Give me a ospe case for and gynec with diagnosis
OSCE Cases: Obstetrics & Gynecology (MBBS Level)
CASE 1 - OBSTETRICS
Station: Preeclampsia with Severe Features
- BP: 162/112 mm Hg (repeated after 10 minutes - same reading)
- Pulse: 88/min
- Pallor: mild
- Pedal and facial edema: +2
- Fundal height: 32 cm (smaller than dates)
- Fetal heart rate: 138 bpm
- Urine dipstick: proteinuria 3+ (24-hr urine protein: 6.2 g/day)
- CBC: Hb 9.8 g/dL, Platelets 88,000/mm³
- LFT: AST and ALT elevated (3x normal), LDH elevated
- Serum creatinine: 1.3 mg/dL
- Urine output last 24 hours: 380 mL
Preeclampsia with severe features (Severe Preeclampsia)
- BP ≥160/110 mm Hg
- Proteinuria >5 g/24 hr
- Thrombocytopenia (<100,000/mm³)
- Impaired liver function (elevated transaminases + RUQ pain)
- Oliguria (<500 mL/24 hr)
- Visual disturbances and headache (CNS involvement)
- FGR (fundal height less than expected)
Yes - this patient fulfills HELLP criteria:
- Hemolysis (elevated LDH, falling Hb)
- ELevated Liver enzymes (elevated AST/ALT)
- LPLow Platelets (88,000/mm³)
HELLP occurs in 5-10% of preeclamptic patients and carries a high maternal and perinatal mortality risk.
- Admit to a high-dependency unit
- IV Magnesium Sulfate - loading dose 4 g IV over 15-20 minutes, then 2 g/hr infusion (seizure prophylaxis / eclampsia prevention)
- Antihypertensive - IV Hydralazine or oral Nifedipine to keep diastolic BP <110 mm Hg
- Fetal surveillance - NST, Biophysical profile, Doppler
- Corticosteroids - Betamethasone 12 mg IM x2 doses (fetal lung maturity at 34 weeks)
- Definitive treatment - Delivery within 24-48 hours (delivery is the only cure)
- Continue magnesium sulfate for 12-24 hours postpartum
- Loss of patellar reflexes (first sign - <7 mEq/L)
- Respiratory depression (<10 breaths/min at levels ~12 mEq/L)
- Cardiac arrest (at very high levels)
- Antidote: Calcium gluconate 1 g IV
CASE 2 - GYNECOLOGY
Station: Ectopic Pregnancy
- Pulse: 118/min, thready
- BP: 90/60 mm Hg
- Pallor: marked
- Abdomen: generalized rigidity, rebound tenderness, guarding; shoulder-tip pain present
- Per vaginal: cervical motion tenderness ++; right adnexal tenderness; no obvious adnexal mass palpable
Ruptured Ectopic Pregnancy (Right Fallopian Tube)
- Amenorrhea (missed period)
- Abdominal/pelvic pain
- Abnormal vaginal bleeding (spotting / light bleeding)
The ampulla of the fallopian tube (~78% of cases). Other sites include the isthmus, fimbria, cornua, ovary, and abdominal cavity.
Urine/Serum β-hCG - will be positive (confirms pregnancy). In ruptured ectopic, quantitative β-hCG is usually >1500-2000 mIU/mL. With a β-hCG >5000 mIU/mL, an intrauterine gestational sac should be visible on transvaginal ultrasound - absence of this strongly suggests ectopic pregnancy.
- Empty uterine cavity (no intrauterine gestational sac)
- Free fluid in pouch of Douglas (hemoperitoneum)
- Possible adnexal mass (tubal ring sign)
This is a surgical emergency:
- Resuscitation - 2 large-bore IV lines, IV fluids, cross-match blood
- Oxygen, monitor vitals
- Emergency Laparotomy - Salpingectomy (removal of the ruptured tube)
- Note: Laparoscopy is preferred in stable patients; laparotomy in unstable/ruptured cases
- Prior PID / salpingitis (tubal scarring)
- Prior ectopic pregnancy
- Previous tubal surgery
- Use of intrauterine device (IUD)
- In vitro fertilization (IVF)
- Smoking
- Endometriosis
CASE 3 - GYNECOLOGY (Bonus)
Station: Abnormal Uterine Bleeding (AUB) / Anovulatory Bleeding
- Hb: 8.9 g/dL (hypochromic microcytic)
- Platelets: 210,000/mm³
- PT/aPTT: normal
- TSH: normal
- β-hCG: negative
- Pelvic ultrasound: normal uterus and ovaries
Anovulatory Abnormal Uterine Bleeding (AUB) - previously called Dysfunctional Uterine Bleeding (DUB)
At menarche, the hypothalamic-pituitary-ovarian (HPO) axis is immature, leading to anovulatory cycles. Without ovulation, there is no corpus luteum and no progesterone production. Estrogen stimulates the endometrium unopposed, causing irregular proliferation and irregular, sometimes heavy shedding.
- Pregnancy (ectopic/miscarriage) - ruled out by β-hCG
- Bleeding disorders (von Willebrand disease, ITP) - ruled out by coagulation studies
- Thyroid disease - ruled out by TSH
- Structural causes (fibroids, polyps) - ruled out by ultrasound
- Infection/trauma - ruled out by history and examination
- Iron supplementation (for iron-deficiency anemia)
- Hormonal therapy - Combined oral contraceptive pill (OCP) to regulate cycles and reduce blood loss; given as 1 pill every 6 hours for acute heavy bleeding, then taper
- For patients who cannot use estrogen: Progestins (Norethisterone 5 mg TDS for 21 days)
- Follow-up: most adolescents' cycles regulate spontaneously as the HPO axis matures
Women >35 years AND those with prolonged anovulatory bleeding at any age who are at high risk for endometrial carcinoma (obesity, PCOS, long-term unopposed estrogen exposure).
- Swanson's Family Medicine Review, Clinical Case Problem 1 (Ectopic Pregnancy)
- Textbook of Family Medicine 9e (Preeclampsia, HELLP, Magnesium Sulfate Protocol)
- Goldman-Cecil Medicine (Abnormal Uterine Bleeding - Diagnosis and Treatment)
Give me more cases
More OSCE Cases: Obstetrics & Gynecology (MBBS Level)
CASE 4 - OBSTETRICS
Station: Placenta Previa
- BP: 100/70 mm Hg, Pulse: 104/min
- Uterus: soft, non-tender
- Fetal heart rate: 148 bpm (reassuring)
- Per vaginal examination: NOT performed
Placenta Previa
Painless, bright red vaginal bleeding in the third trimester - this is the hallmark. There is NO uterine tenderness, NO contractions, and the uterus is soft.
Digital PV examination is absolutely contraindicated in suspected placenta previa - inserting fingers through the cervix can disrupt the overlying placenta and cause catastrophic hemorrhage. Instead, perform Transabdominal Ultrasonography (accuracy 93-98%) to visualize placental position. Transvaginal ultrasound can be used safely if the abdominal view is inadequate (probe placed near but not through the cervix with an empty bladder).
- Total/Complete Previa: placenta completely covers the cervical os
- Partial Previa: placenta partially covers the os
- Marginal Previa: placental edge reaches the edge of the os
- Low-lying placenta: placenta in lower uterine segment but not covering os
The low-lying placenta occupies the lower uterine segment, physically preventing the fetal head from engaging into the pelvis. This causes malpresentation - transverse or breech lie.
- Grand multiparity (G4) - repeated uterine scarring
- Previous cesarean section - uterine scar
- Advanced maternal age Other risk factors: multiple gestation, prior placenta previa, tobacco use, uterine abnormalities
- Admit and do NOT allow home
- IV access, blood group, cross-match, CBC
- If <37 weeks and mother/fetus stable: Expectant management - bed rest, steroids for fetal lung maturity (betamethasone), no intercourse
- If bleeding is uncontrolled or fetus is compromised: Emergency Cesarean Section
- At term with complete previa: Elective Cesarean Section at 36-37 weeks
CASE 5 - OBSTETRICS
Station: Abruptio Placentae (Placental Abruption)
- BP: 160/100 mm Hg
- Pulse: 112/min, Pallor: moderate
- Uterus: tense, "woody hard," extremely tender to palpation
- Uterine contractions: frequent, every 1-2 min
- Fetal heart rate: 90 bpm (bradycardia - fetal distress)
- Vaginal bleeding: dark red, moderate
Abruptio Placentae (Placental Abruption)
| Feature | Abruptio Placentae | Placenta Previa |
|---|---|---|
| Pain | Severe, constant | Painless |
| Bleeding color | Dark red | Bright red |
| Uterus | Hard, woody, tender | Soft, non-tender |
| Fetal distress | Common, early | Uncommon initially |
| Onset | Sudden, with pain | Sudden, painless |
| Presentation | Normal lie usually | Malpresentation common |
Spontaneous hemorrhage into the decidua basalis causes placental separation. The retroplacental hematoma compresses the placenta, cutting off fetal blood supply - causing fetal distress and possibly demise. Increased intrauterine pressure causes uterine hypertonicity ("woody" uterus). If blood penetrates through the uterine wall into the peritoneal cavity, this is called Couvelaire Uterus.
