Hey, explain me about the concept of fibrinolysis, you know. It is the final step where the clot is dissolved when the vessel got healed, right? So, this concept, explain me and what all are the testables through this concept in the USMLE Step 1. I want a topper-like notes, like useful for step 1.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have all the high-yield information needed from multiple authoritative sources. Let me compile the comprehensive USMLE Step 1 notes on fibrinolysis.
Fibrinolysis — USMLE Step 1 High-Yield Notes
The Big Picture
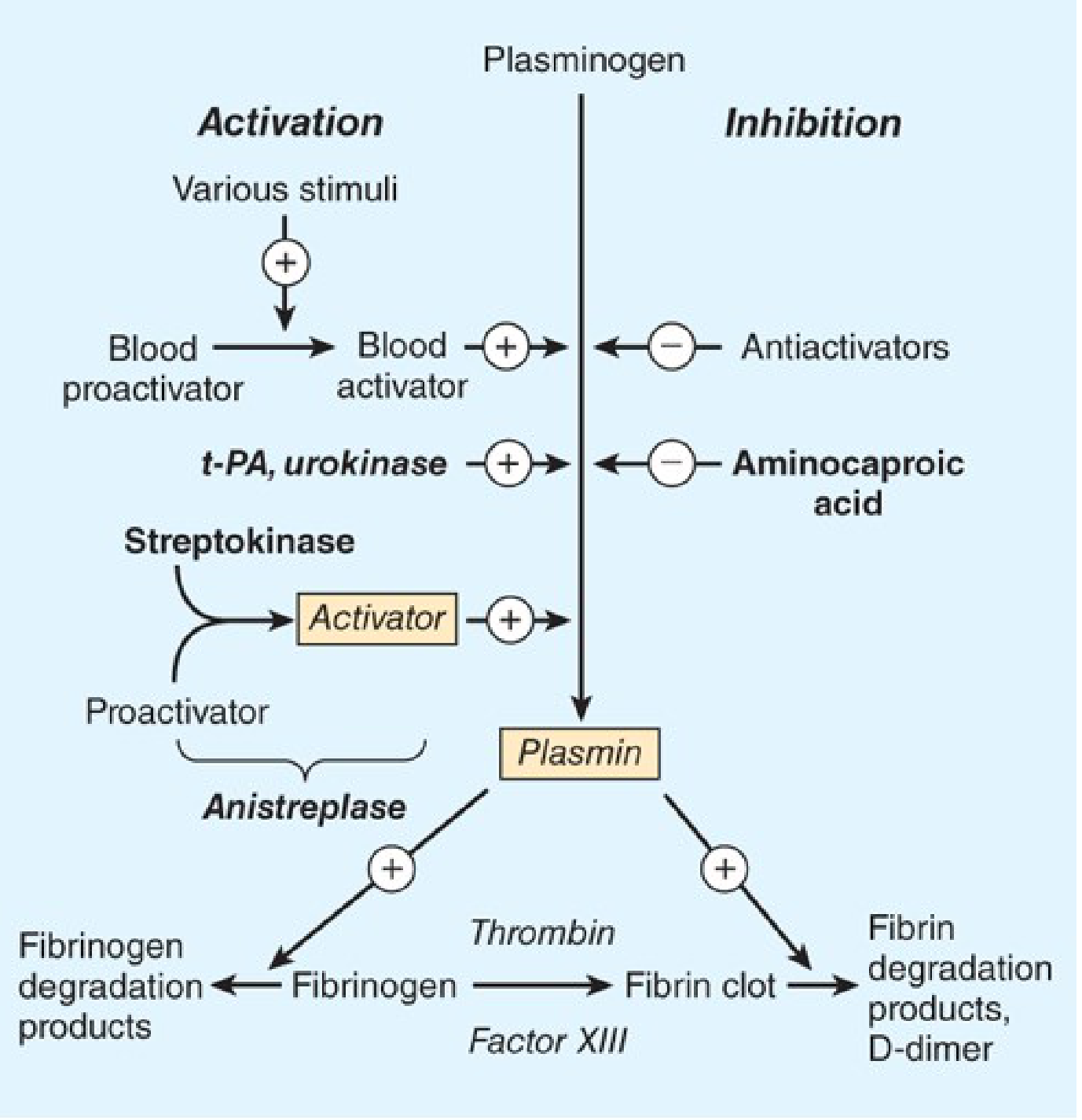
Fibrinolysis is the enzymatic dissolution of a fibrin clot after tissue repair. It is the counter-regulatory system to coagulation — just as thrombin is the master enzyme of coagulation, plasmin is the master enzyme of fibrinolysis. The two systems are activated in parallel during vascular injury, keeping each other in balance.
Your correction is partially right — fibrinolysis is activated during clot formation (not only after healing), to limit clot growth from the start, and then continues to dissolve the clot as the wound heals.
Core Pathway (The One Diagram You Must Know)
Step-by-Step Mechanism
1. Plasminogen → Plasmin (The Key Conversion)
| Component | Role |
|---|---|
| Plasminogen | Inactive zymogen (precursor), circulates in blood |
| tPA (tissue plasminogen activator) | Primary physiologic activator; released by endothelial cells |
| uPA (urokinase-type PA) | Second activator; mainly drives extravascular fibrinolysis (inflammatory contexts) |
| Plasmin | Active serine protease; digests fibrin |
- tPA cleaves the Arg560–Val561 bond of plasminogen → generates active two-chain plasmin
- Endothelial cells synthesize and release both tPA and uPA
- tPA predominates under most physiologic conditions
- The catalytic efficiency of tPA activation of plasminogen increases >300-fold in the presence of fibrin — this is why plasmin is generated on the clot surface, not diffusely in blood
— Goodman & Gilman's Pharmacological Basis of Therapeutics; Katzung's Basic and Clinical Pharmacology 16e
2. Why Is Fibrinolysis "Fibrin-Specific"? (Kringle Domains — HIGH YIELD)
- Plasminogen and plasmin both have kringle domains — loop-like structures near their amino termini that bind to exposed lysine residues on fibrin
- This anchors both plasminogen and tPA onto the clot surface → forms a ternary complex (fibrin + plasminogen + tPA) → massively accelerates plasmin generation locally
- As plasmin begins degrading fibrin, it exposes new carboxy-terminal lysine residues → even more plasminogen and tPA binding → positive feedback loop of clot dissolution
- Plasmin bound to fibrin is protected from circulating α₂-antiplasmin (its inhibitor) because the kringle domains are occupied
- Result: plasmin acts only on the clot, not on circulating fibrinogen — "fibrin-specific"
⚠️ This specificity is lost at pharmacologic doses of tPA (alteplase) — too much plasmin overwhelms the inhibitory controls → systemic lytic state → bleeding risk
— Goodman & Gilman's; Harrison's Internal Medicine 22e
3. What Does Plasmin Actually Degrade?
| Substrate | Product | Clinical Significance |
|---|---|---|
| Cross-linked fibrin (clot) | D-dimer + fibrin degradation products (FDPs) | D-dimer is diagnostic for DVT/PE, DIC |
| Fibrinogen (in systemic lysis) | Fibrinogen degradation products (FDPs) | Seen in DIC, thrombolytic overdose |
| Coagulation factors (at high doses) | Degraded V, VIII | Bleeding risk with thrombolytics |
- D-dimer is produced only when plasmin acts on cross-linked fibrin (Factor XIIIa-stabilized clot) — not from fibrinogen alone. This is its diagnostic value.
— Harrison's Internal Medicine 22e
Regulatory Inhibitors (The Brakes on the System)
| Inhibitor | What It Inhibits | Notes |
|---|---|---|
| PAI-1 (plasminogen activator inhibitor-1) | tPA and uPA | Major inhibitor of plasminogen activators; synthesized by endothelial cells; rapidly clears tPA from blood |
| PAI-2 | tPA and uPA (lesser extent) | Prominent in pregnancy |
| α₂-antiplasmin (α₂-plasmin inhibitor) | Plasmin | Major inhibitor of free plasmin; binds kringle domain 1 then blocks active site; overwhelmed by therapeutic tPA doses |
| TAFI (Thrombin-Activatable Fibrinolysis Inhibitor) | Removes C-terminal lysines from fibrin | Limits plasminogen/tPA binding; thrombin + thrombomodulin activates it |
| Factor XIIIa | Indirectly (cross-links α₂-antiplasmin to fibrin) | Prevents premature clot lysis |
- PAI-1 is the key reason tPA exerts little effect on circulating plasminogen in the absence of fibrin — tPA is rapidly neutralized before it can act systemically
- α₂-antiplasmin is the main circulating safety net that mops up any plasmin that escapes the clot
— Goodman & Gilman's; Katzung 16e; Harrison's 22e
Pharmacology (Thrombolytics/Fibrinolytics) — HIGH YIELD
Drugs That ACTIVATE Fibrinolysis
| Drug | Mechanism | Fibrin-Specific? | Notes |
|---|---|---|---|
| Alteplase (tPA, rt-PA) | Recombinant tPA → activates plasminogen | Yes (at physiologic doses) | Drug of choice for ischemic stroke (within 4.5 hrs), STEMI if no PCI available |
| Reteplase (rPA) | Recombinant tPA variant | Yes | Double bolus IV; used in STEMI |
| Tenecteplase (TNK-tPA) | Engineered tPA variant | Yes | Single weight-based bolus; longer half-life; used in STEMI |
| Streptokinase | Bacterial protein; binds plasminogen → forms an activator complex | No (non-fibrin-specific) | Systemic lytic state; antigenic (↑ antibodies, allergic reactions); cannot re-use |
| Urokinase (uPA) | Directly converts plasminogen → plasmin | No | Used for catheter-directed thrombolysis |
| Anistreplase | Streptokinase + plasminogen complex | No | Older agent |
Drug That INHIBITS Fibrinolysis
| Drug | Mechanism | Use |
|---|---|---|
| Aminocaproic acid (ε-aminocaproic acid) | Lysine analogue → blocks kringle domains → prevents plasminogen/tPA binding to fibrin | Hemostasis after surgery, hemophilia bleeds, post-tonsillectomy bleeding |
| Tranexamic acid (TXA) | Same mechanism as aminocaproic acid (lysine analogue) | Trauma, surgical bleeding, heavy menstrual bleeding |
Mnemonic: Aminocaproic acid = Anti-fibrinolytic — it occupies the lysine-binding sites so plasminogen cannot attach to fibrin.
