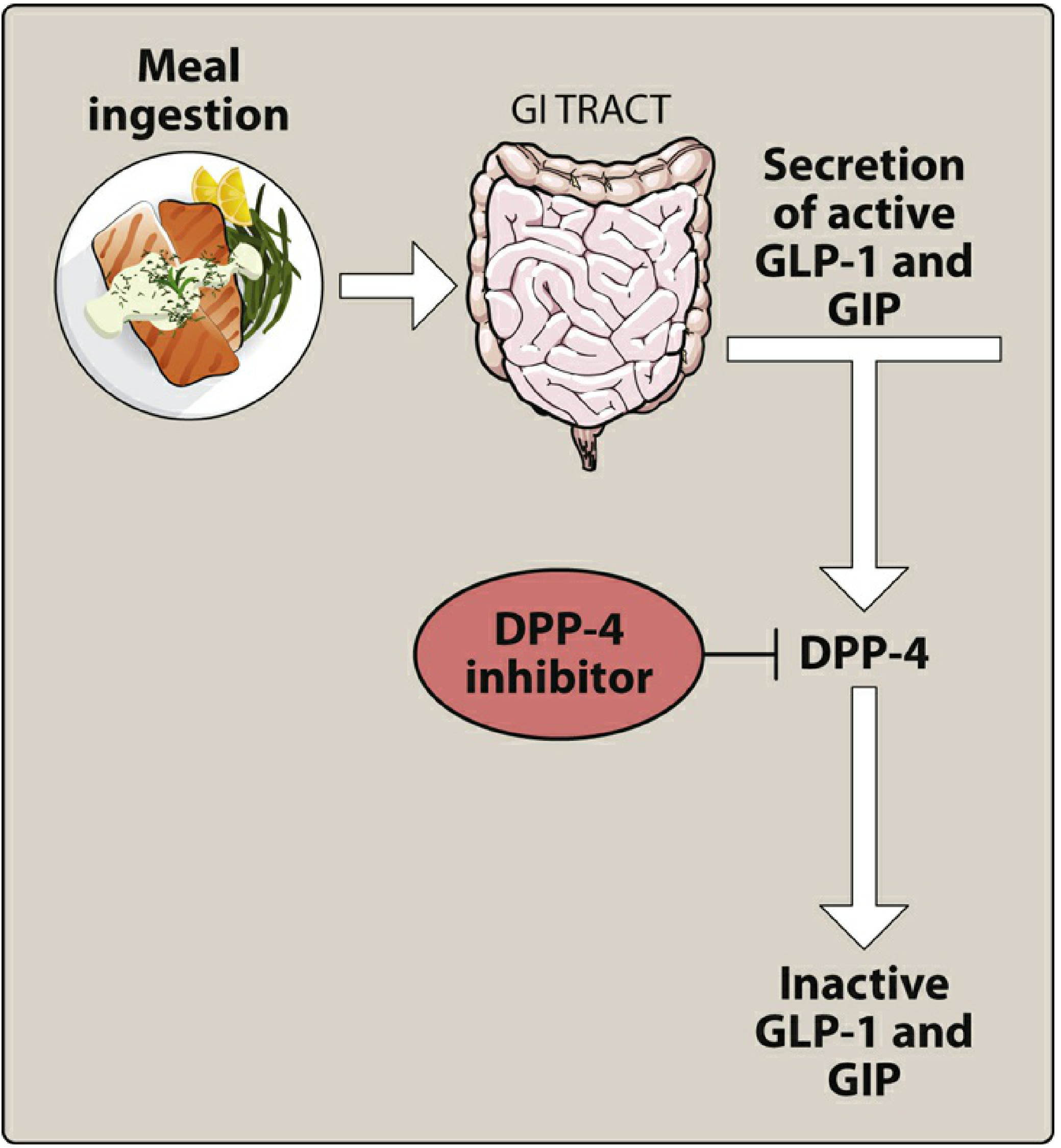
DPP-4 (dipeptidyl peptidase-4) inhibitors work by blocking the enzyme that inactivates GLP-1 and GIP, thereby boosting glucose-dependent insulin secretion and suppressing glucagon. As monotherapy, they reduce HbA1c by 0.4-0.8% - modest but with a clean safety profile. They are weight-neutral and carry low hypoglycemia risk.