Disseminated Intravascular Coagulation (DIC) - the large retroplacental bleed releases thromboplastins into maternal circulation, consuming all clotting factors. Order: CBC + platelets, PT, aPTT, fibrinogen, fibrin degradation products (FDP), D-dimer.
- Hypertension (40-50% of cases) - most common
- Cocaine use
- Trauma
- Smoking
- Sudden uterine decompression (e.g., delivery of first twin, polyhydramnios drainage)
- Previous abruption
This is an obstetric emergency:
- Large-bore IV x2, aggressive IV fluid resuscitation, blood transfusion
- Oxygen, continuous fetal monitoring
- Coagulation studies, blood type and cross-match
- Emergency Cesarean Section - fetal bradycardia indicates compromised fetus requiring immediate delivery
- Correct coagulopathy with FFP, cryoprecipitate, platelets as needed
- D-immune globulin (Anti-D) if Rh-negative mother
CASE 6 - GYNECOLOGY
Station: Ovarian Torsion
- BP: 118/74 mm Hg, Pulse: 96/min, Temp: 37.4°C
- Abdomen: right iliac fossa tenderness, guarding
- Bimanual examination: right adnexal tenderness, no discharge
Right Ovarian Torsion
The utero-ovarian ligament is longer on the right side, giving the right ovary more mobility. Additionally, the sigmoid colon on the left limits available space for torsion on that side. Nearly 70% of torsions occur on the right.
An enlarged ovary (due to a cyst or mass) acts as a fulcrum and twists on its pedicle. This first obstructs venous return, causing vascular congestion and edema. Continued twisting then cuts off arterial supply, causing ischemia and ultimately ovarian necrosis if not treated promptly.
- Ovarian cysts or masses (most common predisposing factor)
- Pregnancy (enlarged corpus luteum cyst)
- Polycystic ovaries (PCOS)
- Ovarian hyperstimulation syndrome (after IVF)
- Prior tubal ligation
- Torsion can occur at any age - infants to postmenopausal women
Transvaginal Ultrasound with Color Doppler:
- Enlarged ovary >4 cm (most common finding)
- Absent or reduced venous blood flow on Doppler (venous disruption is the earliest sign)
- Free fluid in pelvis
- Adnexal mass
- Important: Up to 60% of torsion cases can be missed on arterial Doppler alone - venous Doppler is critical. A positive Doppler has 100% positive predictive value. A negative Doppler does NOT rule out torsion - clinical suspicion must guide management.
Emergency diagnostic and therapeutic laparoscopy - surgical untwisting (detorsion) of the ovary. If ovary is still viable, it is conserved (especially in young women). If necrotic, oophorectomy is performed. The underlying cyst is also dealt with (cystectomy).
Delayed diagnosis leads to irreversible ischemic necrosis and loss of the ovary. Prompt gynecological consultation and surgery are essential. 50% of patients are initially misdiagnosed - clinical suspicion must remain high.
CASE 7 - GYNECOLOGY
Station: Primary Dysmenorrhea vs. Endometriosis (Secondary Dysmenorrhea)
- Case A: Primary Dysmenorrhea
- Case B: Endometriosis (Secondary Dysmenorrhea)
| Feature | Primary | Secondary (Endometriosis) |
|---|---|---|
| Age of onset | Within 6-12 months of menarche | Years after pain-free cycles |
| Pelvic findings | Normal examination | Tender, fixed uterus; nodules in POD |
| Dyspareunia | Absent | Deep dyspareunia present |
| Ultrasound | Normal | Endometrioma ("chocolate cyst") may be seen |
| Associated symptoms | Nausea, diarrhea, headache | Dyspareunia, dyschezia, infertility |
Ovulatory cycles produce progesterone in the luteal phase. After progesterone withdrawal, the endometrium releases prostaglandins (especially PGF2α), which stimulate myometrial contractions, causing uterine vasoconstriction, ischemia, and pain - essentially "uterine angina."
NSAIDs (e.g., Ibuprofen, Mefenamic acid) - they inhibit COX enzymes, reducing prostaglandin synthesis and relieving pain. Start 1-2 days before expected onset of menses. OCPs can be added if contraception is also desired.
Diagnostic Laparoscopy with biopsy - the gold standard. It allows direct visualization of ectopic endometrial implants (bluish-black "powder burn" lesions), adhesions, and endometriomas. Histology confirms endometrial glands and stroma outside the uterus.
- Medical: Combined OCP (continuous), Progestins, GnRH agonists (Leuprolide - induces temporary menopause), Danazol
- Surgical: Laparoscopic excision/ablation of implants, cystectomy for endometrioma
- Definitive: Hysterectomy + bilateral salpingo-oophorectomy (for completed family, severe disease)
CASE 8 - OBSTETRICS
Station: Gestational Diabetes Mellitus (GDM)
- 50 g GCT (1-hour): blood glucose = 155 mg/dL (abnormal ≥140)
- 100 g OGTT performed: Fasting = 102 mg/dL; 1-hr = 196 mg/dL; 2-hr = 170 mg/dL; 3-hr = 148 mg/dL (all 4 values abnormal)
Gestational Diabetes Mellitus (GDM) Diagnosis requires 2 or more abnormal values on the 100 g, 3-hour OGTT. This patient has all 4 values abnormal.
| Time | Abnormal if ≥ |
|---|---|
| Fasting | 105 mg/dL |
| 1 hour | 190 mg/dL |
| 2 hours | 165 mg/dL |
| 3 hours | 145 mg/dL |
Pregnancy is a state of progressive insulin resistance, driven primarily by human placental lactogen (hPL) and other placental hormones. hPL increases with placental mass and gestational age. Most women compensate with increased insulin secretion, but those with limited pancreatic reserve cannot - resulting in hyperglycemia.
- Obesity (BMI >30)
- South Asian ethnicity (high-risk group)
- Previous macrosomic baby (>4 kg)
- Family history of type 2 diabetes
- Glucosuria on dipstick
- Age >25 years
- Macrosomia (large baby >4 kg) - most common
- Shoulder dystocia during delivery
- Neonatal hypoglycemia (baby used to high glucose stops receiving it after birth)
- Neonatal hypocalcemia, polycythemia, hyperbilirubinemia
- Stillbirth / fetal demise
- Congenital anomalies (if hyperglycemia in 1st trimester - more relevant in pre-existing T2DM)
- Diet and exercise first: 30-35 kcal/kg lean body weight/day; walking is recommended
- Blood sugar targets: Fasting <105 mg/dL; 2-hr postprandial <120 mg/dL
- If targets not met: Insulin therapy (insulin does not cross the placenta; safe in pregnancy)
- Fetal surveillance: Ultrasound for fetal growth every 4-6 weeks; antenatal NST in 3rd trimester
- Postpartum: 30-60% of women with GDM develop type 2 diabetes in their lifetime - annual glucose tolerance testing is recommended. Weight loss and exercise reduce this risk.
- Textbook of Family Medicine 9e - Placenta Previa, Abruptio Placentae, Gestational Diabetes
- Tintinalli's Emergency Medicine - Ovarian Torsion (pathophysiology, Doppler findings, management)
- Swanson's Family Medicine Review - Primary vs. Secondary Dysmenorrhea, Endometriosis
Give me more case
More OSCE Cases: Obstetrics & Gynecology (MBBS Level)
CASE 9 - OBSTETRICS
Station: Postpartum Hemorrhage (PPH)
Primary Postpartum Hemorrhage (PPH) due to Uterine Atony PPH is traditionally defined as blood loss >500 mL after vaginal delivery or >1000 mL after cesarean delivery within 24 hours. Clinically, any bleeding causing hemodynamic instability (as in this case) is considered PPH.
Cause Examples Tone Uterine atony (most common, 80%) Trauma Cervical/vaginal lacerations, uterine rupture, inversion Tissue Retained placental fragments Thrombin Coagulopathy (DIC, von Willebrand disease)
- Grand multiparity (G3P3) - uterine muscle fatigue
- Fetal macrosomia (4.2 kg) - overdistended uterus
- Prolonged labor (18 hours) - uterine exhaustion Other risk factors: polyhydramnios, multiple gestation, oxytocin use, chorioamnionitis, tocolytic agents
Step 1 - Resuscitate: 2 large-bore IV lines, IV crystalloids, oxygen, blood transfusion (type and cross-match), monitor vitalsStep 2 - Identify cause: Check uterine tone, inspect for lacerations, check for retained placenta, send coagulation studies (CBC, PT, aPTT, fibrinogen, D-dimer)Step 3 - Uterotonic drugs (for atony):
- Oxytocin 10-30 units in 1L IV fluid - first line; bimanual uterine compression/massage simultaneously
- Methylergonovine 0.2 mg IM q2-4h - contraindicated in hypertension (causes vasoconstriction)
- 15-methyl PGF2α (Carboprost/Hemabate) 0.25 mg IM q15-90 min (max 8 doses) - monitor pulse oximetry
- Misoprostol (PGE1 analogue) - rectal/sublingual
Step 4 - Surgical intervention if medical therapy fails:
- Uterine balloon tamponade
- B-Lynch compression suture
- Uterine artery ligation
- Emergency hysterectomy (last resort - most common indications: uterine atony, placenta accreta, uterine rupture)
AMTSL has been shown to reduce PPH incidence by two-thirds. It consists of:
- Early administration of oxytocin (10 units IM) immediately after delivery of the baby
- Early cord clamping and cutting
- Controlled cord traction (Brandt-Andrews maneuver) to deliver the placenta
CASE 10 - GYNECOLOGY
Station: Pelvic Inflammatory Disease (PID)
- Lower abdominal tenderness bilaterally
- Speculum: mucopurulent cervical discharge
- Bimanual: cervical motion tenderness (CMT), bilateral adnexal tenderness
- WBCs seen on wet prep
Pelvic Inflammatory Disease (PID)
PID is diagnosed clinically when lower abdominal or pelvic pain is present and at least ONE of:
- Cervical motion tenderness (CMT)
- Uterine tenderness
- Adnexal tenderness ...with no other cause identified.
