Intra uterine fetal death
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive coverage of IUFD/stillbirth from Creasy & Resnik's Maternal-Fetal Medicine. Here is a full, structured clinical summary:
Intrauterine Fetal Death (IUFD) / Stillbirth
Definition
| Term | Gestational Age |
|---|---|
| Fetal death (early) | 10–19⁶⁄₇ weeks |
| Stillbirth | ≥20 weeks gestation |
| Late stillbirth (ICD coding) | ≥22 weeks |
| WHO / international definition | ≥28 weeks (for global comparisons) |
Epidemiology
- Global: ~2.6 million stillbirths (≥28 weeks) occur annually; 98% in low- and middle-income countries.
- United States: 1 in 165 pregnancies; ~21,500/year; rate of 5.7 per 1,000 births.
- The US stillbirth rate declined only minimally from 2006–2019 (6.05 → 5.7/1,000), compared to 6.8%/year decline in some European countries.
- Early stillbirths (20–27 weeks): 2.98/1,000; Late (≥28 weeks): 2.73/1,000.
- Racial disparity: Non-Hispanic Black women have a 2.2× higher rate (10.41 vs. 4.71/1,000) than non-Hispanic White women — partly explained by obstetric complications and infection, but multifactorial and not fully explained.
Risk Factors
| Category | Details |
|---|---|
| Maternal age | J-shaped curve; lowest risk 30–34 years. Age ≥35 is independent risk factor. Risk at 37–41 weeks: 1/382 (age 35–39), 1/267 (age ≥40) |
| Parity | Nulliparity and grand multiparity both increase risk |
| Obesity | BMI >30 independently increases risk |
| Diabetes | Particularly if poorly controlled |
| Hypertension | Especially if severe/uncontrolled |
| Multiple gestation | Especially second twin and MCMA twins |
| Prior stillbirth | Significant recurrence risk |
| Smoking, alcohol, drugs | Modifiable risk factors |
| Antiphospholipid syndrome | Thrombosis and placental insufficiency |
| Fetal growth restriction (FGR) | Major independent risk factor |
Causes (Pathogenesis)
Based on the SCRN (Stillbirth Collaborative Research Network) INCODE analysis of 512 stillbirths with complete evaluation:
| Cause | Proportion |
|---|---|
| Obstetric conditions (abruption, preterm labor, PPROM) | 29.3% |
| Placental abnormalities | 23.6% |
| Fetal genetic/structural abnormalities | 13.7% |
| Infection | 12.9% |
| Umbilical cord abnormalities | 10.4% |
| Hypertensive disorders | 9.2% |
| Other maternal medical conditions | 7.8% |
| No cause despite complete evaluation | ~25% |
Key Causes in Detail
1. Infection (~10–20% in developed countries; higher in developing countries)
- Ascending (e.g., Group B Streptococcus, E. coli) → chorioamnionitis, funisitis
- Hematogenous (e.g., Listeria, CMV, parvovirus B19, syphilis, malaria)