— Katzung 16e; Lippincott Pharmacology; Goodman & Gilman's
Contraindications to Thrombolytics (Step 1 Favorite)
Absolute contraindications:
- Prior intracranial hemorrhage (any time)
- Ischemic stroke within 3 months (except acute stroke being treated, <4.5 hrs)
- Suspected aortic dissection
- Active internal bleeding (not menses)
- Significant closed-head trauma/facial trauma within 3 months
- SBP >180 or DBP >110 at presentation (severe uncontrolled hypertension)
Clinical Scenarios and Lab Findings
D-Dimer
- Elevated D-dimer = evidence of fibrin clot formation AND lysis → used to rule OUT DVT/PE (high sensitivity, low specificity)
- D-dimer is elevated in: DVT/PE, DIC, post-surgery, pregnancy, malignancy, infection
- D-dimer is NOT elevated with just thrombocytopenia or with fibrinogen degradation (needs cross-linked fibrin)
DIC (Disseminated Intravascular Coagulation)
- Pathologic activation of BOTH coagulation AND fibrinolysis simultaneously
- Labs: ↑ PT, ↑ aPTT, ↑ D-dimer, ↑ FDPs, ↓ fibrinogen, ↓ platelets
- Causes: sepsis, trauma, obstetric emergencies (abruptio placentae, amniotic fluid embolism), malignancy
- Treat the underlying cause — DIC is often fatal if the underlying process cannot be controlled
Bleeding Complication of Thrombolytics
- At pharmacologic doses, plasmin degrades Factors V and VIII in addition to fibrin → impairs thrombin generation → bleeding
- Also dissolves fibrin in hemostatic plugs (normal wound seals) → more bleeding risk
- Hemorrhage is the major adverse effect of all fibrinolytic drugs
USMLE Step 1 High-Yield Testable Points Summary
| Concept | Testable Fact |
|---|---|
| Plasminogen activator | tPA (physiologic); released by endothelial cells |
| Kringle domains | Bind lysine on fibrin → clot specificity → protected from α₂-antiplasmin |
| Major inhibitor of plasmin | α₂-antiplasmin |
| Major inhibitor of tPA | PAI-1 |
| D-dimer | Product of cross-linked fibrin degradation; rules out DVT/PE |
| FDPs without D-dimer | From fibrinogen degradation only (not cross-linked fibrin) |
| DIC labs | ↑ PT, ↑ aPTT, ↑ D-dimer, ↓ fibrinogen, ↓ platelets, schistocytes on smear |
| Streptokinase | Antigenic, non-fibrin-specific, cannot re-administer |
| Aminocaproic acid / TXA | Lysine analogues → antifibrinolytic |
| Alteplase contraindications | Hemorrhagic stroke ever; ischemic stroke <3 months; aortic dissection |
| Fibrin specificity at high tPA doses | LOST → systemic lytic state → bleeding |
| Positive feedback in lysis | Partial fibrin degradation exposes more lysine residues → more plasmin binding |
| TAFI | Thrombin-activatable fibrinolysis inhibitor; removes lysines → slows lysis |
| Factor XIIIa role | Cross-links fibrin AND cross-links α₂-antiplasmin to fibrin → protects clot from early lysis |
Memory Map
VESSEL INJURY
↓
Coagulation cascade → Thrombin → Fibrin clot (Factor XIIIa cross-links it)
↓ (simultaneously)
Endothelial cells release tPA
↓
tPA + Plasminogen bind to FIBRIN (via kringle-lysine interaction)
→ Ternary complex → Plasmin (locally generated, fibrin-specific)
↓
Plasmin degrades cross-linked fibrin → D-DIMER + FDPs
↓
Clot dissolves; vessel patent again
INHIBITORS:
PAI-1 → blocks tPA/uPA
α₂-antiplasmin → blocks free plasmin
TAFI → removes lysines from fibrin (limits plasmin binding)
Aminocaproic acid / TXA → occupy lysine binding sites (drugs)
Sources: Katzung's Basic and Clinical Pharmacology 16e | Goodman & Gilman's Pharmacological Basis of Therapeutics | Harrison's Principles of Internal Medicine 22e | Lippincott Illustrated Reviews: Pharmacology | Medical Physiology (Boron & Boulpaep)
Step 1 topper like hy and short including everything
Fibrinolysis — Step 1 Topper Notes ⚡
THE MASTER EQUATION
Plasminogen ──[tPA / uPA]──► PLASMIN ──► Fibrin ──► D-dimer + FDPs
▲
(on clot surface only)
KEY PLAYERS — One Line Each
| Player | What It Is | One-liner |
|---|---|---|
| Plasminogen | Inactive zymogen | Circulates in blood; activated ON the fibrin clot |
| tPA | Tissue plasminogen activator | Made by endothelium; main physiologic activator |
| uPA (urokinase) | Urokinase-type PA | Extravascular fibrinolysis; inflammatory states |
| Plasmin | Active serine protease | The actual "clot dissolver" |
| PAI-1 | Plasminogen activator inhibitor-1 | Blocks tPA/uPA → made by endothelium |
| α₂-antiplasmin | Plasmin inhibitor | Destroys free plasmin; can't reach clot-bound plasmin |
| TAFI | Thrombin-activatable fibrinolysis inhibitor | Removes lysines from fibrin → slows lysis |
WHY PLASMIN IS CLOT-SPECIFIC (Most Tested Concept)
- Plasminogen and tPA both have kringle domains → bind lysine residues on fibrin
- Forms ternary complex: Fibrin + Plasminogen + tPA → plasmin generated locally
- Plasmin on fibrin surface = kringle domains occupied = α₂-antiplasmin CANNOT bind = protected
- Partial digestion of fibrin exposes MORE C-terminal lysines → positive feedback → faster lysis
- Free plasmin (escapes clot) → instantly killed by α₂-antiplasmin
High-dose tPA (pharmacologic) → overwhelms PAI-1 and α₂-antiplasmin → clot specificity LOST → systemic lysis → BLEEDING
PRODUCTS OF FIBRINOLYSIS
| Product | Source | Significance |
|---|---|---|
| D-dimer | Plasmin on cross-linked fibrin (Factor XIIIa-stabilized) | Diagnoses active clot formation + lysis (DVT/PE, DIC) |
| FDPs (fibrin/fibrinogen degradation products) | Plasmin on fibrin OR fibrinogen | Less specific; elevated in DIC, liver disease |
D-dimer requires cross-linked fibrin → needs Factor XIIIa to have acted first → not elevated from fibrinogen breakdown alone
DRUGS — THE WHOLE TABLE
🔴 Pro-Fibrinolytic (Thrombolytics) — "Clot Busters"
| Drug | Mechanism | Fibrin-Specific? | Key Facts |
|---|---|---|---|
| Alteplase (tPA) | Recombinant tPA | ✅ Yes | Stroke (≤4.5 hrs), STEMI, massive PE |
| Reteplase | tPA variant | ✅ Yes | Double IV bolus; STEMI |
| Tenecteplase (TNK) | Engineered tPA | ✅ Yes | Single weight-based bolus; STEMI |
| Streptokinase | Bacterial → forms plasminogen-activator complex | ❌ No | Antigenic → allergic rxn; can't re-use (antibodies); systemic lysis |
| Urokinase | Directly converts plasminogen → plasmin | ❌ No | Catheter-directed thrombolysis |
🟢 Anti-Fibrinolytic (Hemostatics) — "Clot Protectors"
| Drug | Mechanism | Uses |
|---|---|---|
| Aminocaproic acid | Lysine analogue → blocks kringle domains → no plasminogen binding to fibrin | Post-op bleeding, hemophilia, tonsillectomy |
| Tranexamic acid (TXA) | Same mechanism | Trauma, surgery, heavy periods |
Both are competitive inhibitors of plasminogen/plasmin binding to fibrin — they occupy the lysine-binding sites
CONTRAINDICATIONS TO THROMBOLYTICS (Absolute)
- Prior intracranial hemorrhage (ever)
- Ischemic stroke within 3 months (except: treating acute stroke <4.5 hrs)
- Suspected aortic dissection
- Active internal bleeding (not menses)
- Severe uncontrolled HTN (SBP >180 / DBP >110)
- Recent significant head/face trauma (<3 months)
DIC — THE PATHOLOGIC EXTREME
Both coagulation AND fibrinolysis go haywire simultaneously
| Lab | Value | Why |
|---|---|---|
| PT / aPTT | ↑ | Clotting factors consumed |
| Fibrinogen | ↓ | Consumed + degraded by plasmin |
| Platelets | ↓ | Consumed in microthrombi |
| D-dimer | ↑↑ | Massive clot lysis |
| FDPs | ↑↑ | Fibrin/fibrinogen degradation |
| Smear | Schistocytes | RBCs sheared by fibrin strands |
Causes: Sepsis, trauma, obstetric emergencies (abruption, amniotic fluid embolism, retained products), malignancy (esp. AML-M3 / APL)
Treatment: Treat underlying cause — if uncontrolled, often fatal
D-DIMER CLINICAL USE
| Situation | D-dimer |
|---|---|
| Suspected DVT/PE (low pre-test probability) | If negative → rules OUT (high sensitivity) |
| DIC | ↑↑ (with ↓ fibrinogen, ↓ platelets) |
| Post-surgery / pregnancy / cancer | False positive (↑ but not diagnostic) |
| Fibrinogenolysis only (no cross-linked fibrin) | Normal D-dimer, elevated FDPs only |
RAPID-FIRE HY FACTS
- tPA made by → endothelial cells
- tPA cleared rapidly from blood by → PAI-1
- Fibrin specificity mechanism → kringle domains + lysine residues
- tPA efficiency on fibrin vs. alone → >300× faster on fibrin surface
- Factor XIIIa does TWO things: ① cross-links fibrin strands ② cross-links α₂-antiplasmin onto fibrin (prevents early lysis)
- TAFI activated by → thrombin + thrombomodulin complex
- Streptokinase → antigenic → cannot re-administer (neutralizing antibodies)
- Bleeding from thrombolytics → plasmin degrades Factors V and VIII → impairs future thrombin generation
- Aminocaproic acid = anti-fibrinolytic → lysine analogue (same as TXA)
- D-dimer = specifically from Factor XIIIa cross-linked fibrin degradation
ONE-LINER SUMMARY
tPA (from endothelium) converts plasminogen → plasmin on fibrin surface (via kringle-lysine binding); plasmin digests cross-linked fibrin → D-dimer; free plasmin is killed by α₂-antiplasmin; tPA is killed by PAI-1; drugs mimicking tPA = thrombolytics; drugs blocking lysine binding = antifibrinolytics.