Supportive criteria (increase diagnostic specificity):
- Oral temperature >38.3°C
- Mucopurulent cervical/vaginal discharge
- WBCs on vaginal wet prep
- Elevated ESR or CRP
- Laboratory confirmation of N. gonorrhoeae or C. trachomatis
- Neisseria gonorrhoeae and Chlamydia trachomatis - primary pathogens
- Anaerobes, gram-negative rods (e.g., E. coli), streptococci - secondary/polymicrobial
- Age <25 years (most common demographic)
- Multiple sexual partners
- No barrier contraception
- High-prevalence area for gonorrhea/chlamydia
- History of prior PID
- Suspected tubo-ovarian abscess (TOA)
- Pregnancy
- Failed outpatient treatment (no improvement in 72 hours)
- Severe illness (high fever, vomiting, inability to take oral medications)
- Surgical emergency cannot be excluded (e.g., appendicitis)
Inpatient (IV):
- Regimen A: IV Cefotetan or IV Cefoxitin + Doxycycline (oral or IV)
- Regimen B: IV Clindamycin + IV Gentamicin
Outpatient (IM/Oral):
- IM Ceftriaxone + oral Doxycycline ± oral Metronidazole (14-day course)
- Treat sexual partners simultaneously
- Infertility (from tubal scarring and blockage) - risk increases with each episode of PID
- Chronic pelvic pain
- Increased risk of ectopic pregnancy (scarred tubes)
- Tubo-ovarian abscess (TOA)
- Fitz-Hugh-Curtis syndrome - perihepatitis (right upper quadrant pain from perihepatic adhesions)
CASE 11 - OBSTETRICS
Station: Eclampsia
Eclampsia - defined as the occurrence of one or more generalized convulsions and/or coma in a woman with preeclampsia, in the absence of other neurological conditions (epilepsy, intracranial bleed).
Preeclampsia = hypertension + proteinuria in pregnancy (without seizures). Eclampsia = preeclampsia PLUS grand mal seizures. It represents the most severe end of the preeclampsia-eclampsia spectrum.
- Headache (severe, frontal/occipital) - from cerebral vasospasm
- Visual disturbances ("flashes" = photopsia, scotoma) - from retinal arteriolar spasm Other warning signs: epigastric/RUQ pain, nausea, vomiting, hyperreflexia, altered mental status
ABCDE + MgSO4:
- Airway - left lateral position, suction, oxygen (target SpO2 >95%)
- IV access - bloods: CBC, LFT, RFT, coagulation, uric acid, blood group
- Stop and prevent seizures: IV Magnesium Sulfate - 4-6 g loading dose over 15-20 min, then 2 g/hr maintenance infusion
- Control BP: IV Labetalol or oral Nifedipine (keep systolic <160, diastolic <110)
- Fetal monitoring: continuous CTG - bradycardia usually resolves once mother is stabilized
- Deliver the baby - eclampsia is an indication for expeditious delivery (vaginal or cesarean depending on cervical status and fetal condition)
- Continue MgSO4 for 24-48 hours postpartum
Give an additional 2 g MgSO4 IV bolus. If seizures continue despite this, consider IV Diazepam or IV Phenytoin as rescue therapy.
MgSO4 Level Sign 5-8 mEq/L Therapeutic range >7 mEq/L Loss of patellar reflex (first sign) ~10 mEq/L Respiratory depression ~15 mEq/L Cardiac arrest Antidote: Calcium gluconate 1 g IV (10 mL of 10% solution) given slowly
CASE 12 - GYNECOLOGY
Station: Polycystic Ovary Syndrome (PCOS)
- LH: 14 mIU/mL (elevated); FSH: 5 mIU/mL; LH:FSH ratio = 2.8:1 (elevated)
- Total testosterone: mildly elevated
- Fasting glucose: 102 mg/dL; Fasting insulin: elevated
- Pelvic ultrasound: bilateral enlarged ovaries with ≥12 follicles per ovary (2-9 mm), increased ovarian volume (>10 mL)
- Prolactin, TSH, 17-OH progesterone: normal
Polycystic Ovary Syndrome (PCOS)
Diagnosis requires 2 out of 3 of the following (after excluding other causes):
- Oligo-ovulation or anovulation (irregular/absent periods)
- Hyperandrogenism - clinical (hirsutism, acne, alopecia) or biochemical (elevated testosterone)
- Polycystic ovaries on ultrasound (≥12 follicles per ovary OR ovarian volume >10 mL)
This patient meets all 3 criteria.
- Congenital Adrenal Hyperplasia (CAH) - check 17-OH progesterone
- Cushing syndrome - check 24-hr urinary cortisol / dexamethasone suppression test
- Androgen-secreting tumors (ovarian or adrenal)
- Hyperprolactinemia - check serum prolactin
- Hypothyroidism - check TSH
The core defect involves insulin resistance and compensatory hyperinsulinemia. Excess insulin stimulates ovarian theca cells to produce excess androgens (testosterone). Elevated LH (from disordered GnRH pulsatility) further amplifies androgen production. Androgens disrupt follicular development, causing arrested follicles ("cysts") and anovulation. Anovulation leads to unopposed estrogen, risking endometrial hyperplasia.
Short-term:
- Infertility (anovulation)
- Irregular menstrual cycles
- Hirsutism, acne
- Endometrial hyperplasia/cancer (from unopposed estrogen)
Long-term:
- Type 2 Diabetes - >50% of PCOS women develop T2DM by age 40
- Metabolic syndrome, dyslipidemia
- Cardiovascular disease
- Obstructive sleep apnea
Goal Treatment Regulate cycles / endometrial protection Combined OCP (e.g., Diane-35) Reduce hirsutism OCP + anti-androgens (Spironolactone, Cyproterone acetate) Infertility / ovulation induction Clomiphene citrate (first line); Letrozole; Metformin Insulin resistance / metabolic Metformin + weight loss Weight loss Lifestyle modification (diet + exercise) - cornerstone of all treatment
- Textbook of Family Medicine 9e - Postpartum Hemorrhage (4 T's, uterotonics, surgical options)
- Swanson's Family Medicine Review - PID diagnostic criteria, causative organisms, antibiotic regimens
- Goldman-Cecil Medicine - PCOS pathobiology, Rotterdam criteria, complications, treatment
- Adams and Victor's Principles of Neurology - Eclampsia and magnesium sulfate seizure management
Give me homoeopathy medicine with case for obs and gynec
homoeopathy medicines obstetrics gynecology OSCE cases remedies
Homoeopathy OSCE Cases: Obstetrics & Gynecology
Note: These cases follow the homoeopathic approach of individualization - the remedy is chosen based on the totality of symptoms (mental, physical generals, and particulars), not diagnosis alone. The same disease may need different remedies in different patients.
