Both diagrams are excellent. Now I have everything needed to build a comprehensive, USMLE-focused enhanced note. Here it is:
🧬 Fibrinolysis & Plasmin — Enhanced USMLE Notes
🔑 Core Concept
| Term | Definition |
|---|
| Plasminogen | Inactive zymogen → synthesized by the liver |
| Plasmin | Active enzyme → cleaves fibrin → fibrin degradation products (FDPs) |
| Fibrinolysis | The physiologic system that dissolves clots to restore vascular patency |
Plasmin is the "thrombin equivalent" of the fibrinolytic system — just as thrombin drives clot formation, plasmin drives clot dissolution.
— Harrison's Principles of Internal Medicine 22E
⚙️ Activation Flowchart
FIBRIN CLOT FORMS
│
▼
Plasminogen binds to fibrin (via lysine-binding sites)
│
▼
tPA released from endothelial cells → also binds fibrin
│
▼
TERNARY COMPLEX: Fibrin + Plasminogen + tPA
│ ← greatly accelerates activation
▼
Plasminogen ──tPA/uPA──► PLASMIN
│
▼
Fibrin cleaved → FDPs + D-DIMER
"The assembly of a ternary complex, consisting of fibrin, plasminogen, and tPA, promotes the localized interaction between plasminogen and tPA and greatly accelerates the rate of plasminogen activation to plasmin." — Harrison's 22E, p. 515
Key insight: Partial fibrin degradation by plasmin exposes new lysine residues → more plasminogen/tPA binding sites → self-amplifying loop. This is why the reaction is fibrin-specific and self-amplifying at the clot surface.
📊 Master Diagram — Fibrinolytic System
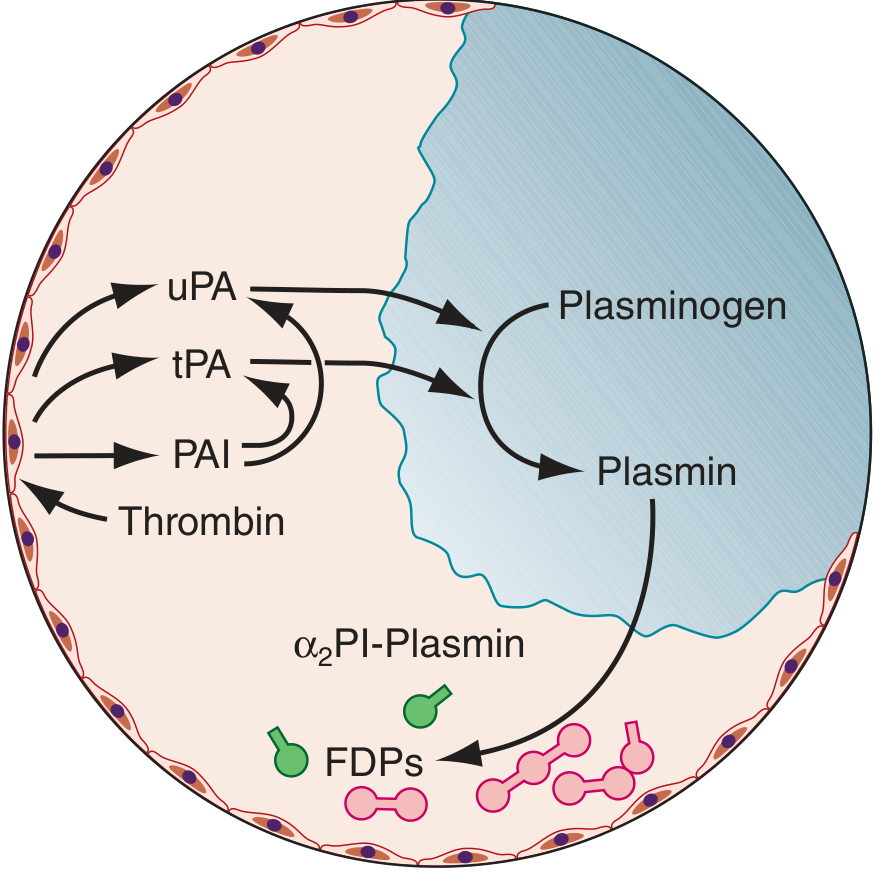
FIGURE 69-4 — Harrison's Principles of Internal Medicine 22E: tPA is released from endothelial cells, binds fibrin, and activates plasminogen → plasmin. PAI-1/PAI-2 inhibit tPA and uPA. Free plasmin is quenched by α₂-antiplasmin. FDPs are released.