Can you make a time table daily to solve questions of complete u world starting from today till june 30
Asking for Preferences
Here's your complete plan:
UWorld Step 1 Complete Timetable
May 19 → June 30 | Sundays Off
The Numbers
| Stat | Value |
|---|---|
| Total questions | 3,658 |
| Total days (May 19 – Jun 30) | 43 days |
| Sundays off (May 25, Jun 1, 8, 15, 22, 29) | 6 days |
| Active study days | 37 days |
| Questions/day needed | 3658 ÷ 37 = ~99 Qs/day |
| Target: 100 Qs/day | Finishes entire bank with buffer |
Daily Schedule (8–9 hrs/day)
| Time | Activity | Duration |
|---|---|---|
| 8:00–8:30 AM | Morning review — yesterday's marked/incorrect | 30 min |
| 8:30–10:30 AM | Block 1 — 40 Qs (Timed) | 2 hrs |
| 10:30–11:30 AM | Review Block 1 explanations deeply | 1 hr |
| 11:30–1:30 PM | Block 2 — 40 Qs (Timed) | 2 hrs |
| 1:30–2:30 PM | Lunch break | 1 hr |
| 2:30–3:30 PM | Review Block 2 explanations | 1 hr |
| 3:30–4:30 PM | Block 3 — 20 Qs (Tutor mode) | 1 hr |
| 4:30–5:15 PM | Review Block 3 + make notes | 45 min |
| 5:15–6:00 PM | Rapid-fire revision — FA/Sketchy/Anki on today's topics | 45 min |
80 Qs timed + 20 Qs tutor = 100 Qs/day with full review each day
Subject Allocation by Week
Based on your qbank breakdown (heaviest subjects first):
| Week | Dates | Subjects | Total Qs |
|---|---|---|---|
| Week 1 | May 19–24 | Pathology (819 Qs) — Part 1 | ~600 |
| Week 2 | May 26–31 | Pathology finish (219) + Pharmacology start (331) | ~550 |
| Week 3 | Jun 2–7 | Pharmacology finish (219) + Pathophysiology start (231) | ~450 |
| Week 4 | Jun 9–14 | Pathophysiology finish (257) + Anatomy (308) | ~565 |
| Week 5 | Jun 16–21 | Microbiology (348) + Behavioral Science start (154) | ~500 |
| Week 6 | Jun 23–28 | Behavioral Sci finish (100) + Physiology (268) + Biochemistry (159) | ~527 |
| Final push | Jun 29–30 | Immunology (132) + Biostatistics (121) + Genetics (107) + Embryology (75) + Histology (29) | ~464 |
Week-by-Week Daily Breakdown
WEEK 1 — May 19–24 | Pathology
| Day | Date | Focus | Qs |
|---|---|---|---|
| Mon | May 19 | Pathology — Cell injury, Inflammation, Neoplasia | 100 |
| Tue | May 20 | Pathology — Cardiovascular | 100 |
| Wed | May 21 | Pathology — Pulmonary | 100 |
| Thu | May 22 | Pathology — GI + Hepatobiliary | 100 |
| Fri | May 23 | Pathology — Renal + Endocrine | 100 |
| Sat | May 24 | Pathology — Heme/Onc + MSK | 100 |
| Sun | May 25 | OFF | — |
WEEK 2 — May 26–31 | Pathology + Pharmacology
| Day | Date | Focus | Qs |
|---|---|---|---|
| Mon | May 26 | Pathology — Neuro + Repro (finish) | 100 |
| Tue | May 27 | Pathology — Remaining + Review weak areas | 119 |
| Wed | May 28 | Pharmacology — Autonomic + CNS drugs | 100 |
| Thu | May 29 | Pharmacology — Cardiovascular drugs | 100 |
| Fri | May 30 | Pharmacology — Antimicrobials | 100 |
| Sat | May 31 | Pharmacology — Endocrine + Chemo drugs | 100 |
| Sun | Jun 1 | OFF | — |
WEEK 3 — Jun 2–7 | Pharmacology + Pathophysiology
| Day | Date | Focus | Qs |
|---|---|---|---|
| Mon | Jun 2 | Pharmacology — Remaining (finish) | ~150 |
| Tue | Jun 3 | Pathophysiology — Cardio | 100 |
| Wed | Jun 4 | Pathophysiology — Pulm + Renal | 100 |
| Thu | Jun 5 | Pathophysiology — GI + Endocrine | 100 |
| Fri | Jun 6 | Pathophysiology — Neuro + Heme | 100 |
| Sat | Jun 7 | Pathophysiology — Remaining (finish) | ~88 |
| Sun | Jun 8 | OFF | — |
WEEK 4 — Jun 9–14 | Anatomy
| Day | Date | Focus | Qs |
|---|---|---|---|
| Mon | Jun 9 | Anatomy — Head & Neck | 100 |
| Tue | Jun 10 | Anatomy — Upper limb + Lower limb | 100 |
| Wed | Jun 11 | Anatomy — Thorax + Abdomen | 100 |
| Thu | Jun 12 | Anatomy — finish (8 Qs leftover) + Microbiology — Bacteria | 100 |
| Fri | Jun 13 | Microbiology — Viruses | 100 |
| Sat | Jun 14 | Microbiology — Fungi + Parasites | 100 |
| Sun | Jun 15 | OFF | — |
WEEK 5 — Jun 16–21 | Microbiology + Behavioral Science
| Day | Date | Focus | Qs |
|---|---|---|---|
| Mon | Jun 16 | Microbiology — Remaining + Behavioral Sci start | 100 |
| Tue | Jun 17 | Behavioral Science — Epidemiology + Ethics | 100 |
| Wed | Jun 18 | Behavioral Science — finish + Physiology start | 100 |
| Thu | Jun 19 | Physiology — Cardio + Pulm | 100 |
| Fri | Jun 20 | Physiology — Renal + GI | 100 |
| Sat | Jun 21 | Physiology — Neuro + Endocrine (finish) | 68 |
| Sun | Jun 22 | OFF | — |
WEEK 6 — Jun 23–28 | Biochemistry + Small Subjects
| Day | Date | Focus | Qs |
|---|---|---|---|
| Mon | Jun 23 | Biochemistry — Metabolism + Molecular bio | 100 |
| Tue | Jun 24 | Biochemistry — finish (59) + Immunology start | 100 |
| Wed | Jun 25 | Immunology — finish (32 leftover) + Biostatistics | 100 |
| Thu | Jun 26 | Biostatistics — finish (21) + Genetics | 100 |
| Fri | Jun 27 | Genetics — finish (7) + Embryology | 100 |
| Sat | Jun 28 | Embryology — finish + Histology (29) + Spillover/Review | ~54 |
| Sun | Jun 29 | OFF | — |
FINAL 1 DAY — Jun 30
| Day | Date | Activity |
|---|---|---|
| Mon | Jun 30 | Full comprehensive review — All marked questions + weak subjects. Do a mixed 40Q timed block to simulate real test feel. |
Rules for Review (Non-Negotiable)
- Never skip explanations — read every explanation, even for correct answers
- Mark aggressively — if you're not 100% sure, mark it
- Wrong answer notebook — one line per wrong answer: "Q topic → Why I was wrong → Correct concept"
- Saturday = light day — fewer new Qs, more review of the week's weak spots
- Sunday = full off — your brain needs it
Weekly Check-In Targets
| End of Week | Qs Completed | % Done |
|---|---|---|
| May 24 | ~600 | 16% |
| May 31 | ~1,219 | 33% |
| Jun 7 | ~1,757 | 48% |
| Jun 14 | ~2,357 | 64% |
| Jun 21 | ~2,957 | 81% |
| Jun 28 | ~3,511 | 96% |
| Jun 30 | 3,658 | 100% ✅ |
Bottom line: 100 Qs/day, 6 days/week, 37 active days = entire UWorld done with 1 full review day left. Stick to the 80 timed + 20 tutor split so you build speed AND understand concepts simultaneously.