CASE 1
Station: Dysmenorrhea (Primary)
Primary Dysmenorrhea
- Abdomen: pain, menses during
- Female: menses, painful (dysmenorrhea)
- Generals: heat ameliorates
- Mind: irritability, wants to be alone
Magnesia Phosphorica (Mag Phos)
- Keynote: Crampy, spasmodic, neuralgic pain - best remedy for spasmodic dysmenorrhea
- Pain relieved by warmth (hot water bottle, warm drinks)
- Pain relieved by pressure and bending double
- Radiates down thighs
- Potency: 6X or 30C - dissolve in warm water and sip (enhances absorption)
Differential Remedy: Colocynthis
- Violent cramping pain, doubled up, extreme pressure relieves
- Pain comes in waves, with anger/indignation as causative factor
- Restless during pain
Differential: Chamomilla
- Unbearable pain, extreme irritability, cannot stand being spoken to
- Pain with anger, wants to be carried
- Dark clotted blood, pain down thighs
CASE 2
Station: Menorrhagia / Heavy Menstrual Bleeding
Menorrhagia (Heavy Menstrual Bleeding) with possible hypothyroid constitution
Calcarea Carbonica (Calc Carb)
- Obese, chilly, sluggish constitution - classical "Calc Carb" patient
- Profuse, early, prolonged menses
- Exhaustion before and after menses
- Mentally slow, forgetful, confused
- Chilly patient - cannot tolerate cold
- Associated with leucorrhoea (milky, acrid)
- Potency: 200C monthly or 30C weekly depending on vitality
Differential: Sepia
- Profuse menses with bearing-down sensation ("as if everything would fall out")
- Indifferent to loved ones, irritable, weepy
- Worse before menses, better after vigorous exercise
- Yellowish/greenish leucorrhoea
Differential: China (Cinchona)
- Profuse bleeding leading to debility and exhaustion
- Blood dark, with clots
- Weakness from loss of body fluids
- Ringing in ears, faintness
CASE 3
Station: Amenorrhea (Absence of Periods)
Secondary Amenorrhea - stress/weight-loss induced (functional hypothalamic amenorrhea)
Pulsatilla Nigricans
- Most important remedy for amenorrhea in young girls
- Mild, yielding, emotional - weeps easily, craves consolation/company
- Periods absent or suppressed especially after emotional shock, grief, getting feet wet, or cold exposure
- Changeable moods
- Thirstless even when unwell
- Better in open air
- Potency: 30C or 200C
Differential: Natrum Muriaticum (Nat Mur)
- Amenorrhea from grief, suppressed emotions
- Introvert - does NOT want consolation, weeps alone
- Craves salt
- Worse at 10 AM
- Thin constitution despite eating well
Differential: Sepia
- Amenorrhea with indifference, bearing-down sensation
- Better from vigorous exercise
CASE 4
Station: Morning Sickness / Nausea and Vomiting of Pregnancy (NVP)
Nausea and Vomiting of Pregnancy (NVP) / Hyperemesis Gravidarum (if severe)
Nux Vomica
- Irritable, over-sensitive, fastidious patient
- Nausea worse in morning, after eating
- Retching but difficulty vomiting
- Nausea from smell of food or tobacco
- Better after vomiting temporarily
- Chilly patient, worse cold
- Potency: 30C
Differential: Ipecacuanha (Ipecac)
- Constant, persistent nausea - not relieved at all by vomiting
- Clean tongue (despite nausea)
- Vomiting of frothy mucus or food
- Face pale, profuse salivation
Differential: Sepia
- Nausea at the smell or thought of food
- Empty, all-gone feeling in stomach
- Indifferent to pregnancy, husband, children
- Better from eating (paradoxically)
Differential: Symphytum / Tabacum
- Tabacum: deathly nausea, vertigo, cold sweat, pallor - worse opening eyes, better in fresh air
- Excellent for sea-sickness type morning sickness
CASE 5
Station: Threatened Abortion / Recurrent Miscarriage
Threatened Abortion (with history of recurrent pregnancy loss)
Arsenicum Album
- Anxiety, fear of death/losing the baby, restlessness
- Wakes between 1-3 AM with anxiety
- Chilly, thirsty for small sips frequently
- Bleeding: dark, offensive
- Potency: 30C or 200C
Differential: Sabina
- Most important remedy for threatened/recurrent miscarriage
- Bleeding bright red, profuse, gushing, mixed with clots
- Pain from sacrum to pubes (pubic bone)
- Tendency to miscarry at 3rd month repeatedly
- Music is intolerable
Differential: Viburnum Opulus
- Threatened abortion with severe, crampy pains
- Pain radiates from back to thighs and loins
- Called the "homoeopathic antispasmodic of the uterus"
- Tendency to miscarry at 2nd and 3rd month
Differential: Caulophyllum
- Habitual abortion from uterine weakness/atony
- Painful, irregular uterine contractions
- Severe cramping in small muscles
- Also used for prolonged/inefficient labor
CASE 6
Station: Leucorrhoea (Vaginal Discharge)
Non-infective Leucorrhoea
Kreosotum
- Profuse, acrid, corrosive, offensive leucorrhoea
- Causes intense itching, burning, excoriation of vulva and thighs
- Discharge stains yellow and is very offensive (putrid smell)
- Worse between menses
- Burning and soreness of vagina
- Potency: 30C
Differential: Calcarea Carbonica
- Profuse, milky white, non-irritating discharge
- No burning or itching
- Chilly, obese, sluggish patient
Differential: Sepia
- Yellowish-green, offensive leucorrhoea
- With bearing-down sensation
- Worse before menses
- Itching of vulva
Differential: Borax
- Albuminous, thick, white, egg-white-like discharge
- With sensation of warm water flowing
- Worse between menses
- Anxiety about downward motion (characteristic)
Differential: Hydrastis
- Thick, ropy, yellow, stringy discharge
- Profuse, tenacious
- Associated with debility
CASE 7
Station: Menopausal Syndrome
Menopausal Syndrome (Perimenopause/Menopause with vasomotor and psychological symptoms)
Sepia
- Most important remedy for menopausal complaints
- Hot flushes with sweating, worse evening/night
- Bearing-down sensation in pelvis
- Indifference to loved ones - the hallmark of Sepia
- Weeping without reason, irritable
- Loss of libido
- Better from vigorous exercise (dancing, walking)
- Potency: 200C or 1M
Differential: Lachesis
- Hot flushes worse on waking, cannot bear anything tight around neck or waist
- Very talkative, jealous, suspicious
- Left-sided symptoms
- Worse after sleep, better from discharges
Differential: Sulphur
- Hot flushes with burning heat on top of head, hot palms and soles (kicks feet out of bed)
- Offensive perspiration
- Untidy, philosophical, selfish constitution
Differential: Glonoine
- Sudden, violent hot flushes with throbbing headache
- Surging of blood to head and face
- Confusion, cannot find her way in familiar streets
CASE 8
Station: Labor - Prolonged / Inefficient Uterine Contractions
Prolonged Active Labor / Hypotonic Uterine Dysfunction (arrested active phase)
Caulophyllum (Blue Cohosh)
- Most important remedy for inefficient uterine contractions
- Contractions are weak, irregular, spasmodic, painful but do not dilate the cervix
- Exhaustion from prolonged, fruitless labor
- Trembling of limbs
- Rigidity of os (cervix does not dilate)
- Also used in habitual abortion from uterine weakness
- Potency: 30C
Differential: Gelsemium
- Weakness, trembling, heaviness - "I can't do it" feeling
- Fear and anticipatory anxiety (anxiety before labor)
- Dilation slow due to nervous exhaustion
- Dull, drowsy, dizzy
Differential: Pulsatilla
- Irregular, changeable contractions
- Patient is weeping, clinging, wants company and reassurance
- Malpresentation (Pulsatilla is known to turn mal-presented babies - posterior/transverse)
- Thirstless
Quick Reference: Key Homoeopathic Remedies in Obs & Gynec
| Condition | Top Remedy | Key Indication |
|---|---|---|
| Dysmenorrhea (spasmodic) | Mag Phos | Heat + pressure relieve; crampy pain |
| Dysmenorrhea (with anger) | Chamomilla | Unbearable pain, irritable, dark clots |
| Heavy bleeding (obese, chilly) | Calc Carb | Profuse, exhausting periods |
| Heavy bleeding (bearing down) | Sepia | Indifference, bearing-down |
| Recurrent miscarriage | Sabina | Bright red gushing bleed, sacrum-to-pubis pain |
| Morning sickness (irritable) | Nux Vomica | Retching, worse smells, snappy |
| Morning sickness (constant nausea) | Ipecac | Nausea not relieved by vomiting |
| Amenorrhea (emotional, weepy) | Pulsatilla | Mild, yielding, thirstless, craves company |
| Leucorrhoea (acrid, burning) | Kreosotum | Corrosive, excoriates skin |
| Leucorrhoea (milky, bland) | Calc Carb | No irritation, chilly patient |
| Menopause (hot flushes + indifference) | Sepia | Bearing down, better exercise |
| Menopause (talkative, worse waking) | Lachesis | Left-sided, can't bear tight clothing |
| Inefficient labor | Caulophyllum | Weak irregular contractions |
| Labor (fear and trembling) | Gelsemium | Weak, drowsy, anxious |
| Threatened abortion | Sabina | Gushing bright red + clots |
| Postpartum hemorrhage | China | Weakness from blood loss |
Important note for exam: In homoeopathy, the totality of symptoms - especially mental generals, physical generals, and characteristic particulars - determines the remedy. Two patients with the same diagnosis (e.g., dysmenorrhea) may need completely different remedies based on their individual symptom picture. This is the principle of individualization - the cornerstone of homoeopathic prescribing.
