Give me pathway of facial nerve from cortex to end of the nerve give photo
Reading File
Finding Sources
Finding Sources
Searching the Web
facial nerve pathway cortex to periphery anatomy diagram
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive content and images from multiple authoritative textbooks. Here is the complete answer:
Facial Nerve (CN VII) - Complete Pathway: Cortex to End Organ
1. CORTICAL ORIGIN (Upper Motor Neuron)
The motor command for facial movement originates in the lower third of the primary motor cortex (precentral gyrus), in the face representation area of the homunculus.
- Upper face (forehead, orbicularis oculi): Receives bilateral cortical input - both crossed and uncrossed corticobulbar fibers. This is why forehead wrinkling is spared in upper motor neuron (UMN) lesions (e.g., internal capsule stroke).
- Lower face (mouth, lips, cheeks): Receives predominantly contralateral (crossed) input only.
The corticobulbar fibers descend through the genu of the internal capsule, then through the cerebral peduncles and pons to reach the facial motor nucleus.

Diagram showing upper face receives bilateral cortical input; lower face receives only contralateral input - explaining UMN vs LMN pattern of weakness
2. BRAINSTEM NUCLEI (Three Nuclei)
Three nuclei give rise to the fibers of CN VII (Shambaugh Surgery of the Ear):
| Nucleus | Location | Fiber Type | Function |
|---|---|---|---|
| Facial motor nucleus | Caudal pons | Special visceral efferent (SVE) | Muscles of facial expression, stapedius, stylohyoid, posterior digastric |
| Superior salivatory nucleus | Dorsal to motor nucleus, pons | General visceral efferent (GVE) | Lacrimal gland, submandibular & sublingual glands, nasal seromucinous glands |
| Nucleus of the solitary tract (NTS) | Medulla oblongata | Special visceral afferent (SVA) | Taste - anterior 2/3 tongue |
Key nuclear feature: The motor fibers loop around the abducens (CN VI) nucleus, forming the facial colliculus (visible bump on the floor of the 4th ventricle).

Complete schematic: Brainstem nuclei, nervus intermedius, and all peripheral branches of CN VII
3. INTRACRANIAL SEGMENT (~24 mm)
- Exits the pons at the cerebellopontine angle (CPA) - the pontomedullary junction, lateral aspect
- Travels with the nervus intermedius (carrying parasympathetic + taste fibers) and CN VIII
- Enters the internal auditory meatus (porus acousticus)
- Length: ~24 mm from the pontomedullary sulcus to the porus of the internal auditory canal (IAC)
- At this point the nerve lacks a fibrous sheath (no epineurium) and is covered only by arachnoid
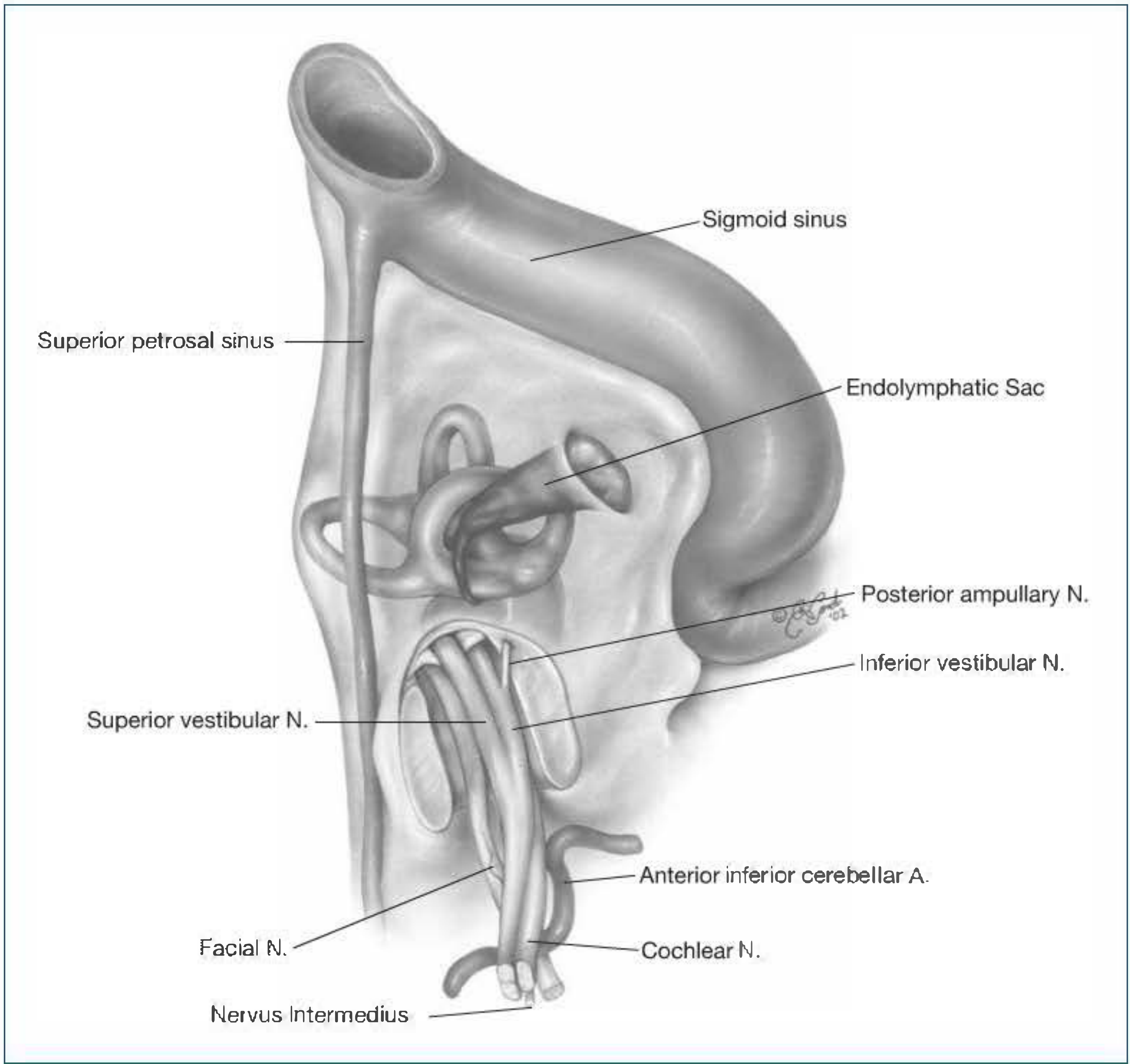