Wait today is april 13 2026 make from tomorrow
UWorld Step 1 Complete Timetable
April 14 → June 30, 2026 | Sundays Off
The Numbers
| Stat | Value |
|---|---|
| Total questions | 3,658 |
| Total days (Apr 14 – Jun 30) | 78 days |
| Sundays off (Apr 19, 26, May 3, 10, 17, 24, 31, Jun 7, 14, 21, 28) | 11 days |
| Active study days | 67 days |
| Questions/day needed | 3658 ÷ 67 = ~55 Qs/day |
| Target: 60 Qs/day | Finishes bank with ~5 days buffer for revision |
Great news — you have a very comfortable timeline. 60 Qs/day is very doable in 8–9 hrs, leaving significant time for deep review, notes, and Anki/FA alongside each subject.
Daily Schedule (8–9 hrs/day)
| Time | Activity | Duration |
|---|---|---|
| 8:00–8:30 AM | Morning review — previous day's marked/incorrect Qs | 30 min |
| 8:30–10:00 AM | Block 1 — 40 Qs (Timed mode) | 1.5 hrs |
| 10:00–11:15 AM | Deep review of Block 1 explanations + notes | 1 hr 15 min |
| 11:15–11:30 AM | Short break | 15 min |
| 11:30–12:30 PM | Block 2 — 20 Qs (Tutor mode) | 1 hr |
| 12:30–1:30 PM | Lunch break | 1 hr |
| 1:30–2:30 PM | Review Block 2 + update wrong answer log | 1 hr |
| 2:30–4:30 PM | First Aid / Sketchy / Pathoma — parallel reading of today's subject | 2 hrs |
| 4:30–5:30 PM | Anki / Flashcard review (new + due cards) | 1 hr |
| 5:30–6:00 PM | Plan tomorrow, review weak points | 30 min |
40 timed + 20 tutor = 60 Qs/day with full deep review + resource reading every day
Subject Allocation Plan
| Subject | Qs | Days Needed @ 60/day |
|---|---|---|
| Pathology | 819 | ~14 days |
| Pharmacology | 550 | ~9 days |
| Pathophysiology | 488 | ~8 days |
| Anatomy | 308 | ~5 days |
| Microbiology | 348 | ~6 days |
| Behavioral Science | 254 | ~4 days |
| Physiology | 268 | ~4 days |
| Biochemistry | 159 | ~3 days |
| Immunology | 132 | ~2 days |
| Biostatistics | 121 | ~2 days |
| Genetics | 107 | ~2 days |
| Embryology | 75 | ~1 day |
| Histology | 29 | ~1 day |
| TOTAL | 3,658 | ~61 days → done by ~Jun 18 |
Leaves Jun 19–30 (12 days) purely for revision of wrong/marked questions
Full Week-by-Week Schedule
WEEK 1 — Apr 14–19 | Pathology: Foundations
| Day | Date | Subject Focus | Qs |
|---|---|---|---|
| Mon | Apr 14 | Pathology — Cell injury, Apoptosis, Necrosis | 60 |
| Tue | Apr 15 | Pathology — Inflammation (acute + chronic) | 60 |
| Wed | Apr 16 | Pathology — Tissue repair, Wound healing | 60 |
| Thu | Apr 17 | Pathology — Neoplasia (basics, carcinogenesis) | 60 |
| Fri | Apr 18 | Pathology — Hematologic neoplasms (leukemia/lymphoma) | 60 |
| Sat | Apr 19 | Pathology — Vascular pathology | 60 |
| Sun | Apr 19 | OFF ☀️ | — |
WEEK 2 — Apr 21–26 | Pathology: Organ Systems
| Day | Date | Subject Focus | Qs |
|---|---|---|---|
| Mon | Apr 21 | Pathology — Cardiovascular | 60 |
| Tue | Apr 22 | Pathology — Pulmonary | 60 |
| Wed | Apr 23 | Pathology — GI (esophagus → small bowel) | 60 |
| Thu | Apr 24 | Pathology — GI (colon, liver, pancreas) | 60 |
| Fri | Apr 25 | Pathology — Renal | 60 |
| Sat | Apr 26 | Pathology — Endocrine | 60 |
| Sun | Apr 26 | OFF ☀️ | — |
WEEK 3 — Apr 28 – May 3 | Pathology: Finish + Pharmacology Start
| Day | Date | Subject Focus | Qs |
|---|---|---|---|
| Mon | Apr 28 | Pathology — MSK + Derm | 60 |
| Tue | Apr 29 | Pathology — Neuro + Repro (finish Pathology ✅) | 60 |
| Wed | Apr 30 | Pharmacology — Autonomic nervous system | 60 |
| Thu | May 1 | Pharmacology — CNS drugs (antidepressants, antipsychotics) | 60 |
| Fri | May 2 | Pharmacology — CNS drugs (antiepileptics, anesthesia, opioids) | 60 |
| Sat | May 3 | Pharmacology — Cardiovascular drugs (antihypertensives, antiarrhythmics) | 60 |
| Sun | May 3 | OFF ☀️ | — |
WEEK 4 — May 5–10 | Pharmacology: Finish
| Day | Date | Subject Focus | Qs |
|---|---|---|---|
| Mon | May 5 | Pharmacology — Cardiovascular (statins, anticoagulants, antiplatelets) | 60 |
| Tue | May 6 | Pharmacology — Antimicrobials Part 1 (cell wall, protein synthesis) | 60 |
| Wed | May 7 | Pharmacology — Antimicrobials Part 2 (quinolones, antifungals, antivirals) | 60 |
| Thu | May 8 | Pharmacology — Endocrine drugs (insulin, thyroid, steroids) | 60 |
| Fri | May 9 | Pharmacology — Chemotherapy + Immunosuppressants (finish Pharmacology ✅) | 60 |
| Sat | May 10 | Pathophysiology — Cardiovascular | 60 |
| Sun | May 10 | OFF ☀️ | — |
WEEK 5 — May 12–17 | Pathophysiology
| Day | Date | Subject Focus | Qs |
|---|---|---|---|
| Mon | May 12 | Pathophysiology — Pulmonary | 60 |
| Tue | May 13 | Pathophysiology — Renal (AKI, CKD, acid-base) | 60 |
| Wed | May 14 | Pathophysiology — GI + Hepatobiliary | 60 |
| Thu | May 15 | Pathophysiology — Endocrine | 60 |
| Fri | May 16 | Pathophysiology — Hematology (anemias, coagulation) | 60 |
| Sat | May 17 | Pathophysiology — Neuro + Repro (finish Pathophysiology ✅) | 60 |
| Sun | May 17 | OFF ☀️ | — |
WEEK 6 — May 19–24 | Microbiology
| Day | Date | Subject Focus | Qs |
|---|---|---|---|
| Mon | May 19 | Microbiology — Bacteriology Part 1 (Gram +ve) | 60 |
| Tue | May 20 | Microbiology — Bacteriology Part 2 (Gram –ve, atypicals) | 60 |
| Wed | May 21 | Microbiology — Virology (DNA viruses, RNA viruses) | 60 |
| Thu | May 22 | Microbiology — Mycology + Parasitology | 60 |
| Fri | May 23 | Microbiology — Remaining (finish Microbiology ✅) | 60 |
| Sat | May 24 | Anatomy — Head & Neck | 60 |
| Sun | May 24 | OFF ☀️ | — |
WEEK 7 — May 26–31 | Anatomy + Behavioral Science
| Day | Date | Subject Focus | Qs |
|---|---|---|---|
| Mon | May 26 | Anatomy — Upper limb + Lower limb | 60 |
| Tue | May 27 | Anatomy — Thorax + Abdomen | 60 |
| Wed | May 28 | Anatomy — Neuroanatomy (finish Anatomy ✅) | 60 |
| Thu | May 29 | Behavioral Science — Biostatistics/Epidemiology within BS | 60 |
| Fri | May 30 | Behavioral Science — Ethics, Development, Psychiatry | 60 |
| Sat | May 31 | Behavioral Science — finish (finish Behavioral Science ✅) | 60 |
| Sun | May 31 | OFF ☀️ | — |
WEEK 8 — Jun 2–7 | Physiology + Biochemistry
| Day | Date | Subject Focus | Qs |
|---|---|---|---|
| Mon | Jun 2 | Physiology — Cardiovascular + Pulmonary | 60 |
| Tue | Jun 3 | Physiology — Renal + GI | 60 |
| Wed | Jun 4 | Physiology — Neuro + Endocrine (finish Physiology ✅) | 60 |
| Thu | Jun 5 | Biochemistry — Metabolism (glycolysis, TCA, FA) | 60 |
| Fri | Jun 6 | Biochemistry — Molecular biology + Nutrition (finish Biochemistry ✅) | 60 |
| Sat | Jun 7 | Immunology — Innate + Adaptive immunity | 60 |
| Sun | Jun 7 | OFF ☀️ | — |
WEEK 9 — Jun 9–14 | Small Subjects: Finish All
| Day | Date | Subject Focus | Qs |
|---|---|---|---|
| Mon | Jun 9 | Immunology — finish (finish Immunology ✅) | 72 |
| Tue | Jun 10 | Biostatistics — Full (finish Biostatistics ✅) | 60 |
| Wed | Jun 11 | Genetics — Full (finish Genetics ✅) | 60 |
| Thu | Jun 12 | Embryology + Histology — Full (finish both ✅) | 60 |
| Fri | Jun 13 | 🎉 QBANK COMPLETE — Mixed weak subject review block | 60 |
| Sat | Jun 14 | Revision Day 1 — All Incorrect Qs (252 total) Part 1 | 60 |
| Sun | Jun 14 | OFF ☀️ | — |
WEEK 10 — Jun 16–21 | Pure Revision
| Day | Date | Activity | Qs |
|---|---|---|---|
| Mon | Jun 16 | Revision — Incorrect Qs Part 2 | 60 |
| Tue | Jun 17 | Revision — All Marked Qs (65 total) + Omitted Part 1 | 60 |
| Wed | Jun 18 | Revision — Omitted Qs Part 2 (259 total) | 60 |
| Thu | Jun 19 | Revision — Omitted Qs finish + Mixed timed block (simulate exam) | 60 |
| Fri | Jun 20 | Mixed timed block — Pathology + Pharmacology (highest yield) | 60 |
| Sat | Jun 21 | Mixed timed block — Micro + Physio + Biochem | 60 |
| Sun | Jun 21 | OFF ☀️ | — |
FINAL WEEK — Jun 23–30 | Power Revision
| Day | Date | Activity |
|---|---|---|
| Mon | Jun 23 | Weak subject deep dive (whatever scored lowest) |
| Tue | Jun 24 | Mixed 60Q timed block — all subjects random |
| Wed | Jun 25 | Behavioral Science + Biostatistics revision (pure memorization) |
| Thu | Jun 26 | Pharmacology rapid review — mechanisms + side effects only |
| Fri | Jun 27 | Pathology rapid review — classic findings + buzzwords |
| Sat | Jun 28 | Full 40Q timed mock block — exam simulation |
| Sun | Jun 28 | OFF ☀️ |
| Mon | Jun 29 | Final review — only your flagged/wrong answer notebook |
| Tue | Jun 30 | Light day — No new Qs. Only read notes. Rest. Sleep early. |
Progress Checkpoints
| Checkpoint | Date | Qs Done | % Complete |
|---|---|---|---|