Give me a give me instument of obs and gynec
obstetrics gynecology instruments OSCE identification uses images list
Instruments of Obstetrics & Gynecology
OSCE Instrument Identification Guide (MBBS Level)
In OSCE stations you will be shown an instrument and asked: Name it | Describe it | Uses | Contraindications | Complications
CATEGORY 1: EXAMINATION INSTRUMENTS
1. Cusco's Bivalve Speculum (Duck-bill Speculum)
- Two-bladed (bivalve), self-retaining speculum made of metal or plastic
- Has a thumbscrew to lock the blades open
- Blades open anteroposteriorly when inserted
- Routine pelvic/vaginal examination
- Visualization of cervix and vaginal walls
- Pap smear / cervical cytology
- High vaginal swab collection
- IUD insertion and removal
- Cervical biopsy / colposcopy
- Treatment of cervical erosion
2. Sims' Speculum (Single-blade / Duck-bill)
- Single-blade, L-shaped (double-ended) speculum
- Has a curved blade with a handle at one end
- NOT self-retaining - requires an assistant to hold it
- Examination of the anterior vaginal wall
- Diagnosis and repair of vesicovaginal fistula (VVF) and rectovaginal fistula
- Vaginal wall prolapse assessment
- Anterior colporrhaphy
3. Pinard's Fetal Stethoscope
- Trumpet-shaped, single-piece instrument made of wood or metal
- Wider end placed on maternal abdomen, narrower end to the examiner's ear
- Auscultation of fetal heart sounds
- Monitoring fetal wellbeing in labor
- Detects: fetal heart rate, rhythm, character
4. Pelvimeter (Pelvic Caliper)
- Large caliper with curved arms, calibrated in cm/inches
- Two types: External (Martin's) and Internal (Thoms')
- Measurement of external pelvic diameters (clinical pelvimetry)
- Interspinous diameter (normal ≥26 cm)
- Intercristal diameter (normal ≥28 cm)
- External conjugate / Baudelocque's diameter (normal ≥18 cm)
- Assess adequacy of pelvis for vaginal delivery
CATEGORY 2: CERVICAL & UTERINE INSTRUMENTS
5. Vulsellum Forceps (Volsellum Forceps)
- Long, straight or curved forceps with toothed (claw-like) tips - 1×1 or 2×2 teeth
- Ring handles (like scissors)
- Grasping and steadying the cervix during procedures
- IUD insertion / removal
- Dilatation and Curettage (D&C)
- Cervical biopsy
- Manual vacuum aspiration (MVA)
- IUCD insertion
- Pulling down the cervix for inspection
6. Uterine Sound (Sims' Uterine Sound)
- Long, slender, malleable metal probe
- Graduated in centimeters (markings every 1 cm)
- Bulbous tip (to avoid perforating uterus)
- Measure the length and direction of uterine cavity before procedures
- Check uterine position (anteverted/retroverted) before IUD insertion
- Detect uterine anomalies (septum, polyp)
7. Hegar's Dilators
- Set of graduated, cylindrical, blunt-ended metal rods
- Numbered 1-20 (number = diameter in mm)
- Used in pairs (same size for each pass)
- Dilatation of the cervical os before:
- D&C (Dilatation and Curettage)
- Suction evacuation (for incomplete/missed abortion)
- Hysteroscopy
- IUD insertion (if os is tight)
- Cervical incompetence (if forceful over-dilatation)
- Uterine perforation
- Bleeding
8. Uterine Curette (Sharp & Blunt)
- Long-handled instrument with a loop or spoon at the end
- Sharp curette: has a sharp cutting edge
- Blunt curette: smooth edge (safer, used in pregnancy)
- D&C (Dilatation and Curettage):
- Incomplete/missed abortion (remove retained products)
- Endometrial biopsy / sampling
- Gestational trophoblastic disease (molar pregnancy)
- Dysfunctional uterine bleeding (diagnosis + treatment)
- Endometrial carcinoma diagnosis
- Asherman's syndrome - intrauterine adhesions from over-vigorous curettage
- Uterine perforation
- Hemorrhage
9. Ovum Forceps (Polyp Forceps / Ring Forceps)
- Long forceps with oval/ring-shaped, fenestrated (perforated) jaws
- Smooth, atraumatic tips
- Removing products of conception (placental tissue, POC) from uterine cavity
- Removing polyps from uterine cavity
- Grasping and removing foreign bodies from vagina
- Holding swabs during D&C (to clean the cavity)
CATEGORY 3: OBSTETRIC DELIVERY INSTRUMENTS
10. Obstetric Forceps (Simpson's / Wrigley's / Neville-Barnes)
- Paired, articulated metal blades with:
- Cephalic curve - fits the fetal head
- Pelvic curve - follows the birth canal
- Blade, shank, lock, and handle
- Simpson's forceps: long shank, for OA position, low/outlet forceps
- Neville-Barnes: most widely used, for rotational + non-rotational use
- Wrigley's: short, for outlet use (also used at cesarean section)
- Kielland's: straight (no pelvic curve), for rotation of fetal head (e.g., deep transverse arrest)
| Type | Station | Rotation |
|---|---|---|
| Outlet forceps | Scalp visible at introitus | <45° |
| Low forceps | Station ≥+2 cm | <45° or >45° |
| Mid-forceps | Engaged, above +2 cm | Any |
| High forceps | Not engaged | - (abandoned, unsafe) |
- Fully dilated cervix (10 cm)
- Engaged head (station 0 or below)
- Membranes ruptured
- Known position of fetal head
- Empty bladder (catheterize)
- Adequate analgesia
- No CPD (cephalopelvic disproportion)
11. Ventouse (Vacuum Extractor)
- A suction cup (metal or soft silastic) attached to a chain/handle and vacuum pump
- Creates negative pressure (vacuum) of 0.6-0.8 kg/cm² for traction
- Types: Metal cup (Malmstrom), Soft cup (silastic/Silc cup), Hand-held (Kiwi OmniCup)
- Assisted vaginal delivery - alternative to forceps
- When maternal expulsive efforts are inadequate
- Fetal distress in 2nd stage (needs quick delivery)
- Chignon (scalp swelling from cup) - resolves spontaneously
- Cephalohematoma
- Subgaleal hemorrhage (most serious)
- Retinal hemorrhage
- "3 pull rule" - if not delivered in 3 pulls, abandon and proceed to cesarean
12. Episiotomy Scissors (Braun's Scissors)
- Blunt-tipped scissors, slightly angled/curved
- One blade has a rounded point to protect the fetus
- Performing episiotomy (deliberate incision of perineum) during delivery
| Type | Direction | Used when |
|---|---|---|
| Medio-lateral | 45° to right | Standard in most countries, reduces sphincter injury |
| Midline | Straight down | USA, heals better but higher 3rd/4th degree risk |
CATEGORY 4: SURGICAL / OPERATIVE INSTRUMENTS
13. Green-Armytage Forceps