Head-to-Head Comparison
| Drug | Brand | Dose | Renal Adjustment | CYP3A4 Risk | CV Safety | Key Notes |
|---|---|---|---|---|---|---|
| Sitagliptin | Januvia | 100 mg/day | Yes | No | TECOS: HR ~1.0 (neutral) | Most studied; first-in-class; widely used |
| Linagliptin | Tradjenta | 5 mg/day | No | No | Neutral (CARMELINA) | Hepatobiliary clearance; preferred in CKD/ESRD |
| Saxagliptin | Onglyza | 5 mg/day | Yes | Yes (reduce to 2.5 mg with strong CYP3A4 inhibitors) | SAVOR-TIMI 53: increased HHF risk | Use with caution in HF or HF risk |
| Alogliptin | Nesina | 25 mg/day | Yes | No | EXAMINE: HR ~1.0 (neutral) | Competitive inhibitor; less commonly used in US |
| Vildagliptin | Galvus | 50 mg OD or BD | Yes | No | Not studied in large CV trial | Available in EU, not FDA-approved in US; covalent binder |
Which Is "Best" by Clinical Scenario?
Renal impairment (CKD, ESRD): Linagliptin is the clear winner - it is the only DPP-4 inhibitor requiring no dose adjustment whatsoever, because it is cleared through the hepatobiliary system rather than the kidneys. All others need dose reduction.
- Comprehensive Clinical Nephrology, 7th Edition confirms: "No dose adjustment is required for linagliptin."
General use / most evidence: Sitagliptin is the most extensively studied, has the largest body of real-world data, and is the most prescribed worldwide. TECOS trial showed cardiovascular neutrality (HR ~1.0 for MACE). It is the default choice for most clinicians.
Heart failure risk present: Avoid saxagliptin (SAVOR-TIMI 53 showed a statistically significant increase in heart failure hospitalizations). Sitagliptin or linagliptin are preferable. TECOS with sitagliptin showed no increase in HHF.
Drug interactions (strong CYP3A4 inhibitors co-prescribed): Avoid saxagliptin or reduce dose to 2.5 mg. All other gliptins lack this interaction.
EU-only practice: Vildagliptin is an additional option (50 mg once or twice daily), also a covalent DPP-4 binder like saxagliptin, but not FDA-approved in the US.
Shared Class Adverse Effects
- Nasopharyngitis and headache (most common, generally mild)
- Rare but serious: pancreatitis, severe hypersensitivity reactions
- Rare: severe and disabling joint pain (FDA warning for the whole class)
- No weight gain, low hypoglycemia risk when used without secretagogues
Bottom Line
There is no universally "best" gliptin - the choice depends on context:
- Linagliptin if CKD or renal impairment
- Sitagliptin for most other patients (most data, no HHF signal)
- Avoid saxagliptin in patients with or at risk for heart failure, and watch for CYP3A4 drug interactions
Recent evidence note (2024 ACP): A 2024 ACP systematic review and guideline in Annals of Internal Medicine (PMID 38639549) compared newer diabetes pharmacotherapy across drug classes. DPP-4 inhibitors remain a valid option but SGLT-2 inhibitors and GLP-1 agonists are now preferred in patients with established cardiovascular disease or high CV risk, given their demonstrated cardiovascular and renal benefits beyond glucose lowering.
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics | Lippincott Illustrated Reviews: Pharmacology | Comprehensive Clinical Nephrology, 7th Edition
How do DPP-4 inhibitors compare to SGLT-2 inhibitors and GLP-1 agonists?
Finding Sources
Searching PubMed
"DPP-4 inhibitor" OR "SGLT2 inhibitor" OR "GLP-1" type 2 diabetes comparison cardiovascular
Finding Sources
Finding Sources
Reading Article
PMID: 41454299
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have strong textbook and recent trial data to give a thorough, structured comparison. Here it is:
DPP-4 Inhibitors vs. SGLT-2 Inhibitors vs. GLP-1 Agonists
These three classes represent the three "newer" pillars of type 2 diabetes pharmacotherapy after metformin, but they differ profoundly in potency, mechanism, and clinical benefits beyond glucose lowering.