| End Week 1 | Apr 19 | ~360 | 10% |
| End Week 2 | Apr 26 | ~720 | 20% |
| End Week 4 | May 10 | ~1,440 | 39% |
| End Week 6 | May 24 | ~2,160 | 59% |
| End Week 8 | Jun 7 | ~2,880 | 79% |
| Qbank complete | Jun 13 | ~3,658 | 100% ✅ |
| Jun 30 | Jun 30 | Revision done | Ready 🎯 |
Golden Rules
- Never skip explanations — read every one, even when correct
- Wrong answer log — one line: Topic → Why wrong → Correct concept
- Timed mode always for the 40Q block — builds exam stamina
- Read First Aid alongside each subject as you do UWorld
- Sundays = full off — no guilt, your brain consolidates on rest days
- If you miss a day — don't try to catch up with 120 Qs next day; just resume normally
Can you make a pdf please
Writing File
/home/user/uworld_timetable.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<meta name="viewport" content="width=device-width, initial-scale=1.0">
<title>UWorld Step 1 Timetable — Apr 14 to Jun 30, 2026</title>
<style>
@import url('https://fonts.googleapis.com/css2?family=Inter:wght@400;600;700;800&display=swap');
* { margin: 0; padding: 0; box-sizing: border-box; }
body {
font-family: 'Inter', sans-serif;
background: #f0f4f8;
color: #1a202c;
font-size: 13px;
line-height: 1.5;
}
.page {
max-width: 900px;
margin: 0 auto;
background: white;
padding: 40px 48px;
}
/* HEADER */
.header {
background: linear-gradient(135deg, #1a56db 0%, #0e3a8a 100%);
color: white;
padding: 32px 36px;
border-radius: 12px;
margin-bottom: 28px;
}
.header h1 {
font-size: 26px;
font-weight: 800;
letter-spacing: -0.5px;
margin-bottom: 6px;
}
.header p {
font-size: 14px;
opacity: 0.85;
}
.header .badge {
display: inline-block;
background: rgba(255,255,255,0.2);
border-radius: 20px;
padding: 4px 14px;
font-size: 12px;
font-weight: 600;
margin-top: 10px;
margin-right: 6px;
}
/* SECTION TITLES */
h2 {
font-size: 16px;
font-weight: 700;
color: #1a56db;
margin: 28px 0 10px 0;
padding-bottom: 6px;
border-bottom: 2px solid #e2e8f0;
text-transform: uppercase;
letter-spacing: 0.5px;
}
h3 {
font-size: 13px;
font-weight: 700;
color: #2d3748;
margin: 20px 0 8px 0;
}
/* TABLES */
table {
width: 100%;
border-collapse: collapse;
margin-bottom: 16px;
font-size: 12.5px;
}
thead th {
background: #1a56db;
color: white;
padding: 9px 12px;
text-align: left;
font-weight: 700;
font-size: 11.5px;
text-transform: uppercase;
letter-spacing: 0.4px;
}
tbody tr:nth-child(even) { background: #f7faff; }
tbody tr:nth-child(odd) { background: #ffffff; }
tbody td {
padding: 8px 12px;
border-bottom: 1px solid #e8edf5;
vertical-align: middle;
}
tbody tr:hover { background: #eef2ff; }
.sunday-row td {
background: #fef3c7 !important;
color: #92400e;
font-weight: 700;
}
.complete-row td {
background: #d1fae5 !important;
color: #065f46;
font-weight: 700;
}
.revision-row td {
background: #fde8ff !important;
color: #6b21a8;
font-weight: 600;
}
.qs-badge {
display: inline-block;
background: #1a56db;
color: white;
border-radius: 10px;
padding: 2px 9px;
font-size: 11px;
font-weight: 700;
min-width: 36px;
text-align: center;
}
/* STATS GRID */
.stats-grid {
display: grid;
grid-template-columns: repeat(4, 1fr);
gap: 12px;
margin-bottom: 24px;
}
.stat-card {
background: linear-gradient(135deg, #1a56db 0%, #1e40af 100%);
color: white;
border-radius: 10px;
padding: 16px;
text-align: center;
}
.stat-card .num {
font-size: 24px;
font-weight: 800;
line-height: 1;
margin-bottom: 4px;
}
.stat-card .label {
font-size: 10.5px;
opacity: 0.85;
font-weight: 600;
text-transform: uppercase;
letter-spacing: 0.4px;
}
/* DAILY SCHEDULE */
.schedule-grid {
display: grid;
grid-template-columns: 140px 1fr 80px;
gap: 0;
border: 1px solid #e2e8f0;
border-radius: 10px;
overflow: hidden;
margin-bottom: 20px;
}
.sched-header {
background: #1a56db;
color: white;
padding: 8px 12px;
font-weight: 700;
font-size: 11px;
text-transform: uppercase;
}
.sched-cell {
padding: 8px 12px;
border-bottom: 1px solid #e8edf5;
font-size: 12px;
vertical-align: middle;
}
.sched-cell.time { background: #f0f4f8; font-weight: 600; color: #1a56db; font-size: 11.5px; }
.sched-cell.block { background: #fff8f0; font-weight: 700; color: #c05621; }
.sched-cell.dur { background: #f7faff; text-align: center; font-weight: 600; color: #4a5568; }
.sched-cell.break-row { background: #f0fff4; color: #276749; font-weight: 600; }
/* SUBJECT TABLE */
.subj-badge {
display: inline-block;
padding: 2px 8px;
border-radius: 8px;
font-size: 11px;
font-weight: 700;
}
.subj-path { background:#fee2e2; color:#991b1b; }
.subj-pharm { background:#dbeafe; color:#1e3a8a; }
.subj-physio { background:#d1fae5; color:#065f46; }
.subj-micro { background:#fef3c7; color:#78350f; }
.subj-anat { background:#ede9fe; color:#4c1d95; }
.subj-bioc { background:#fce7f3; color:#831843; }
.subj-behav { background:#e0f2fe; color:#0c4a6e; }
.subj-immun { background:#ecfdf5; color:#064e3b; }
.subj-small { background:#f3f4f6; color:#374151; }
/* CHECKPOINT */
.checkpoint-grid {
display: grid;
grid-template-columns: repeat(3, 1fr);
gap: 10px;
margin-bottom: 20px;
}
.checkpoint-card {
border: 2px solid #e2e8f0;
border-radius: 10px;
padding: 12px;
text-align: center;
}
.checkpoint-card .date { font-size: 11px; color: #718096; font-weight: 600; text-transform: uppercase; }
.checkpoint-card .pct { font-size: 22px; font-weight: 800; color: #1a56db; line-height: 1.1; margin: 4px 0; }
.checkpoint-card .qs-done { font-size: 11px; color: #4a5568; }
.checkpoint-card.done { border-color: #10b981; }
.checkpoint-card.done .pct { color: #059669; }
/* RULES */
.rules-list {
list-style: none;
padding: 0;
}
.rules-list li {
padding: 8px 12px 8px 36px;
position: relative;
border-bottom: 1px solid #f0f4f8;
font-size: 12.5px;
}
.rules-list li::before {
content: attr(data-num);
position: absolute;
left: 8px;
width: 20px;
height: 20px;
background: #1a56db;
color: white;
border-radius: 50%;
font-size: 10px;
font-weight: 800;
display: flex;
align-items: center;
justify-content: center;
top: 8px;
}
/* FOOTER */
.footer {
margin-top: 32px;
padding-top: 16px;
border-top: 2px solid #e2e8f0;
text-align: center;
font-size: 11px;
color: #a0aec0;
}
.tip-box {
background: #eff6ff;
border-left: 4px solid #1a56db;
border-radius: 0 8px 8px 0;
padding: 12px 16px;
margin: 12px 0;
font-size: 12.5px;
color: #1e3a8a;
}
.week-header {
background: linear-gradient(90deg, #1a56db, #3b82f6);
color: white;
padding: 8px 16px;
border-radius: 8px;
margin: 20px 0 8px 0;
font-weight: 700;
font-size: 13px;
}
/* PRINT */
@media print {
body { background: white; font-size: 11px; }
.page { padding: 20px 24px; max-width: 100%; }
.header { padding: 20px 24px; }
.header h1 { font-size: 20px; }
h2 { font-size: 13px; margin: 18px 0 8px 0; }
.stats-grid { grid-template-columns: repeat(4, 1fr); gap: 8px; }
.stat-card .num { font-size: 18px; }
table { font-size: 10.5px; }
thead th { padding: 6px 8px; }
tbody td { padding: 5px 8px; }
.week-header { padding: 6px 12px; font-size: 11px; }
.checkpoint-grid { grid-template-columns: repeat(3, 1fr); }
.checkpoint-card .pct { font-size: 18px; }
.tip-box { font-size: 11px; padding: 8px 12px; }
.rules-list li { font-size: 11px; padding: 6px 12px 6px 32px; }
@page { margin: 15mm; size: A4; }
}
</style>
</head>
<body>
<div class="page">
<!-- HEADER -->
<div class="header">
<h1>UWorld USMLE Step 1 — Complete Timetable</h1>
<p>Personalized schedule to complete the entire question bank with full revision</p>
<div>
<span class="badge">📅 Apr 14 – Jun 30, 2026</span>
<span class="badge">📚 3,658 Questions</span>
<span class="badge">⏰ 8–9 hrs/day</span>
<span class="badge">🗓 Sundays Off</span>
</div>
</div>
<!-- STATS -->
<h2>The Numbers</h2>
<div class="stats-grid">
<div class="stat-card">
<div class="num">3,658</div>
<div class="label">Total Questions</div>
</div>
<div class="stat-card">
<div class="num">67</div>
<div class="label">Study Days</div>
</div>
<div class="stat-card">
<div class="num">60</div>
<div class="label">Questions/Day</div>
</div>
<div class="stat-card" style="background: linear-gradient(135deg, #059669, #047857);">
<div class="num">~12</div>
<div class="label">Revision Days Left</div>
</div>
</div>
<div class="tip-box">
💡 <strong>Great news:</strong> With 78 days available and only 67 needed to finish the bank, you have a comfortable <strong>~12 full days of pure revision</strong> (Jun 19–30) after completing all questions.