- Mechanisms: direct fetal infection, placental dysfunction, severe maternal illness, preterm labor
2. Placental causes
- Abruption, infarction, velamentous cord insertion, vasa previa, massive fetomaternal hemorrhage, chronic villitis
3. Fetal genetic/structural anomalies
- Chromosomal abnormalities found in 6–13% of tested stillbirths; >20% when structural anomalies or FGR present
- Microarray detects additional copy-number variants missed by standard karyotype
4. Umbilical cord abnormalities
- Cord prolapse, true knot, nuchal cord with compression, cord thrombosis
5. Fetal growth restriction
- Placental insufficiency → fetal hypoxia
6. Intrapartum stillbirth
- Developed countries: ~1/1,000 births; developing countries: ~7.3/1,000 (up to 20–25/1,000 in parts of Africa/Asia)
- Causes: shoulder dystocia, malpresentation, cord prolapse, birth trauma, abruption, uterine rupture
Classification Systems
- Over 80 classification systems have been proposed — no global consensus
- INCODE (Stillbirth Collaborative Research Network): assigns "probable," "possible," or "condition present" levels of certainty
- ICD-PM (WHO ICD-10 based): preferred in low-resource settings
Diagnosis & Evaluation
Initial Steps (All Cases)
- Thorough medical and obstetric history (Box 42.1)
- Placental pathology (gross + histologic) — single most useful test; should be done in all cases
- Fetal autopsy — recommended in all cases; provides cause of death in >30%
Yield of Additional Tests (SCRN Data)
| Test | Diagnostic yield |
|---|---|
| Genetic testing (karyotype/microarray) | 11.9% |
| Antiphospholipid antibodies | 11.1% |
| Fetomaternal hemorrhage (Kleihauer-Betke) | 6.4% |
| Glucose screen | 1.6% |
| Parvovirus | 0.4% |
| Syphilis | 0.2% |
Clinical Scenario-Based Approach
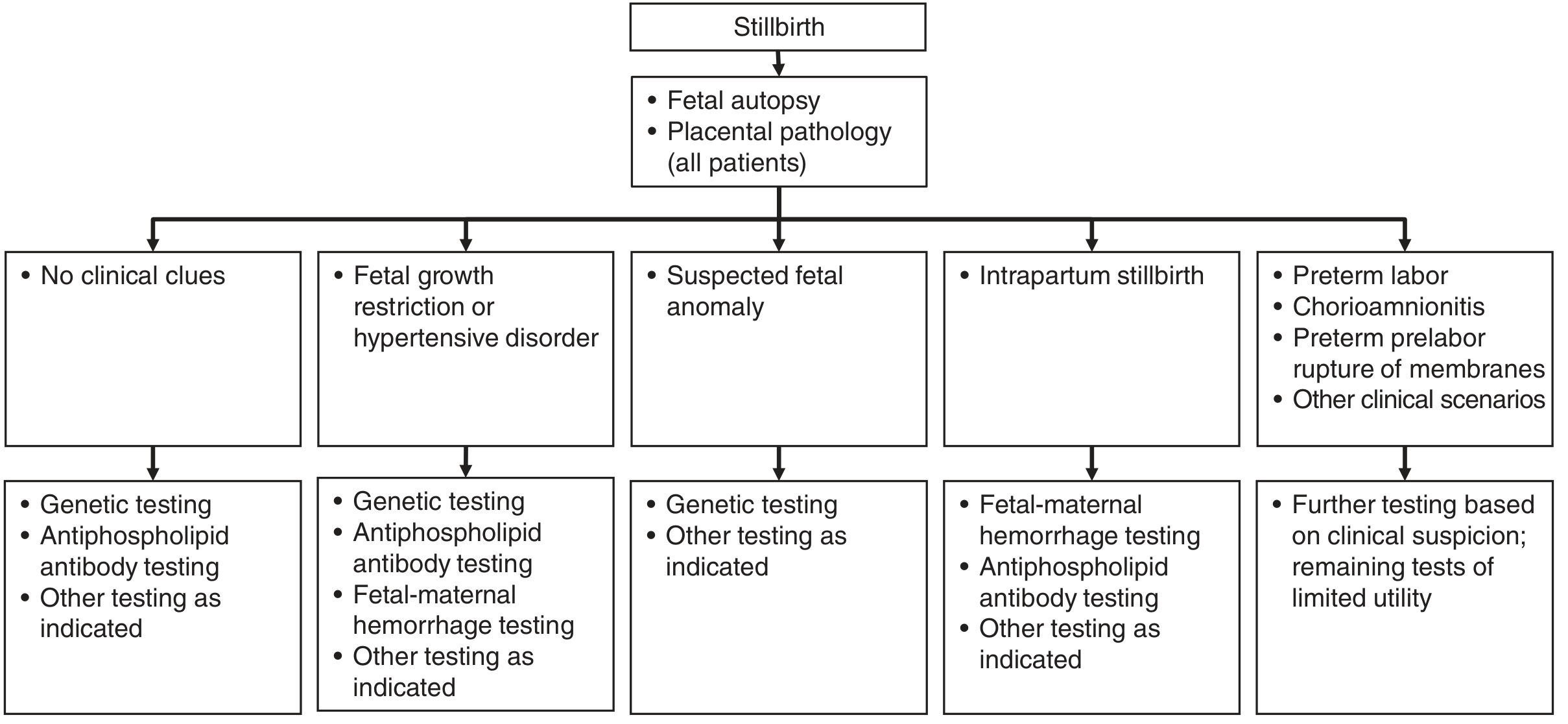
Figure 42.2 — Evaluation of stillbirth. All patients undergo fetal autopsy + placental pathology; additional tests guided by clinical scenario — Creasy & Resnik's Maternal-Fetal Medicine
Management / Delivery
Timing
- No medical urgency for immediate delivery
- 80–90% of women enter spontaneous labor within 2 weeks
- Consumptive coagulopathy (DIC) from tissue factor release: occurs in ~3–4% after 4–8 weeks; risk increases with abruption or uterine perforation
- Coagulation screen (fibrinogen, platelets, PT, aPTT) required before neuraxial anesthesia
Mode of Delivery — by Gestational Age
Second trimester (13–22 weeks uterine size): D&E preferred
- Lower complication rate (4%) vs. induction of labor (29%) when performed by experienced providers
- Limitation: limits quality of perinatal autopsy