Side-by-Side Comparison Table
| Feature | DPP-4 Inhibitors | SGLT-2 Inhibitors | GLP-1 Receptor Agonists |
|---|---|---|---|
| Examples | Sitagliptin, linagliptin, saxagliptin | Empagliflozin, canagliflozin, dapagliflozin | Semaglutide, liraglutide, dulaglutide, exenatide |
| Route | Oral | Oral | Subcutaneous (mostly); oral semaglutide available |
| Mechanism | Blocks DPP-4 → ↑ active GLP-1/GIP | Blocks renal SGLT2 → urinary glucose excretion | Mimics GLP-1 → ↑ insulin, ↓ glucagon, ↓ gastric emptying, ↑ satiety |
| HbA1c reduction | ~0.4-0.8% | ~0.5-1.0% | ~0.8-2.0% (highest of the three) |
| Weight effect | Neutral (no change) | Modest loss: 2-5 kg | Significant loss: 3-6+ kg (semaglutide 10-15%+ in obesity trials) |
| Hypoglycemia risk | Low | Low | Low (unless combined with sulfonylurea/insulin) |
| BP effect | Neutral | ↓ systolic 3-5 mmHg (osmotic diuresis) | Modest ↓ |
| CV mortality | Neutral (TECOS, EXAMINE) | ✅ Reduced (EMPA-REG OUTCOME, CANVAS) | ✅ Reduced (LEADER, SUSTAIN-6, REWIND) |
| Heart failure hospitalization | Saxagliptin ↑ risk (SAVOR-TIMI 53); others neutral | ✅ Strongly reduced (HR ~0.68) | Modest reduction |
| Renal protection | None proven | ✅ Strong (CREDENCE, DAPA-CKD, EMPA-KIDNEY) | Reduces albuminuria; less robust than SGLT-2i |
| Atherosclerotic events (MACE) | Neutral | ✅ Reduced | ✅ Reduced (GLP-1 nominally better for MACE: HR 0.82 vs. 0.89) |
| Adverse effects | Nasopharyngitis, rare pancreatitis, joint pain | UTI/genital fungal infections, DKA risk, volume depletion, amputation risk (canagliflozin) | Nausea, vomiting, diarrhea (especially early); rare pancreatitis; thyroid C-cell risk (rodents) |
| Renal dosing | Most need adjustment; linagliptin does not | Not for glycemic control if eGFR <45; contraindicated <30 | Generally safe; avoid exenatide if eGFR <30 |
| Cost | Moderate | Moderate-high | High (especially injectable agents) |
What the Latest Evidence Says (2025)
A 2025 systematic review and meta-analysis across 12 RCTs (n = 99,261) directly comparing SGLT-2 inhibitors vs. GLP-1 agonists vs. placebo found (PMID 41454299):
- Both SGLT-2i and GLP-1RA significantly reduced MACE vs. placebo
- GLP-1RA showed nominally greater MACE reduction (HR 0.82) vs. SGLT-2i (HR 0.89)
- SGLT-2i were far superior for heart failure hospitalization (HR 0.68) and composite renal outcomes (HR 0.69)
- GLP-1RA excelled for atherosclerotic events and weight loss
- The two classes are complementary, not interchangeable; DPP-4 inhibitors are not in this conversation for CV/renal benefit
How to Choose in Practice
Patient has established ASCVD (prior MI, stroke)?
→ GLP-1 agonist first (stronger atherosclerotic MACE benefit; semaglutide/liraglutide/dulaglutide FDA-approved for this indication)
Patient has heart failure (HFrEF) or high HF risk?
→ SGLT-2 inhibitor (dapagliflozin/empagliflozin; HR 0.68 for HHF; also approved in HF without diabetes)
Patient has CKD / proteinuria?
→ SGLT-2 inhibitor (CREDENCE with canagliflozin, DAPA-CKD, EMPA-KIDNEY; benefits seen even without diabetes)
Patient needs significant weight loss?
→ GLP-1 agonist (especially semaglutide; injectable 2.4 mg = ~15% body weight loss in STEP trials)
Patient wants lowest complexity / cost / pill burden with no major comorbidities?
→ DPP-4 inhibitor (especially sitagliptin or linagliptin) - well-tolerated, oral, once-daily, low hypoglycemia risk, but no CV/renal added benefit
Both ASCVD + HF + CKD?
→ Combine SGLT-2i + GLP-1 agonist (complementary mechanisms, additive benefits)
The Bottom Line
DPP-4 inhibitors are the "safe and easy" option - excellent tolerability, no weight gain, once-daily oral dosing - but offer no proven cardiovascular or renal protection. SGLT-2 inhibitors and GLP-1 agonists have transformed T2DM management precisely because they do what DPP-4 inhibitors cannot: reduce CV death, prevent heart failure hospitalizations, and slow CKD progression. Current guidelines (ADA, ACP) now recommend SGLT-2 inhibitors or GLP-1 agonists as preferred add-ons when a patient has ASCVD, CKD, or HF - DPP-4 inhibitors are reserved for those who need additional glucose lowering without these comorbidities.
Sources: Katzung's Basic and Clinical Pharmacology 16th Ed. | Lippincott Illustrated Reviews: Pharmacology | Ahmed et al., BMC Cardiovasc Disord 2025 (PMID 41454299)
This is a shared conversation. Sign in to Orris to start your own chat.