</div>
<!-- SUBJECT BREAKDOWN -->
<h2>Subject Allocation</h2>
<table>
<thead>
<tr>
<th>Subject</th>
<th>Questions</th>
<th>Days @ 60/day</th>
<th>Scheduled Weeks</th>
</tr>
</thead>
<tbody>
<tr><td><span class="subj-badge subj-path">Pathology</span></td><td>819</td><td>~14 days</td><td>Week 1–3 (Apr 14–29)</td></tr>
<tr><td><span class="subj-badge subj-pharm">Pharmacology</span></td><td>550</td><td>~9 days</td><td>Week 3–4 (Apr 30 – May 9)</td></tr>
<tr><td><span class="subj-badge subj-physio">Pathophysiology</span></td><td>488</td><td>~8 days</td><td>Week 4–5 (May 10–17)</td></tr>
<tr><td><span class="subj-badge subj-micro">Microbiology</span></td><td>348</td><td>~6 days</td><td>Week 6 (May 19–24)</td></tr>
<tr><td><span class="subj-badge subj-anat">Anatomy</span></td><td>308</td><td>~5 days</td><td>Week 6–7 (May 24–28)</td></tr>
<tr><td><span class="subj-badge subj-behav">Behavioral Science</span></td><td>254</td><td>~4 days</td><td>Week 7 (May 29–31)</td></tr>
<tr><td><span class="subj-badge subj-physio">Physiology</span></td><td>268</td><td>~4 days</td><td>Week 8 (Jun 2–4)</td></tr>
<tr><td><span class="subj-badge subj-bioc">Biochemistry</span></td><td>159</td><td>~3 days</td><td>Week 8 (Jun 5–6)</td></tr>
<tr><td><span class="subj-badge subj-immun">Immunology</span></td><td>132</td><td>~2 days</td><td>Week 8–9 (Jun 7–9)</td></tr>
<tr><td><span class="subj-badge subj-small">Biostatistics</span></td><td>121</td><td>~2 days</td><td>Week 9 (Jun 10)</td></tr>
<tr><td><span class="subj-badge subj-small">Genetics</span></td><td>107</td><td>~2 days</td><td>Week 9 (Jun 11)</td></tr>
<tr><td><span class="subj-badge subj-small">Embryology</span></td><td>75</td><td>~1 day</td><td>Week 9 (Jun 12)</td></tr>
<tr><td><span class="subj-badge subj-small">Histology</span></td><td>29</td><td>~1 day</td><td>Week 9 (Jun 12)</td></tr>
<tr style="background:#f0f4f8; font-weight:700;"><td><strong>TOTAL</strong></td><td><strong>3,658</strong></td><td><strong>~61 days</strong></td><td><strong>Done by ~Jun 13</strong></td></tr>
</tbody>
</table>
<!-- DAILY SCHEDULE -->
<h2>Daily Schedule (8–9 Hours)</h2>
<table>
<thead>
<tr><th>Time</th><th>Activity</th><th>Duration</th></tr>
</thead>
<tbody>
<tr><td>8:00 – 8:30 AM</td><td>Morning review — previous day's marked & incorrect Qs</td><td>30 min</td></tr>
<tr class="complete-row"><td>8:30 – 10:00 AM</td><td>⏱ Block 1 — 40 Questions (TIMED mode)</td><td>1.5 hrs</td></tr>
<tr><td>10:00 – 11:15 AM</td><td>Deep review of Block 1 explanations + make notes</td><td>1 hr 15 min</td></tr>
<tr><td>11:15 – 11:30 AM</td><td>☕ Short break</td><td>15 min</td></tr>
<tr class="complete-row"><td>11:30 AM – 12:30 PM</td><td>📖 Block 2 — 20 Questions (TUTOR mode)</td><td>1 hr</td></tr>
<tr><td>12:30 – 1:30 PM</td><td>🍽 Lunch break</td><td>1 hr</td></tr>
<tr><td>1:30 – 2:30 PM</td><td>Review Block 2 + update wrong answer log</td><td>1 hr</td></tr>
<tr><td>2:30 – 4:30 PM</td><td>First Aid / Sketchy / Pathoma — parallel reading of today's subject</td><td>2 hrs</td></tr>
<tr><td>4:30 – 5:30 PM</td><td>Anki / Flashcard review (new cards + due cards)</td><td>1 hr</td></tr>
<tr><td>5:30 – 6:00 PM</td><td>Plan tomorrow, review weak points</td><td>30 min</td></tr>
<tr style="background:#f0f4f8; font-weight:700;"><td colspan="2"><strong>Total: 40 Timed + 20 Tutor = 60 Qs/day with full review</strong></td><td><strong>~8.5 hrs</strong></td></tr>
</tbody>
</table>
<!-- WEEKLY TIMETABLE -->
<h2>Week-by-Week Schedule</h2>
<div class="week-header">WEEK 1 — Apr 14–19 | Pathology: Foundations</div>
<table>
<thead><tr><th>Day</th><th>Date</th><th>Subject / Focus</th><th>Qs</th></tr></thead>
<tbody>
<tr><td>Monday</td><td>Apr 14</td><td><span class="subj-badge subj-path">Pathology</span> Cell injury, Apoptosis, Necrosis</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Tuesday</td><td>Apr 15</td><td><span class="subj-badge subj-path">Pathology</span> Inflammation (acute + chronic)</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Wednesday</td><td>Apr 16</td><td><span class="subj-badge subj-path">Pathology</span> Tissue repair, Wound healing</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Thursday</td><td>Apr 17</td><td><span class="subj-badge subj-path">Pathology</span> Neoplasia basics, Carcinogenesis, Tumor markers</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Friday</td><td>Apr 18</td><td><span class="subj-badge subj-path">Pathology</span> Hematologic neoplasms (Leukemia/Lymphoma)</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Saturday</td><td>Apr 19</td><td><span class="subj-badge subj-path">Pathology</span> Vascular pathology</td><td><span class="qs-badge">60</span></td></tr>
<tr class="sunday-row"><td>Sunday</td><td>Apr 20</td><td>☀️ REST DAY — No studying</td><td>—</td></tr>
</tbody>
</table>
<div class="week-header">WEEK 2 — Apr 21–26 | Pathology: Organ Systems</div>
<table>
<thead><tr><th>Day</th><th>Date</th><th>Subject / Focus</th><th>Qs</th></tr></thead>
<tbody>
<tr><td>Monday</td><td>Apr 21</td><td><span class="subj-badge subj-path">Pathology</span> Cardiovascular</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Tuesday</td><td>Apr 22</td><td><span class="subj-badge subj-path">Pathology</span> Pulmonary</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Wednesday</td><td>Apr 23</td><td><span class="subj-badge subj-path">Pathology</span> GI — Esophagus to Small Bowel</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Thursday</td><td>Apr 24</td><td><span class="subj-badge subj-path">Pathology</span> GI — Colon, Liver, Pancreas</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Friday</td><td>Apr 25</td><td><span class="subj-badge subj-path">Pathology</span> Renal</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Saturday</td><td>Apr 26</td><td><span class="subj-badge subj-path">Pathology</span> Endocrine</td><td><span class="qs-badge">60</span></td></tr>
<tr class="sunday-row"><td>Sunday</td><td>Apr 27</td><td>☀️ REST DAY — No studying</td><td>—</td></tr>
</tbody>
</table>
<div class="week-header">WEEK 3 — Apr 28 – May 3 | Pathology Finish + Pharmacology Start</div>
<table>
<thead><tr><th>Day</th><th>Date</th><th>Subject / Focus</th><th>Qs</th></tr></thead>
<tbody>
<tr><td>Monday</td><td>Apr 28</td><td><span class="subj-badge subj-path">Pathology</span> MSK + Dermatology</td><td><span class="qs-badge">60</span></td></tr>
<tr class="complete-row"><td>Tuesday</td><td>Apr 29</td><td><span class="subj-badge subj-path">Pathology</span> Neuro + Repro — ✅ PATHOLOGY COMPLETE</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Wednesday</td><td>Apr 30</td><td><span class="subj-badge subj-pharm">Pharmacology</span> Autonomic Nervous System</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Thursday</td><td>May 1</td><td><span class="subj-badge subj-pharm">Pharmacology</span> CNS drugs (Antidepressants, Antipsychotics)</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Friday</td><td>May 2</td><td><span class="subj-badge subj-pharm">Pharmacology</span> CNS drugs (Antiepileptics, Anesthesia, Opioids)</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Saturday</td><td>May 3</td><td><span class="subj-badge subj-pharm">Pharmacology</span> Cardiovascular drugs (Antihypertensives, Antiarrhythmics)</td><td><span class="qs-badge">60</span></td></tr>
<tr class="sunday-row"><td>Sunday</td><td>May 4</td><td>☀️ REST DAY — No studying</td><td>—</td></tr>
</tbody>
</table>
<div class="week-header">WEEK 4 — May 5–10 | Pharmacology Finish + Pathophysiology Start</div>
<table>
<thead><tr><th>Day</th><th>Date</th><th>Subject / Focus</th><th>Qs</th></tr></thead>
<tbody>