- Large, curved clamps with broad, serrated jaws
- Ring handles
- Control of bleeding from the uterine incision edges at cesarean section
- Grasping uterine angles during uterotomy
- Hemostasis of broad ligament
14. Doyen's Retractor (Bladder Retractor)
- Wide, curved, spatula-like retractor with a handle
- Solid blade with smooth edges
- Retracts the bladder downward during cesarean section (to expose lower uterine segment)
- Retract bladder during hysterectomy, myomectomy
- Protects the bladder during uterine incision
15. Bonney's Myomectomy Clamp (Bonney Clamp)
- Large, curved, atraumatic clamp with broad jaws
- Applied across the broad ligament and uterine vessels
- Reduces blood loss during myomectomy (fibroid removal)
- Compresses uterine vessels temporarily (like a tourniquet)
- Can be left in place for ≤30-45 minutes
16. Colposcope
- Binocular microscope mounted on a stand
- Provides 6-40× magnification of the cervix
- Has a green filter to highlight vascular patterns
- NOT inserted into the body - used externally
- Examination of the transformation zone of the cervix
- Follow-up of abnormal Pap smear / positive HPV test
- Identify CIN (cervical intraepithelial neoplasia)
- Guide directed cervical biopsy
- Detect condylomata, erosions, carcinoma in situ
QUICK OSCE SUMMARY TABLE
| Instrument | Category | Primary Use |
|---|---|---|
| Cusco's speculum | Examination | Cervix visualization, Pap smear |
| Sims' speculum | Examination | VVF repair, anterior wall, needs assistant |
| Pinard's stethoscope | Examination | Fetal heart auscultation |
| Pelvimeter | Examination | Pelvic measurement |
| Vulsellum forceps | Cervical | Grip cervix for procedures |
| Uterine sound | Uterine | Measure uterine cavity length |
| Hegar's dilators | Cervical | Dilate cervical os for D&C |
| Uterine curette | Uterine | D&C - remove endometrium/POC |
| Ovum forceps | Uterine | Remove POC / polyps |
| Obstetric forceps | Delivery | Assisted vaginal delivery |
| Ventouse (vacuum) | Delivery | Assisted delivery, less trauma |
| Episiotomy scissors | Delivery | Controlled perineal incision |
| Green-Armytage forceps | Surgical | Hemostasis at LSCS |
| Doyen's retractor | Surgical | Retract bladder at LSCS |
| Bonney's clamp | Surgical | Reduce blood loss at myomectomy |
| Colposcope | Diagnostic | Examine cervix for CIN/cancer |
HIGH-YIELD OSCE POINTS TO REMEMBER
- Sims' speculum - single blade, needs assistant, used for VVF, patient in Sims' position
- Cusco's speculum - bivalve, self-retaining, routine pelvic exam
- Kielland's forceps - no pelvic curve (straight), used for rotation in deep transverse arrest
- Wrigley's forceps - short, used at cesarean section and outlet delivery
- Ventouse "3 pull rule" - abandon after 3 pulls, do not use <34 weeks gestation
- Hegar's dilators - sequential, by number (number = diameter in mm)
- Uterine sound complication - perforation (most feared)
- Curette complication - Asherman's syndrome (intrauterine adhesions)
- Doyen's retractor - protects bladder at cesarean section
- Green-Armytage - for LSCS uterine angle bleeding
With images
obstetrics gynecology instruments images Cusco speculum Sims Pinard Hegar dilators obstetric forceps ventouse
Cusco speculum Sims speculum Pinard stethoscope Hegar dilator obstetric instruments labeled diagrams
obstetric forceps Simpson Kielland vacuum extractor ventouse Green-Armytage Doyen retractor instrument images
Hegar dilators uterine curette vulsellum forceps uterine sound obstetric instrument photo
vulsellum forceps uterine curette Pinard stethoscope obstetric instrument images Wikipedia commons
Instruments of Obstetrics & Gynecology — With Images
CATEGORY 1: EXAMINATION INSTRUMENTS
1. Cusco's Bivalve Speculum

| Feature | Detail |
|---|---|
| Type | Bivalve, self-retaining |
| Material | Metal or plastic |
| Blades | Open anteroposteriorly |
- Routine cervical/vaginal visualization
- Pap smear / cervical cytology (with Ayre's spatula)
- High vaginal swab
- IUD insertion and removal
- Colposcopy / cervical biopsy
- Detect PROM (pool of liquor in fornix)
2. Sims' Speculum (Single Blade / Double-ended)
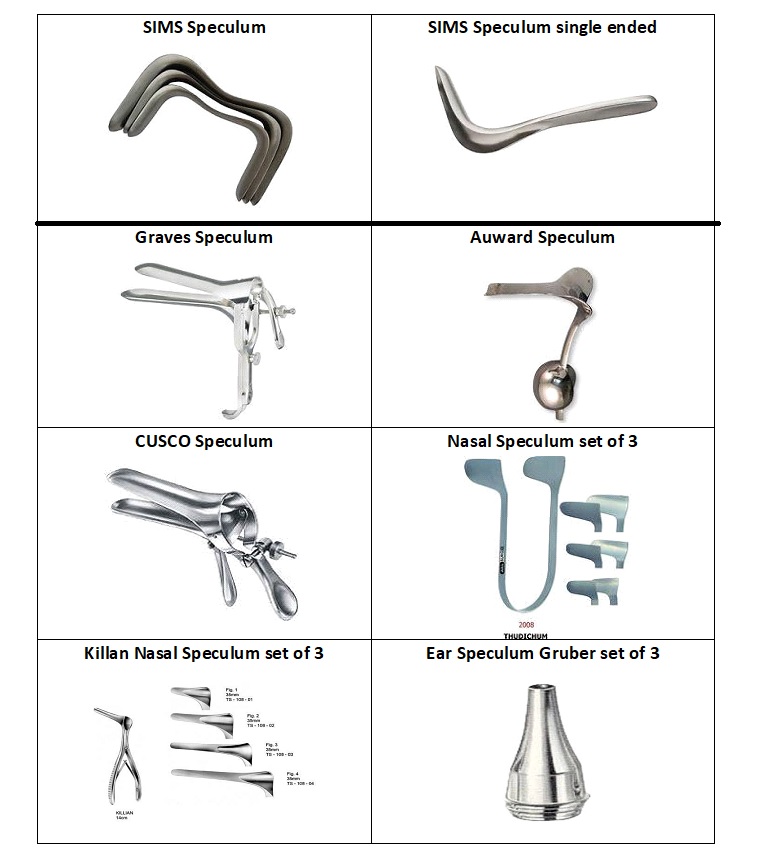
| Feature | Detail |
|---|---|
| Type | Single blade, NOT self-retaining |
| Shape | L-shaped, concave blade with shaft and groove |
| Ends | Double-ended (two different blade widths) |
- Examination of anterior vaginal wall
- Diagnosis and repair of vesicovaginal fistula (VVF)
- Rectovaginal fistula assessment
- Prolapse evaluation
- D&E operations
3. Sims' Speculum (Single Blade) — Close-Up Anatomy

4. Pinard's Fetal Stethoscope
| Feature | Detail |
|---|---|
| Shape | Trumpet/cone shaped, hollow |
| Material | Wood, metal, or plastic |
| Wider end | Applied to maternal abdomen |
| Narrow end | To examiner's ear |
- Auscultate fetal heart rate (normal: 110-160 bpm)
- Monitor fetal wellbeing in labor
- Detect: rate, rhythm, murmurs
CATEGORY 2: CERVICAL & UTERINE INSTRUMENTS
5. Vulsellum Forceps (Jacobs/Museux Type)

| Feature | Detail |
|---|---|
| Tips | Toothed (1×1 or 2×2 sharp teeth) |
| Handles | Ring handles (like scissors) |
| Length | ~25 cm |
| Lock | Ratchet lock |
- Grip and steady the cervix during:
- IUD insertion / removal
- D&C and suction evacuation
- Cervical biopsy
- Manual vacuum aspiration (MVA)
- Traction on cervix for inspection
6. Ovum Forceps (Ring/Polyp Forceps)

| Feature | Detail |
|---|---|
| Tips | Oval/ring-shaped, fenestrated, smooth |
| Handles | Ring handles |
| Jaws | Atraumatic - no teeth |
- Remove products of conception (POC) from uterine cavity
- Remove endometrial polyps
- Remove foreign bodies from vagina
- Hold swabs during D&C
7. Hegar's Dilators (Set)
| Feature | Detail |
|---|---|
| Shape | Cylindrical, blunt-ended metal rods |
| Numbering | 1-20 (number = diameter in mm) |
| Design | Double-ended (different sizes each end) |
| Curvature | Slightly curved in opposite directions from center |
- Sequential cervical dilatation before:
- D&C (dilatation and curettage)
- Suction evacuation (incomplete/missed abortion)
- Hysteroscopy
- IUD insertion (if os is tight)
- Cervical incompetence (over-dilatation)
- Uterine perforation