- Admit: CBC, type & screen; doxycycline 200 mg PO 1 hour pre-procedure; misoprostol 200 μg vaginally 4 hours prior OR laminaria; RhD immune globulin if Rh-negative
Induction of Labor Protocol
- Uterus <28 weeks: Misoprostol 200–400 μg vaginally or orally q4h
- Uterus ≥28 weeks: Misoprostol 25–50 μg vaginally/orally q4h OR oxytocin infusion
- Consider fibrinogen level if fetal death >4 weeks
- Allow spontaneous placental delivery (avoid cord traction) to reduce retained placenta
- Epidural, IV narcotics (PCA), or intermittent dosing for analgesia
Previous Cesarean Section
- Prior low-transverse: use misoprostol for <28 weeks; oxytocin + cervical Foley for ≥28 weeks
- Prior classic incision: repeat cesarean delivery is appropriate
Bereavement
- Parents encouraged to see, hold, and spend time with baby
- Offer keepsake items (photos, hand/footprints)
- Consider postpartum care on a non-maternity ward
- Bereavement services referral
- Follow-up visit at 2–6 weeks
Screening & Prediction
| Marker | Significance |
|---|---|
| Low PAPP-A (<5th percentile at 10 weeks) | 9.2× increased risk of all-cause stillbirth; 46× for placental cause |
| Elevated maternal serum AFP (>2.5 MoM) | Associated with placentation defects and stillbirth |
| Elevated β-hCG | 1.4× increased risk per 1 MoM increase |
| Low PAPP-A + high AFP combined | OR 36.7 for antepartum stillbirth |
| Uterine artery Doppler (22–24 weeks, mean PI >90th percentile) | 5.5× risk of placental stillbirth |
Prevention
- Most stillbirths occur in pregnancies with no identifiable prior risk factors — population-wide screening is needed
- Modifiable risk factors: smoking cessation, weight reduction (BMI >30), treating diabetes/hypertension optimally, avoiding illicit substances
- Antepartum fetal surveillance for high-risk pregnancies
- Fetal movement counting — awareness of decreased movements prompts evaluation
Management of Subsequent Pregnancy (Box 42.3)
| Trimester | Key Actions |
|---|---|
| Preconception | Evaluate prior stillbirth, counseling, thrombophilia testing, diabetes screen, weight optimization |
| 1st trimester | Dating US, PAPP-A/hCG/NT or cfDNA screening |
| 2nd trimester | Anatomic survey at 18–20 weeks, AFP if needed |
| 3rd trimester | Serial growth US from 28 weeks, fetal movement counting, antepartum surveillance from 32 weeks (or 1–2 weeks before previous stillbirth GA) |
| Delivery | Planned delivery at 39⁰⁄₇ weeks (or earlier based on comorbidities/anxiety) |
Source: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice — Chapter 41 (Fetal Death 10–20 weeks) & Chapter 42 (Stillbirth), 9th Edition.