🔬 Molecular Mechanism — D-dimer Formation
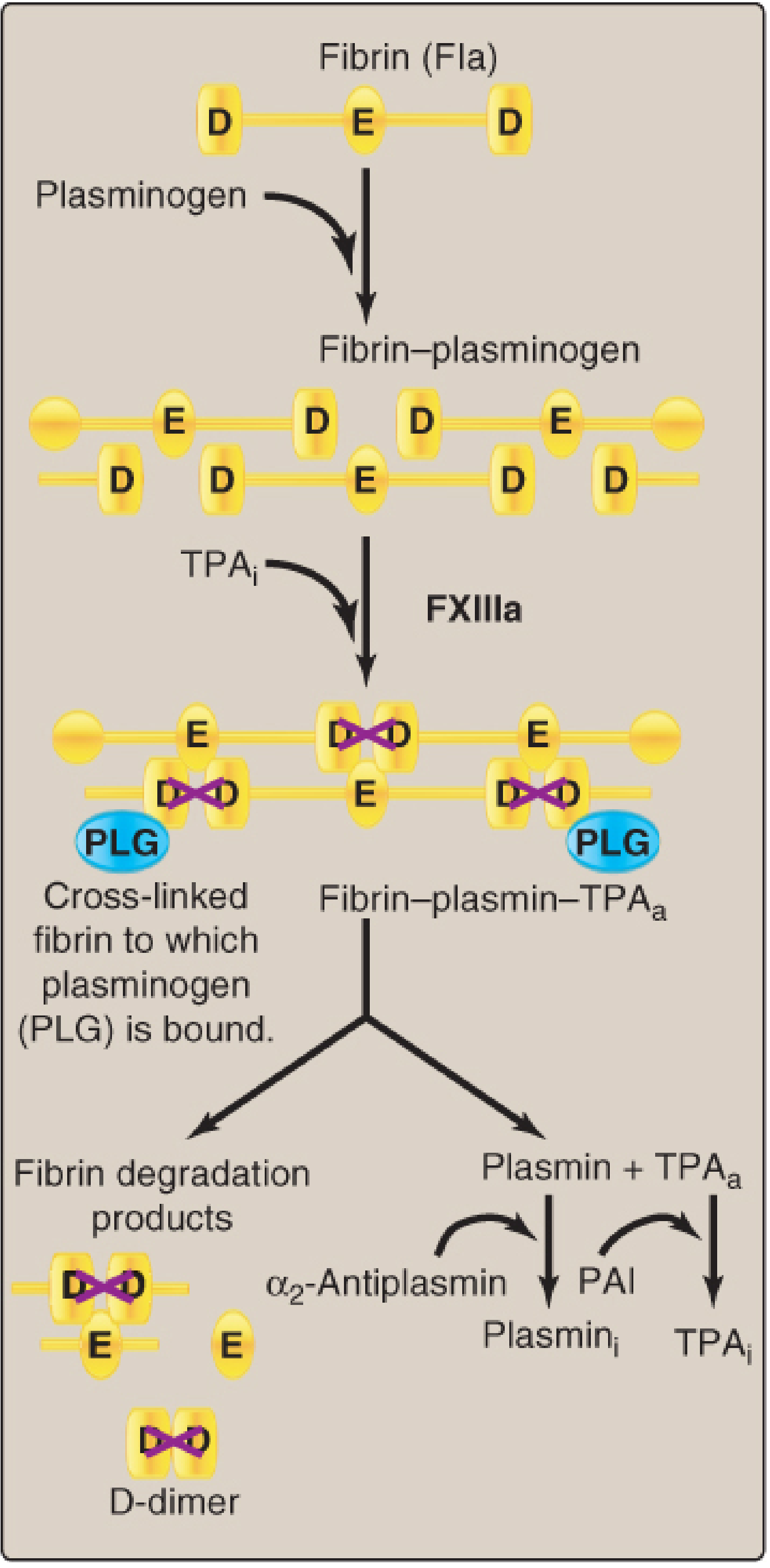
Lippincott Illustrated Reviews Biochemistry 8e, Fig. 35.19: Plasmin cleaves cross-linked fibrin (D–E–D structure) → FDPs + D-dimer (two cross-linked D domains). tPA and plasmin are released from the clot upon completion.