- Asherman's syndrome (if combined with vigorous curettage)
8. Uterine Curette (Sharp vs. Blunt)
| Type | Feature | Used when |
|---|---|---|
| Sharp curette | Cutting edge loop | Non-pregnant uterus (endometrial biopsy, D&C) |
| Blunt curette | Smooth edge loop | Pregnant uterus (softer, avoids perforation) |
- D&C for incomplete/missed abortion (retained POC)
- Endometrial biopsy / sampling
- Molar pregnancy evacuation
- Diagnosis of AUB / endometrial carcinoma
- Asherman's syndrome treatment
9. Uterine Sound (Sims' Sound)
| Feature | Detail |
|---|---|
| Shape | Long, slender, malleable probe |
| Tip | Bulbous (safety) |
| Markings | Graduated every 1 cm |
| Material | Stainless steel |
- Measure length and axis of uterine cavity before IUD insertion / D&C
- Check uterine position (anteverted / retroverted)
- Detect uterine anomaly (septum, polyp)
CATEGORY 3: OBSTETRIC DELIVERY INSTRUMENTS
10. Obstetric Forceps — Types Compared
| Type | Pelvic Curve | Cephalic Curve | Use |
|---|---|---|---|
| Simpson's | Yes | Yes | OA position, outlet/low forceps, elongated head |
| Wrigley's | Yes (short) | Yes | Outlet forceps, at cesarean section |
| Neville-Barnes | Yes | Yes | Most widely used in UK |
| Kielland's | None (straight) | Yes | Rotation - deep transverse/posterior arrest |
| Piper's | Yes (reversed) | Yes | Aftercoming head in breech delivery |
- Blade (has cephalic curve + pelvic curve)
- Shank (long vs. short)
- Lock (English lock - articulation point)
- Handle (where traction applied)
| Classification | Station | Rotation |
|---|---|---|
| Outlet | Head visible at introitus | ≤45° |
| Low | ≥+2 cm station | Any |
| Mid | Engaged, above +2 cm | Any |
| High | Unengaged | Abandoned |
- Fully dilated cervix (10 cm)
- Fetal head engaged (0 station or below)
- Membranes ruptured
- Fetal position known
- Bladder emptied (catheterize)
- Adequate analgesia
- No CPD
11. Ventouse / Vacuum Extractor
| Type | Cup | Best for |
|---|---|---|
| Malmstrom | Metal | Posterior positions |
| Silastic/soft cup | Soft silicone | Anterior OA position |
| Kiwi OmniCup | Handheld disposable | Occipito-posterior |
- Less maternal perineal trauma
- Less analgesia needed
- Safer in skilled hands for rotation
- Chignon (scalp swelling) - resolves spontaneously
- Cephalohematoma
- Subgaleal hemorrhage (most serious - can be life-threatening)
- Retinal hemorrhage
- Do NOT use <34 weeks gestation (fragile fetal skull)
12. Episiotomy Scissors (Braun's/Straight scissors)
| Feature | Detail |
|---|---|
| Tips | Blunt-tipped (one rounded) |
| Angle | Slightly angled/curved |
| Purpose | Protects fetus during perineal incision |
| Type | Direction | Notes |
|---|---|---|
| Medio-lateral | 45° to right | Standard; reduces 3rd/4th degree tears |
| Midline | Straight posterior | Better healing, but higher sphincter injury risk |
| J-shaped | Midline then lateral | Rarely used |
CATEGORY 4: SURGICAL INSTRUMENTS
13. Green-Armytage Forceps
| Feature | Detail |
|---|---|
| Jaws | Broad, curved, serrated |
| Handles | Ring handles |
| Association | Cesarean section |
- Control bleeding from uterine incision edges at LSCS
- Clamp uterine angles at uterotomy
- Hemostasis of broad ligament during hysterectomy
14. Doyen's Retractor (Bladder Retractor)
| Feature | Detail |
|---|---|
| Shape | Wide, curved spatula |
| Blade | Solid, smooth edges |
| Handle | Lateral handle |
- Retract bladder downward at cesarean section to expose lower uterine segment
- Protect bladder during hysterotomy incision
- Used in hysterectomy and myomectomy
15. Bonney's Myomectomy Clamp
| Feature | Detail |
|---|---|
| Jaws | Large, curved, atraumatic |
| Purpose | Temporary occlusion of uterine blood supply |
- Applied across broad ligament + uterine vessels to reduce blood loss during myomectomy
- Acts as a temporary tourniquet
QUICK VISUAL SUMMARY TABLE
| # | Instrument | Key Visual Feature | Primary Use |
|---|---|---|---|
| 1 | Cusco's speculum | Bivalve, self-retaining, thumbscrew | Cervix visualization, Pap smear |
| 2 | Sims' speculum | Single L-shaped blade, no lock | VVF repair, needs assistant |
| 3 | Pinard's stethoscope | Trumpet shaped, hollow | Fetal heart auscultation |
| 4 | Vulsellum forceps | Long, toothed tips, ring handles | Grip cervix for D&C, IUD |
| 5 | Ovum forceps | Long, ring/oval smooth jaws | Remove POC, polyps |
| 6 | Hegar's dilators | Set of graded metal rods | Dilate cervix for D&C |
| 7 | Uterine sound | Slender, graduated, bulbous tip | Measure uterine length |
| 8 | Uterine curette | Loop-ended handle | D&C - scrape endometrium |
| 9 | Simpson's forceps | Two blades, cephalic + pelvic curve | Outlet/low forceps delivery |
| 10 | Kielland's forceps | No pelvic curve (straight) | Rotation in DTA / OP position |
| 11 | Wrigley's forceps | Short, light | Outlet + at cesarean section |
| 12 | Ventouse cup | Suction cup + vacuum pump | Assisted vaginal delivery |
| 13 | Episiotomy scissors | Blunt, angled | Controlled perineal incision |
| 14 | Green-Armytage | Broad curved jaws | LSCS - uterine angle bleeding |
| 15 | Doyen's retractor | Wide curved spatula | Protect bladder at LSCS |
| 16 | Bonney's clamp | Large atraumatic clamp | Reduce blood loss at myomectomy |
OSCE tip: When shown an instrument, always say:
- Name it
- Describe it (material, parts, special features)
- Uses (list 3-4)
- Contraindications (if any)
- Complications of use
Prolasp instrument
instruments used for uterine prolapse repair surgery gynecology Sims speculum Auvard Hegar dilator OSCE
prolapse instruments Sims speculum Auvard weighted speculum anterior posterior colporrhaphy vaginal hysterectomy retractors images
ring pessary prolapse Heaney retractor Langenbeck retractor vaginal hysterectomy repair instruments images
ring pessary silicone different types prolapse treatment image shelf cube donut
Instruments for Uterovaginal Prolapse
Examination, Non-Surgical & Surgical Instruments with Images
UNDERSTANDING PROLAPSE FIRST
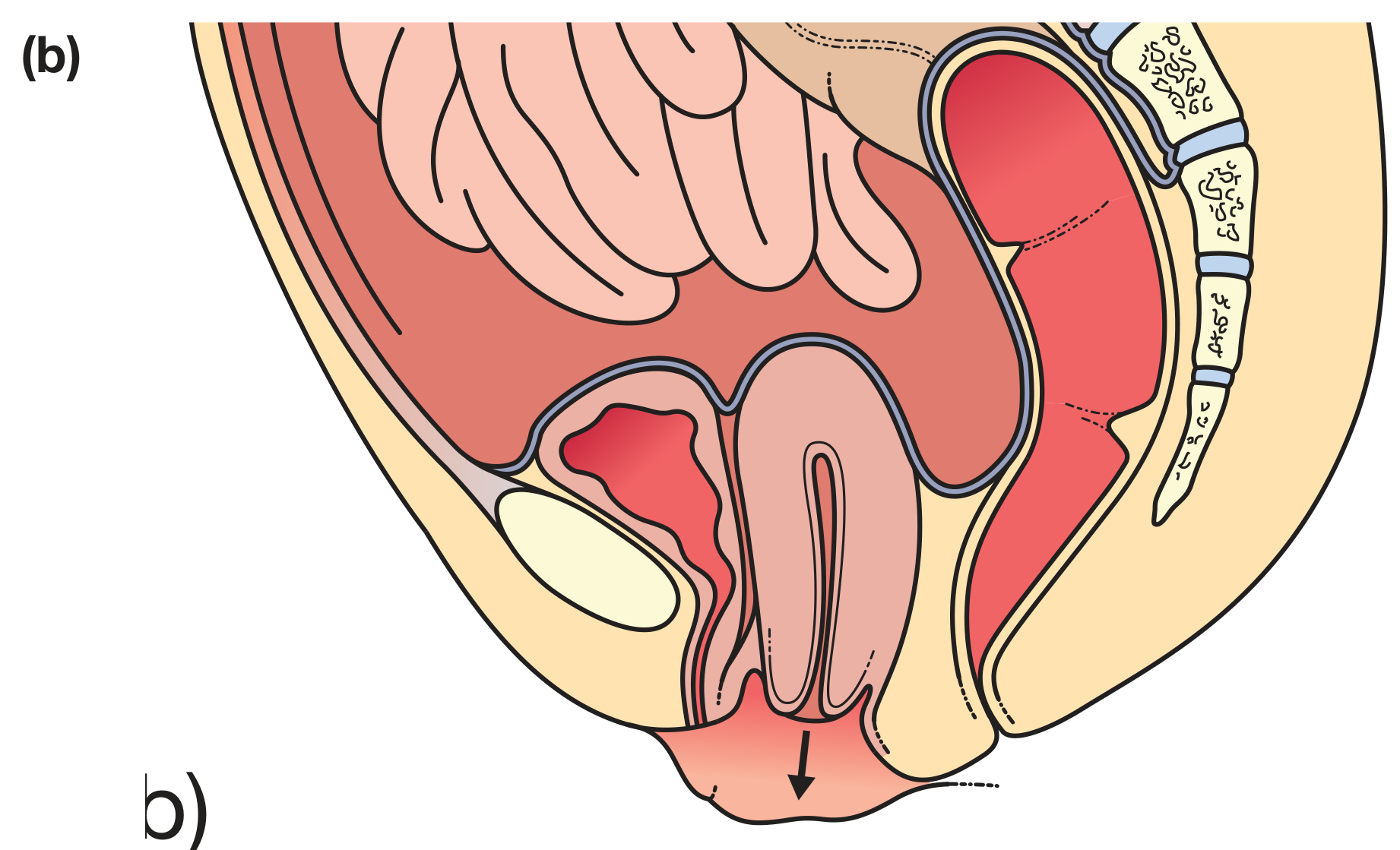
| Grade | Description |
|---|---|
| Grade 0 | No prolapse |
| Grade 1 | Most distal part >1 cm above hymen |
| Grade 2 | ≤1 cm above or below hymen |