<tr><td>Monday</td><td>May 5</td><td><span class="subj-badge subj-pharm">Pharmacology</span> Cardiovascular (Statins, Anticoagulants, Antiplatelets)</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Tuesday</td><td>May 6</td><td><span class="subj-badge subj-pharm">Pharmacology</span> Antimicrobials Part 1 (Cell wall, Protein synthesis)</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Wednesday</td><td>May 7</td><td><span class="subj-badge subj-pharm">Pharmacology</span> Antimicrobials Part 2 (Quinolones, Antifungals, Antivirals)</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Thursday</td><td>May 8</td><td><span class="subj-badge subj-pharm">Pharmacology</span> Endocrine drugs (Insulin, Thyroid, Steroids)</td><td><span class="qs-badge">60</span></td></tr>
<tr class="complete-row"><td>Friday</td><td>May 9</td><td><span class="subj-badge subj-pharm">Pharmacology</span> Chemotherapy + Immunosuppressants — ✅ PHARMACOLOGY COMPLETE</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Saturday</td><td>May 10</td><td><span class="subj-badge subj-physio">Pathophysiology</span> Cardiovascular</td><td><span class="qs-badge">60</span></td></tr>
<tr class="sunday-row"><td>Sunday</td><td>May 11</td><td>☀️ REST DAY — No studying</td><td>—</td></tr>
</tbody>
</table>
<div class="week-header">WEEK 5 — May 12–17 | Pathophysiology</div>
<table>
<thead><tr><th>Day</th><th>Date</th><th>Subject / Focus</th><th>Qs</th></tr></thead>
<tbody>
<tr><td>Monday</td><td>May 12</td><td><span class="subj-badge subj-physio">Pathophysiology</span> Pulmonary</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Tuesday</td><td>May 13</td><td><span class="subj-badge subj-physio">Pathophysiology</span> Renal (AKI, CKD, Acid-base)</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Wednesday</td><td>May 14</td><td><span class="subj-badge subj-physio">Pathophysiology</span> GI + Hepatobiliary</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Thursday</td><td>May 15</td><td><span class="subj-badge subj-physio">Pathophysiology</span> Endocrine</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Friday</td><td>May 16</td><td><span class="subj-badge subj-physio">Pathophysiology</span> Hematology (Anemias, Coagulation)</td><td><span class="qs-badge">60</span></td></tr>
<tr class="complete-row"><td>Saturday</td><td>May 17</td><td><span class="subj-badge subj-physio">Pathophysiology</span> Neuro + Repro — ✅ PATHOPHYSIOLOGY COMPLETE</td><td><span class="qs-badge">60</span></td></tr>
<tr class="sunday-row"><td>Sunday</td><td>May 18</td><td>☀️ REST DAY — No studying</td><td>—</td></tr>
</tbody>
</table>
<div class="week-header">WEEK 6 — May 19–24 | Microbiology</div>
<table>
<thead><tr><th>Day</th><th>Date</th><th>Subject / Focus</th><th>Qs</th></tr></thead>
<tbody>
<tr><td>Monday</td><td>May 19</td><td><span class="subj-badge subj-micro">Microbiology</span> Bacteriology Part 1 (Gram +ve organisms)</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Tuesday</td><td>May 20</td><td><span class="subj-badge subj-micro">Microbiology</span> Bacteriology Part 2 (Gram –ve, Atypicals)</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Wednesday</td><td>May 21</td><td><span class="subj-badge subj-micro">Microbiology</span> Virology (DNA viruses + RNA viruses)</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Thursday</td><td>May 22</td><td><span class="subj-badge subj-micro">Microbiology</span> Mycology + Parasitology</td><td><span class="qs-badge">60</span></td></tr>
<tr class="complete-row"><td>Friday</td><td>May 23</td><td><span class="subj-badge subj-micro">Microbiology</span> Remaining Qs — ✅ MICROBIOLOGY COMPLETE</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Saturday</td><td>May 24</td><td><span class="subj-badge subj-anat">Anatomy</span> Head & Neck</td><td><span class="qs-badge">60</span></td></tr>
<tr class="sunday-row"><td>Sunday</td><td>May 25</td><td>☀️ REST DAY — No studying</td><td>—</td></tr>
</tbody>
</table>
<div class="week-header">WEEK 7 — May 26–31 | Anatomy + Behavioral Science</div>
<table>
<thead><tr><th>Day</th><th>Date</th><th>Subject / Focus</th><th>Qs</th></tr></thead>
<tbody>
<tr><td>Monday</td><td>May 26</td><td><span class="subj-badge subj-anat">Anatomy</span> Upper limb + Lower limb</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Tuesday</td><td>May 27</td><td><span class="subj-badge subj-anat">Anatomy</span> Thorax + Abdomen</td><td><span class="qs-badge">60</span></td></tr>
<tr class="complete-row"><td>Wednesday</td><td>May 28</td><td><span class="subj-badge subj-anat">Anatomy</span> Neuroanatomy — ✅ ANATOMY COMPLETE</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Thursday</td><td>May 29</td><td><span class="subj-badge subj-behav">Behavioral Sci</span> Biostatistics/Epidemiology + Ethics</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Friday</td><td>May 30</td><td><span class="subj-badge subj-behav">Behavioral Sci</span> Development, Psychiatry, Social determinants</td><td><span class="qs-badge">60</span></td></tr>
<tr class="complete-row"><td>Saturday</td><td>May 31</td><td><span class="subj-badge subj-behav">Behavioral Sci</span> Remaining Qs — ✅ BEHAVIORAL SCIENCE COMPLETE</td><td><span class="qs-badge">60</span></td></tr>
<tr class="sunday-row"><td>Sunday</td><td>Jun 1</td><td>☀️ REST DAY — No studying</td><td>—</td></tr>
</tbody>
</table>
<div class="week-header">WEEK 8 — Jun 2–7 | Physiology + Biochemistry + Immunology Start</div>
<table>
<thead><tr><th>Day</th><th>Date</th><th>Subject / Focus</th><th>Qs</th></tr></thead>
<tbody>
<tr><td>Monday</td><td>Jun 2</td><td><span class="subj-badge subj-physio">Physiology</span> Cardiovascular + Pulmonary</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Tuesday</td><td>Jun 3</td><td><span class="subj-badge subj-physio">Physiology</span> Renal + GI</td><td><span class="qs-badge">60</span></td></tr>
<tr class="complete-row"><td>Wednesday</td><td>Jun 4</td><td><span class="subj-badge subj-physio">Physiology</span> Neuro + Endocrine — ✅ PHYSIOLOGY COMPLETE</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Thursday</td><td>Jun 5</td><td><span class="subj-badge subj-bioc">Biochemistry</span> Metabolism (Glycolysis, TCA, Fatty acids)</td><td><span class="qs-badge">60</span></td></tr>
<tr class="complete-row"><td>Friday</td><td>Jun 6</td><td><span class="subj-badge subj-bioc">Biochemistry</span> Molecular biology + Nutrition — ✅ BIOCHEMISTRY COMPLETE</td><td><span class="qs-badge">60</span></td></tr>
<tr><td>Saturday</td><td>Jun 7</td><td><span class="subj-badge subj-immun">Immunology</span> Innate immunity + Adaptive immunity</td><td><span class="qs-badge">60</span></td></tr>
<tr class="sunday-row"><td>Sunday</td><td>Jun 8</td><td>☀️ REST DAY — No studying</td><td>—</td></tr>
</tbody>
</table>
<div class="week-header">WEEK 9 — Jun 9–14 | Finish All Subjects 🎉</div>
<table>
<thead><tr><th>Day</th><th>Date</th><th>Subject / Focus</th><th>Qs</th></tr></thead>
<tbody>
<tr class="complete-row"><td>Monday</td><td>Jun 9</td><td><span class="subj-badge subj-immun">Immunology</span> Remaining Qs — ✅ IMMUNOLOGY COMPLETE</td><td><span class="qs-badge">72</span></td></tr>
<tr class="complete-row"><td>Tuesday</td><td>Jun 10</td><td><span class="subj-badge subj-small">Biostatistics</span> Full subject — ✅ BIOSTATISTICS COMPLETE</td><td><span class="qs-badge">60</span></td></tr>
<tr class="complete-row"><td>Wednesday</td><td>Jun 11</td><td><span class="subj-badge subj-small">Genetics</span> Full subject — ✅ GENETICS COMPLETE</td><td><span class="qs-badge">60</span></td></tr>
<tr class="complete-row"><td>Thursday</td><td>Jun 12</td><td><span class="subj-badge subj-small">Embryology</span> + <span class="subj-badge subj-small">Histology</span> — ✅ BOTH COMPLETE</td><td><span class="qs-badge">60</span></td></tr>