Why D-dimer is specific for cross-linked fibrin:
- Plasminogen cleaves the Arg560–Val561 bond of plasminogen
- When plasmin acts on Factor XIIIa cross-linked fibrin → releases D-dimers (two D domains covalently bound)
- D-dimer is NOT produced from fibrinogen → clot-specific marker
💊 Pharmacology — Full USMLE Map
Thrombolytics (Pro-fibrinolytic)
| Drug | Mechanism | Half-life | Clinical Use |
|---|
| Alteplase (tPA) | Recombinant tPA; fibrin-specific | ~5 min | Ischemic stroke ≤4.5h, STEMI, massive PE |
| Reteplase (rPA) | Mutant tPA; double IV bolus | ~18 min | STEMI |
| Tenecteplase (TNK) | Mutant tPA; single weight-based bolus | ~20 min | STEMI |
| Streptokinase | Non-fibrin-specific; binds plasminogen | ~30 min | STEMI (older agent) |
"These drugs all act by promoting the conversion of plasminogen to plasmin, which subsequently lyses fibrin thrombi." — Harrison's 22E
tPA dosing pearl (STEMI): 15 mg bolus → 50 mg over 30 min → 35 mg over 60 min
Fibrin-specificity distinction:
- tPA, rPA, TNK = fibrin-specific (preferentially activate fibrin-bound plasminogen)
- Streptokinase = non-fibrin-specific (systemic fibrinolysis → higher bleeding risk)
TIMI Flow Grading (exam favorite):
- Grade 0 = complete occlusion
- Grade 1 = contrast penetrates but no distal perfusion
- Grade 2 = perfusion but flow delayed
- Grade 3 = full perfusion, normal flow ← goal of thrombolysis
Antifibrinolytics (Anti-fibrinolytic)
| Drug | Mechanism | Uses |
|---|
| Tranexamic acid (TXA) | Lysine analog → blocks plasminogen lysine-binding sites on fibrin → prevents plasminogen activation | HMB, trauma hemorrhage, surgical bleeding, hemophilia |
| ε-Aminocaproic acid | Same mechanism as TXA (lysine analog) | Same uses; longer infusion required |
Mechanism deep dive: Both are lysine analogs — they compete with fibrin for plasminogen's lysine-binding sites, preventing the Fibrin-Plasminogen-tPA ternary complex from forming → no plasmin generation → clot stabilization
"Both lysine analog plasmin inhibitors (epsilon-aminocaproic acid and tranexamic acid) have been used [as antifibrinolytics]." — Barash Clinical Anesthesia 9e
🚫 Physiologic Inhibitors — USMLE Traps
INHIBITOR TARGET RESULT
─────────────────────────────────────────────────────
PAI-1 (PAI-2) → tPA + uPA → ↓ plasminogen activation
(endothelial/
platelet release)
α₂-Antiplasmin → Free plasmin → Quenches any plasmin
escaping the clot
PAI-1 Mnemonics:
- PAI-1 is upregulated by thrombin (pro-coagulant state amplifies its own protection)
- PAI-1 ↑ in metabolic syndrome → thrombotic tendency
- PAI-1 excess = impaired fibrinolysis → DVT/PE risk
🧪 D-dimer — Clinical Correlations
| Condition | D-dimer | Reason |
|---|
| DVT / PE | ↑↑ | Active fibrin clot breakdown |
| DIC | ↑↑↑ | Massive simultaneous clotting + fibrinolysis |
| Pregnancy | ↑ (physiologic) | Increased fibrinogen turnover |
| Post-surgery | ↑ | Expected (limits utility) |
| Normal | Low | Rules out PE/DVT with high sensitivity |
High-yield trap: D-dimer has high sensitivity, low specificity → good for ruling OUT PE/DVT (negative predictive value), NOT ruling IN.
🎯 USMLE Flowchart — Coagulation vs. Fibrinolysis
VESSEL INJURY
│
├──► COAGULATION CASCADE
│ │
│ ▼
│ Thrombin → Fibrinogen → FIBRIN CLOT
│
└──► FIBRINOLYTIC SYSTEM (counter-regulation)
│
▼
tPA (from endothelium) → binds fibrin
│
▼
Plasminogen → PLASMIN
│
├── Cleaves fibrin → FDPs + D-dimer
│
└── Inhibited by:
• α₂-antiplasmin (direct)
• PAI-1 (blocks tPA/uPA)
• TXA / aminocaproic acid (drug)
⚡ Contraindications to Thrombolytics (USMLE List)
| Absolute Contraindications |
|---|
| Prior intracranial hemorrhage (any time) |
| Ischemic stroke within prior 3 months (for STEMI; ≤4.5h window for AIS) |
| Suspected aortic dissection |
| Active internal bleeding (not menses) |
| Significant closed-head trauma / facial trauma within 3 months |
| Intracranial neoplasm |
| Relative Contraindications |
|---|
| BP >180/110 on presentation |
| Current anticoagulation use |
| Pregnancy |
| Traumatic or prolonged CPR (>10 min) |
| Major surgery within 3 weeks |
🧠 High-Yield USMLE Pearls Summary
| Pearl | Detail |
|---|
| tPA mechanism | Fibrin-bound → ternary complex → localized plasmin generation |
| Why tPA is "fibrin-specific" | Binds fibrin first → only activates fibrin-bound plasminogen |
| D-dimer source | Cross-linked fibrin only (not fibrinogen) → clot-specific |
| TXA mechanism | Lysine analog → blocks plasminogen binding to fibrin |
| PAI-1 role | Inhibits tPA + uPA; upregulated by thrombin → clot stabilization |
| α₂-antiplasmin | Quenches free plasmin in circulation → prevents systemic lysis |
| Streptokinase vs tPA | Streptokinase = non-fibrin-specific → systemic fibrinolysis |
| Alteplase stroke window | ≤4.5 hours from symptom onset |
| Aminocaproic acid | Same mechanism as TXA; less potent, longer infusion |
Sources: Harrison's Principles of Internal Medicine 22E (Fig. 69-4, pp. 514–516); Lippincott Illustrated Reviews: Biochemistry 8e (Fig. 35.19); Barash Clinical Anesthesia 9e; Goldman-Cecil Medicine