Facial N., Nervus Intermedius, and Cochlear N. at the CPA and IAC - Shambaugh Surgery of the Ear
4. INTRACANALICULAR SEGMENT (within the IAC)
- Traverses the internal auditory canal
- At the fundus of the IAC, the facial nerve occupies the anterosuperior quadrant (Bill's bar separates it from the superior vestibular nerve above)
- The nervus intermedius joins here
- Enters the fallopian canal (bony canal) at the fundus
5. INTRATEMPORAL SEGMENTS (Fallopian Canal)
The nerve runs within the bony fallopian canal through the temporal bone. It is divided into three segments (Cummings Otolaryngology; Shambaugh Surgery of the Ear):
A. Labyrinthine Segment (~4 mm)
- Shortest and narrowest segment of the entire facial nerve
- Runs from the fundus of the IAC to the geniculate ganglion, superior to the cochlea
- Opens into the geniculate fossa (just deep to the suprameatal ridge)
- Contains the geniculate ganglion - cell bodies of taste and somatic sensory neurons
- Bone here is thin and often dehiscent (~25% of ears)
- First branch given off: Greater Superficial Petrosal Nerve (GSPN)
- Exits at the facial hiatus, runs along the middle fossa floor
- Carries preganglionic parasympathetics to the pterygopalatine ganglion → lacrimal gland and nasal glands
B. Tympanic (Horizontal) Segment (~13 mm)
- Begins at the 1st genu (at the geniculate ganglion) - nerve turns sharply posteriorly ~90°
- Runs in the medial wall of the tympanic cavity (middle ear)
- Courses superior to the cochleariform process and superior to the oval window niche
- Most common site of congenital dehiscence of the bony canal (especially above the oval window)
- Second branch: Nerve to stapedius (emerges near the pyramidal eminence)
C. Mastoid (Vertical) Segment (~20 mm)
- Begins at the 2nd genu at the pyramidal eminence (just anteroinferior to the lateral semicircular canal)
- Descends vertically through the mastoid bone
- Third branch: Chorda tympani - arises midway in the descending portion
- Re-enters the middle ear, crosses the tympanic membrane (between malleus and incus)
- Exits via the petrotympanic fissure to join the lingual nerve
- Carries taste from anterior 2/3 tongue + preganglionic parasympathetics to submandibular ganglion → submandibular and sublingual glands
- Terminates at the stylomastoid foramen
6. EXTRATEMPORAL SEGMENT (outside the temporal bone)
The nerve exits the skull at the stylomastoid foramen, then:
- Posterior auricular nerve - first extratemporal branch, supplies occipitalis, posterior auricular muscles
- Branch to posterior belly of digastric
- Branch to stylohyoid muscle
The main trunk then enters the parotid gland (without innervating it - parotid secretomotor supply is from CN IX via the otic ganglion).