<tr class="complete-row"><td>Friday</td><td>Jun 13</td><td>🎉 <strong>ENTIRE QBANK COMPLETE</strong> — Mixed weak subject review block</td><td><span class="qs-badge">60</span></td></tr>
<tr class="revision-row"><td>Saturday</td><td>Jun 14</td><td>📝 REVISION DAY 1 — All Incorrect Qs (252 total) Part 1</td><td><span class="qs-badge">60</span></td></tr>
<tr class="sunday-row"><td>Sunday</td><td>Jun 15</td><td>☀️ REST DAY — No studying</td><td>—</td></tr>
</tbody>
</table>
<div class="week-header">WEEK 10 — Jun 16–21 | Pure Revision</div>
<table>
<thead><tr><th>Day</th><th>Date</th><th>Activity</th><th>Qs</th></tr></thead>
<tbody>
<tr class="revision-row"><td>Monday</td><td>Jun 16</td><td>📝 Revision — Incorrect Qs Part 2 (finish all 252)</td><td><span class="qs-badge">60</span></td></tr>
<tr class="revision-row"><td>Tuesday</td><td>Jun 17</td><td>📝 Revision — All Marked Qs (65) + Omitted Qs Part 1</td><td><span class="qs-badge">60</span></td></tr>
<tr class="revision-row"><td>Wednesday</td><td>Jun 18</td><td>📝 Revision — Omitted Qs Part 2 (259 total)</td><td><span class="qs-badge">60</span></td></tr>
<tr class="revision-row"><td>Thursday</td><td>Jun 19</td><td>📝 Omitted Qs finish + Mixed timed block (simulate exam)</td><td><span class="qs-badge">60</span></td></tr>
<tr class="revision-row"><td>Friday</td><td>Jun 20</td><td>⏱ Mixed timed block — Pathology + Pharmacology (highest yield)</td><td><span class="qs-badge">60</span></td></tr>
<tr class="revision-row"><td>Saturday</td><td>Jun 21</td><td>⏱ Mixed timed block — Micro + Physio + Biochem</td><td><span class="qs-badge">60</span></td></tr>
<tr class="sunday-row"><td>Sunday</td><td>Jun 22</td><td>☀️ REST DAY — No studying</td><td>—</td></tr>
</tbody>
</table>
<div class="week-header">FINAL WEEK — Jun 23–30 | Power Revision + Exam Prep</div>
<table>
<thead><tr><th>Day</th><th>Date</th><th>Activity</th><th>Qs</th></tr></thead>
<tbody>
<tr class="revision-row"><td>Monday</td><td>Jun 23</td><td>📉 Weak subject deep dive (whatever scored lowest)</td><td><span class="qs-badge">60</span></td></tr>
<tr class="revision-row"><td>Tuesday</td><td>Jun 24</td><td>⏱ Mixed 60Q timed block — all subjects random</td><td><span class="qs-badge">60</span></td></tr>
<tr class="revision-row"><td>Wednesday</td><td>Jun 25</td><td>📊 Behavioral Science + Biostatistics rapid revision (memorization focus)</td><td><span class="qs-badge">40</span></td></tr>
<tr class="revision-row"><td>Thursday</td><td>Jun 26</td><td>💊 Pharmacology rapid review — mechanisms + side effects only</td><td><span class="qs-badge">40</span></td></tr>
<tr class="revision-row"><td>Friday</td><td>Jun 27</td><td>🔬 Pathology rapid review — classic findings + buzzwords</td><td><span class="qs-badge">40</span></td></tr>
<tr class="revision-row"><td>Saturday</td><td>Jun 28</td><td>⏱ Final 40Q FULL TIMED MOCK — exam simulation (strict conditions)</td><td><span class="qs-badge">40</span></td></tr>
<tr class="sunday-row"><td>Sunday</td><td>Jun 29</td><td>☀️ REST DAY — No studying</td><td>—</td></tr>
<tr class="revision-row"><td>Monday</td><td>Jun 30</td><td>✏️ Light day — Wrong answer notebook only. NO new Qs. Sleep early.</td><td>—</td></tr>
</tbody>
</table>
<!-- PROGRESS CHECKPOINTS -->
<h2>Progress Checkpoints</h2>
<div class="checkpoint-grid">
<div class="checkpoint-card">
<div class="date">Apr 19 (End Wk 1)</div>
<div class="pct">~10%</div>
<div class="qs-done">~360 Qs done</div>
</div>
<div class="checkpoint-card">
<div class="date">Apr 26 (End Wk 2)</div>
<div class="pct">~20%</div>
<div class="qs-done">~720 Qs done</div>
</div>
<div class="checkpoint-card">
<div class="date">May 3 (End Wk 3)</div>
<div class="pct">~29%</div>
<div class="qs-done">~1,080 Qs done</div>
</div>
<div class="checkpoint-card">
<div class="date">May 10 (End Wk 4)</div>
<div class="pct">~39%</div>
<div class="qs-done">~1,440 Qs done</div>
</div>
<div class="checkpoint-card">
<div class="date">May 17 (End Wk 5)</div>
<div class="pct">~49%</div>
<div class="qs-done">~1,800 Qs done</div>
</div>
<div class="checkpoint-card">
<div class="date">May 24 (End Wk 6)</div>
<div class="pct">~59%</div>
<div class="qs-done">~2,160 Qs done</div>
</div>
<div class="checkpoint-card">
<div class="date">May 31 (End Wk 7)</div>
<div class="pct">~69%</div>
<div class="qs-done">~2,520 Qs done</div>
</div>
<div class="checkpoint-card">
<div class="date">Jun 7 (End Wk 8)</div>
<div class="pct">~79%</div>
<div class="qs-done">~2,880 Qs done</div>
</div>
<div class="checkpoint-card done">
<div class="date">Jun 13 (End Wk 9)</div>
<div class="pct">100% ✅</div>
<div class="qs-done">3,658 Qs — BANK DONE</div>
</div>
</div>
<!-- GOLDEN RULES -->
<h2>Golden Rules (Non-Negotiable)</h2>
<ul class="rules-list">
<li data-num="1"><strong>Never skip explanations</strong> — read every one, even when you got the answer correct. The explanation teaches more than the question.</li>
<li data-num="2"><strong>Wrong answer log</strong> — one line per wrong answer: <em>Topic → Why I was wrong → Correct concept.</em> Review every Saturday.</li>
<li data-num="3"><strong>Timed mode for the 40Q block always</strong> — builds exam stamina and time management from day one.</li>
<li data-num="4"><strong>Read First Aid in parallel</strong> — open the relevant FA section after every UWorld block. UWorld explains; FA consolidates.</li>
<li data-num="5"><strong>Sundays = full off</strong> — no guilt, no "just a few cards." Your brain consolidates memory during rest.</li>
<li data-num="6"><strong>If you miss a day</strong> — do NOT try to catch up with 120 Qs the next day. Just resume the normal 60. Consistency beats bingeing.</li>
<li data-num="7"><strong>Mark aggressively</strong> — if you're not 100% certain, mark it. Your marked list is your personal high-yield review set.</li>
</ul>
<!-- FOOTER -->
<div class="footer">
<p>UWorld USMLE Step 1 Timetable | Apr 14 – Jun 30, 2026 | 3,658 Questions | 60 Qs/day | Generated by Orris</p>
<p style="margin-top:4px;">To save as PDF: Open in browser → File → Print → Save as PDF (A4, margins: default)</p>
</div>
</div>
</body>
</html>
Your file is ready at:
📄
/home/user/uworld_timetable.htmlTo save it as a PDF:
- Open the file in any browser (Chrome, Edge, Firefox)
- Press Ctrl+P (or Cmd+P on Mac)
- Set destination to "Save as PDF"
- Paper size: A4, Margins: Default
- Enable "Background graphics" so the colors print properly
- Click Save
The PDF includes everything — color-coded weekly tables, subject breakdown, daily schedule, progress checkpoints, golden rules, and Sunday rest days clearly marked in yellow. Green rows = subject completion milestones, purple rows = revision days.
I cant open
Unfortunately, I can't generate or export actual downloadable PDF/HTML files that you can open on your device — the file only exists on the server side and isn't accessible to you directly.
Here's what you can do to get a PDF:
Option 1 — Copy from chat (easiest)
- Scroll up to the full timetable I wrote in the previous message
- Select all the text → paste into Microsoft Word or Google Docs
- File → Download as PDF
Option 2 — Google Docs (best formatting)
- Open docs.google.com
- Paste the timetable text
- Use Format → Table to recreate the tables
- File → Download → PDF
Option 3 — Notion (cleanest)
- Open notion.so
- Create a new page → paste the content
- Click the ... menu → Export → PDF
Option 4 — I generate a cleaner plain-text version
I can rewrite the entire timetable in a clean plain format that you can directly paste into Word and it'll look good instantly — just say the word and I'll do it right now.
Which option works best for you?
This is a shared conversation. Sign in to Orris to start your own chat.