| Grade 3 | >1 cm below hymen but not complete |
| Grade 4 | Maximal descent (procidentia) |
- Cystocele - anterior vaginal wall + bladder descends
- Rectocele - posterior vaginal wall + rectum descends
- Urethrocele - urethral descent
- Uterine prolapse - descent of uterus
- Vault prolapse - post-hysterectomy vaginal vault descent
- Enterocele - small bowel herniation into vaginal vault
PART A: EXAMINATION INSTRUMENTS FOR PROLAPSE
1. Sims' Speculum + Auvard Weighted Speculum
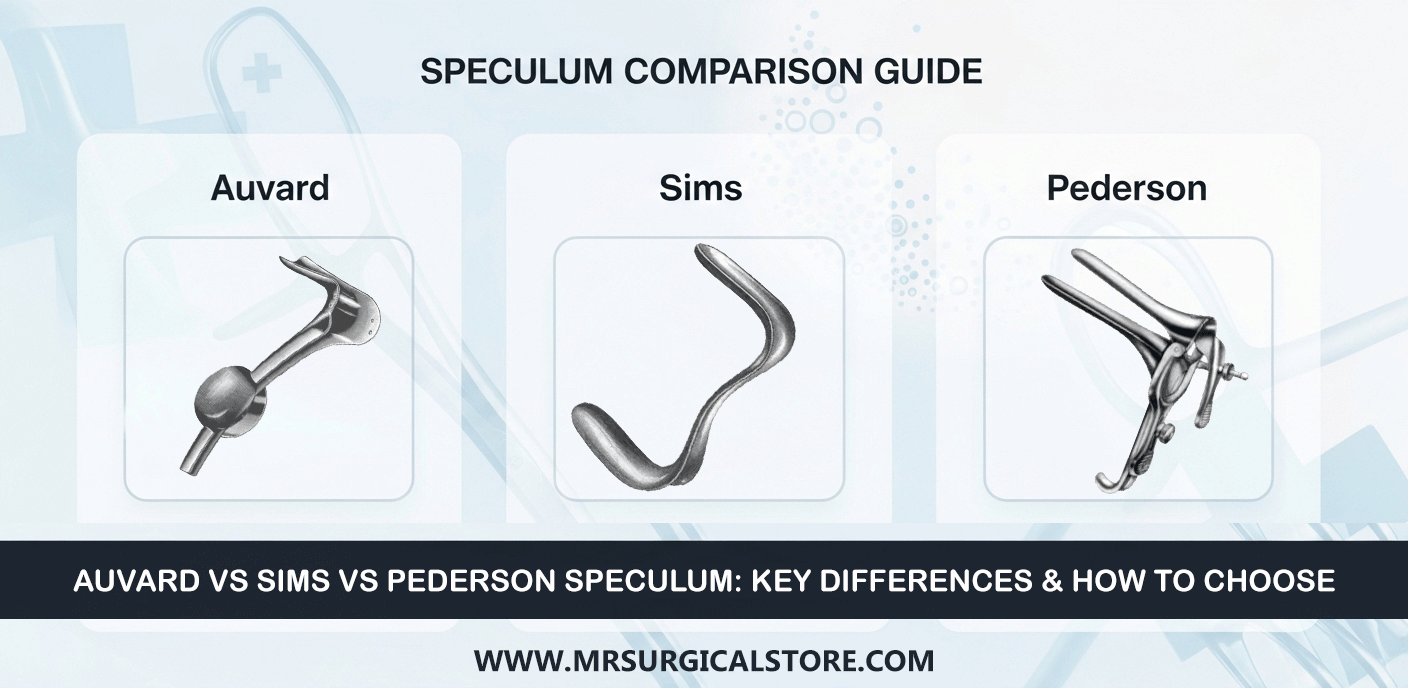
| Speculum | Wall Retracted | Self-Retaining? |
|---|---|---|
| Sims' speculum | Posterior vaginal wall | No - needs assistant |
| Auvard weighted speculum | Posterior vaginal wall | Yes - weight holds it |
2. Auvard Weighted Speculum — Instrument of Choice for Vaginal Surgery

- Single-blade retractor with a heavy ball/weight at its base
- The weight provides self-retraction by gravity
- Blade is broad and concave to cradle the posterior vaginal wall
- Self-retaining posterior retractor during vaginal surgery
- Anterior colporrhaphy (cystocele repair)
- Vaginal hysterectomy
- Posterior colporrhaphy (rectocele repair)
- VVF (vesico-vaginal fistula) repair
PART B: NON-SURGICAL MANAGEMENT - PESSARIES
3. Vaginal Pessaries — Types and Uses
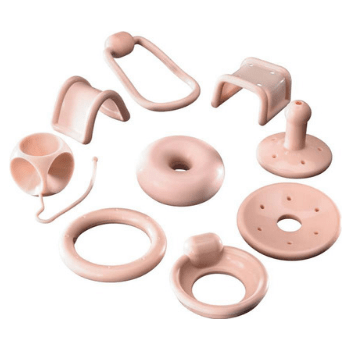
| Pessary | Shape | Best for | Notes |
|---|---|---|---|
| Ring Pessary | Simple ring | Uterine prolapse Grade 1-2 | Most commonly used; inserted between posterior fornix and pubic bone |
| Shelf Pessary | Ring with shelf | Moderate-severe prolapse | Supports vault + anterior wall |
| Donut/Doughnut | Thick inflated ring | Significant prolapse | Larger surface area |
| Gellhorn | Disc with stem | Severe uterovaginal prolapse | Requires removal by clinician |
| Cube | Cube with suction | Vault prolapse, post-hysterectomy | Suction-based hold |
| Hodge Pessary | Oval flat ring | Retroverted uterus, stress incontinence | Repositions uterus anteriorly |
- Patient unfit for surgery
- Grade 1-2 prolapse (conservative)
- Pending surgery
- Patient preference
- During pregnancy
- Vaginal ulceration / erosion
- Discharge and infection
- Difficulty removing (impaction)
- Fistula (if neglected for years)
PART C: SURGICAL INSTRUMENTS FOR PROLAPSE REPAIR
4. Heaney Retractor (Right-Angle Vaginal Retractor)

- Right-angle (J-shaped) retractor
- Flat, broad blade set at 90° to the handle
- Available in various blade widths
- Retracting vaginal walls during vaginal hysterectomy
- Exposing the uterosacral and cardinal ligaments
- Anterior and posterior colporrhaphy
- Essential in every vaginal surgery set
5. Vulsellum / Tenaculum Forceps (for Cervix in Prolapse)
- Used to grasp the cervix and pull down the prolapsed uterus for hysterectomy
- Exposes uterosacral ligaments for ligation
- Multiple-toothed vulsellum preferred for firm grip
6. Instruments for Specific Prolapse Operations
A. Anterior Colporrhaphy (Cystocele Repair)
| Instrument | Purpose |
|---|---|
| Auvard weighted speculum | Posterior wall retraction (self-retaining) |
| Sims' retractor | Lateral wall retraction |
| Allis tissue forceps | Grasp anterior vaginal wall flaps |
| Scissors (curved) | Incise anterior vaginal wall |
| Hegar dilators | Pre-op cervical dilatation if needed |
| Absorbable sutures (Vicryl 2-0) | Plication of pubocervical fascia |
B. Posterior Colporrhaphy (Rectocele Repair)
| Instrument | Purpose |
|---|---|
| Auvard speculum | Posterior wall retraction |
| Allis forceps | Grasp posterior vaginal wall |
| Scissors | Incise posterior vaginal wall |
| Absorbable sutures | Levatorplasty (pelvic floor repair) |
C. Vaginal Hysterectomy (for Uterine Prolapse)
| Instrument | Purpose |
|---|---|
| Auvard weighted speculum | Posterior wall retraction |
| Multiple-toothed vulsellum | Grip and pull cervix |
| Heaney retractors (pair) | Expose operative field |
| Heaney clamps | Clamp uterine vessels (cardinal + uterosacral ligaments) |
| Long scissors | Cut pedicles |
| Long needle holder | Suture deep pedicles |
| Uterine sound | Pre-op uterine length measurement |
D. Manchester Repair (Fothergill's Operation) — For Cervical Elongation with Prolapse
| Instrument | Purpose |
|---|---|
| Vulsellum | Grip elongated cervix |
| Auvard speculum | Exposure |
| Amputation knife/scissors | Amputation of elongated cervix |
| Hegar dilators | Dilate endocervix |
| Sutures | Attach cardinal ligaments to cervical stump (Sturmdorf sutures) |
PART D: SPECIAL INSTRUMENTS
7. Perineorrhaphy / Perineoplasty Instruments (Perineal Body Repair)
| Instrument | Purpose |
|---|---|
| Allis forceps | Mark corners of perineal incision |
| Mayo scissors | Excise perineal skin |
| Needle holder | Deep suturing of levator ani muscles |
| Vicryl 2-0 sutures | Plication of perineal body |
QUICK OSCE REFERENCE
| Instrument | Used In | Key Feature |
|---|---|---|
| Sims' speculum | Prolapse examination | Single blade, needs assistant |
| Auvard speculum | All vaginal surgery | Self-retaining, weighted ball |
| Ring pessary | Conservative prolapse Mx | Most common pessary, replaced 3-6 monthly |
| Gellhorn pessary | Severe prolapse | Disc + stem, needs clinician to remove |
| Heaney retractor | Vaginal hysterectomy | Right-angle J-shape |
| Vulsellum | Pull cervix in VH + Manchester | Toothed tips |
| Heaney clamp | Ligate uterine pedicles | Used in VH |
| Allis forceps | Grasp vaginal wall flaps | Colporrhaphy |
OSCE KEY POINTS TO REMEMBER
- Auvard = the single most important instrument for ALL vaginal prolapse surgery - self-retaining, weighted, retracts posterior wall
- Sims' position (left lateral) + Sims' speculum = classic position for examining prolapse
- Ring pessary = first-line non-surgical Rx for grade 1-2 prolapse; change every 3-6 months
- Manchester repair = amputation of cervix + cardinal ligament plication - uterus preserved
- Vaginal hysterectomy = definitive surgical treatment for uterine prolapse when uterus not needed
- Anterior colporrhaphy = cystocele repair; posterior colporrhaphy = rectocele repair; perineorrhaphy = perineal body repair
- POP-Q Grade 4 = procidentia (complete uterovaginal prolapse) = surgical emergency if ulcerated