For ms level
Here is a focused, MS-level (medical student / postgraduate exam) summary of IUFD:
Intrauterine Fetal Death (IUFD)
Definition
- Death of a fetus at or after 20 weeks of gestation (some definitions: ≥28 weeks for international comparisons)
- Before 20 weeks → called abortion/miscarriage
- Also called stillbirth
Etiology (Causes) — "ABCDE" Framework
| Category | Examples |
|---|---|
| A — Antepartum/Maternal | Diabetes, hypertension, SLE, antiphospholipid syndrome, hypothyroidism, anaemia, infections (TORCH, syphilis, parvovirus B19) |
| B — Baby (Fetal) | Chromosomal anomalies (trisomy 13, 18, 21), structural defects, FGR, Rh isoimmunization, hydrops fetalis |
| C — Cord/Placenta | Cord prolapse, true knot, abruption, placenta previa, velamentous insertion, vasa previa, circumvallate placenta |
| D — Delivery complications | Obstructed labour, shoulder dystocia, uterine rupture, intrapartum hypoxia |
| E — Unexplained | ~25% even after complete evaluation |
Diagnosis
Symptoms
- Absent fetal movements (most common presenting complaint)
- Disappearance of pregnancy symptoms (breast tenderness, nausea)
- No fetal heart sounds on auscultation
Investigations
| Investigation | Finding |
|---|---|
| USG (confirmatory) | Absent fetal cardiac activity, collapsed cranium |
| Spalding's sign (X-ray) | Overlapping of fetal skull bones (after 4–5 days) |
| Robert's sign | Gas in fetal cardiovascular system (early sign on X-ray) |
| Hyperflexion of spine | X-ray finding — "crowding" of vertebrae |
| Spalding sign on USG | Skull bone collapse |
Gold standard for confirmation: Ultrasound — absence of fetal cardiac activity
Complications (Maternal)
1. DIC / Coagulopathy ⚠️ (Most feared)
- Dead fetus releases thromboplastin (tissue factor) → activates extrinsic coagulation cascade → consumptive coagulopathy
- Occurs after 4+ weeks of fetal retention
- Risk: ~3–4% at 4–8 weeks; increases with abruption
- Monitor: Fibrinogen (earliest to fall), PT, aPTT, platelets
- Fibrinogen <150 mg/dL = treat before delivery
2. Infection / Sepsis
- From ascending organisms; especially with PPROM
3. Psychological morbidity
- Grief, depression, post-traumatic stress
Management
Step 1 — Confirm diagnosis
- USG: absent cardiac activity
Step 2 — Evaluate
- Thorough history + examination
- Placental pathology + fetal autopsy — most useful investigations
- Coagulation screen (fibrinogen, PT, aPTT, platelets) — especially if dead >4 weeks
- Kleihauer-Betke test (fetomaternal hemorrhage)
- Antiphospholipid antibodies
- Karyotype/chromosomal microarray
- Infection screen (TORCH, parvovirus, syphilis)
- Blood glucose, thyroid function
Step 3 — Deliver
There is no medical emergency for immediate delivery unless coagulopathy, sepsis, or maternal indication exists. 80–90% of women go into spontaneous labour within 2 weeks.
| Gestation | Method |
|---|---|
| <13 weeks | Suction evacuation (MVA) |
| 13–22 weeks | D&E (preferred) OR misoprostol 200–400 μg vaginally/orally q4h |
| >28 weeks | Induction with misoprostol 25–50 μg q4h OR oxytocin infusion |
| Previous LSCS, uterus ≥28 weeks | Oxytocin + cervical Foley; avoid high-dose misoprostol |
| Previous classical CS | Repeat caesarean section |
- Administer anti-D immunoglobulin to all Rh-negative mothers
- If fibrinogen <150 mg/dL → correct coagulopathy before induction
X-ray Signs of IUFD (Classical Exam Points)
| Sign | Description |
|---|---|
| Spalding's sign | Overlapping of skull bones due to brain liquefaction |
| Robert's sign | Gas in fetal great vessels and heart |
| Hyperflexion of spine | Exaggerated curvature |
| Crowding of ribs | Loss of normal thoracic contour |
| Abnormal posture | Hyperextended or flexed limbs |
Bereavement Care
- Allow parents to see and hold the baby
- Photographs, handprints, footprints
- Refer to bereavement/psychological support
- Follow-up at 2–6 weeks post-delivery
Subsequent Pregnancy Counselling
- Evaluate and treat cause before next pregnancy
- Serial growth ultrasounds from 28 weeks
- Antepartum fetal surveillance from 32 weeks (or 1–2 weeks before previous stillbirth GA)
- Fetal movement counting from 28 weeks
- Planned delivery at 39 weeks (or earlier if indicated)
- Risk of recurrence depends on cause; overall ~7–10× higher background risk
Key High-Yield Points for Exams
| Point | Detail |
|---|---|
| Most common presenting symptom | Absent fetal movements |
| Confirmatory investigation | Ultrasound (absent cardiac activity) |
| Most feared maternal complication | DIC (coagulopathy) |
| Earliest biochemical sign of DIC | Falling fibrinogen |
| When does DIC risk rise? | After 4 weeks of fetal retention |
| Best single investigation to find cause | Placental pathology + fetal autopsy |
| Most common cause in developed countries | Obstetric complications (abruption, preterm labour) |
| Unexplained stillbirths | ~25% even after complete workup |
| Rh-negative mother | Always give anti-D |
| Drug of choice for induction <28 weeks | Misoprostol 200–400 μg vaginally |
This is a shared conversation. Sign in to Orris to start your own chat.