Within the parotid, it divides at the pes anserinus ("goose's foot") into:
- Upper division (temporofacial trunk)
- Lower division (cervicofacial trunk)
Five Terminal Branches (mnemonic: To Zanzibar By Motor Car):
| Branch | Muscles Innervated |
|---|---|
| Temporal | Frontalis, orbicularis oculi (upper), corrugator supercilii, procerus |
| Zygomatic | Orbicularis oculi (lower), zygomaticus (most important for eye closure and smile) |
| Buccal | Buccinator, orbicularis oris, zygomaticus major, levator labii |
| Marginal mandibular | Depressors of lower lip, mentalis |
| Cervical | Platysma |
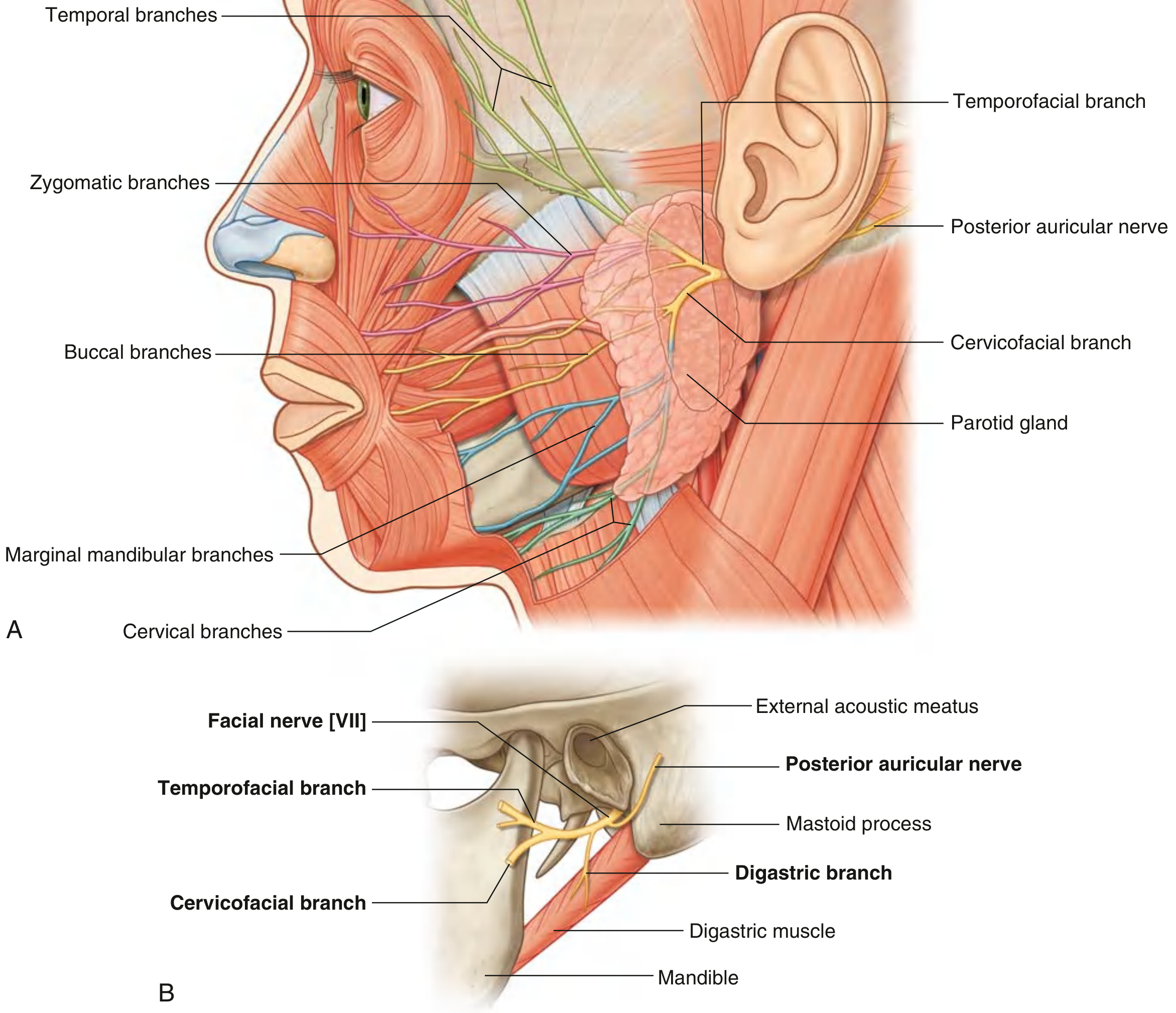
(A) All five terminal branches labeled on the face. (B) The pes anserinus division at the stylomastoid foramen - Gray's Anatomy for Students
Summary: Complete Pathway at a Glance
Primary Motor Cortex (precentral gyrus, lower 1/3)
↓ Corticobulbar tract
Genu of Internal Capsule → Cerebral peduncle → Pons
↓
Facial Motor Nucleus (caudal pons) + Superior Salivatory Nucleus + NTS
↓
Loops around CN VI nucleus (facial colliculus) → exits at CPA (pontomedullary junction)
↓ Intracranial segment (24 mm)
Internal Auditory Canal (IAC) - anterosuperior quadrant at fundus
↓
Fallopian Canal begins:
[1] Labyrinthine segment (4 mm) → Geniculate ganglion → GSPN branch given off
[2] 1st genu → Tympanic/Horizontal segment (13 mm) → Stapedius nerve branch
[3] 2nd genu → Mastoid/Vertical segment (20 mm) → Chorda tympani branch
↓
Stylomastoid foramen
↓ Posterior auricular nerve, digastric branch, stylohyoid branch
Parotid gland → Pes anserinus division
↓
5 terminal branches: Temporal | Zygomatic | Buccal | Marginal mandibular | Cervical
↓
Muscles of facial expression + stapedius + stylohyoid + posterior digastric
Key Clinical Points:
- UMN lesion (e.g., cortical stroke): Contralateral lower face weakness; forehead spared (bilateral cortical supply)
- LMN lesion (e.g., Bell's palsy, acoustic neuroma): Ipsilateral entire hemiface weakness including forehead
- Bell's palsy typically involves the geniculate ganglion / labyrinthine segment (reactivation of HSV-1), causing facial palsy + possible hyperacusis + loss of taste + dry eye
Sources: Cummings Otolaryngology Head & Neck Surgery; Shambaugh Surgery of the Ear; Gray's Anatomy for Students; Neuroanatomy through Clinical Cases, 3rd Edition
What happen if there is lesion in cortex n internal capsule
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Now I have everything needed. Here is the complete detailed answer:
Lesion of Cortex / Internal Capsule - Upper Motor Neuron (UMN) Facial Palsy
The Core Concept: WHY the Forehead is Spared
This is the single most important concept to understand. Recall from the facial nerve pathway:
- Upper face neurons (frontalis, orbicularis oculi) in the facial motor nucleus receive bilateral corticobulbar input - both from the ipsilateral AND contralateral cortex
- Lower face neurons (muscles around the mouth) receive predominantly contralateral (crossed) input only
So when the cortex or internal capsule on one side is damaged:
- The lower face loses its only cortical input → weakness
- The upper face still has intact input from the other hemisphere → spared
What Happens: Feature by Feature
1. Pattern of Facial Weakness
| Area of Face | Effect | Reason |
|---|---|---|
| Forehead (frontalis) | SPARED - can still wrinkle | Bilateral cortical supply intact from opposite side |
| Orbicularis oculi | RELATIVELY SPARED - can still close eye | Also has bilateral innervation |
| Lower face (mouth, lips, cheeks) | WEAK/PARALYZED | Only contralateral input - now lost |
| Muscles around mouth | Most severely affected | Predominantly crossed input |
"With supranuclear lesions, there is paresis of voluntary movements of the muscles of facial expression contralateral to the affected hemisphere, with relative sparing of the frontalis and orbicularis oculi. The muscles around the mouth are especially affected." - Localization in Clinical Neurology, 8e
2. Side of Weakness
Contralateral to the lesion - because corticobulbar fibers cross before reaching the facial nucleus in the pons.
- Left cortex/internal capsule lesion → Right lower face weakness
3. Voluntary vs. Emotional Facial Movement - Important Dissociation
This is a very clinically important and frequently examined point:
| Type | Pathway | Effect of Cortex/IC Lesion |
|---|---|---|
| Voluntary facial movement | Corticobulbar tract → internal capsule → facial nucleus | LOST - patient cannot voluntarily show teeth or smile on command |
| Emotional/involuntary facial movement | SMA + cingulate cortex → does NOT pass through internal capsule | PRESERVED - patient may still smile naturally when happy or laugh |
"Volitional facial paresis without emotional is far more common... and results from interruption of corticobulbar pathways due to lesions of the lower precentral gyrus, internal capsule, cerebral peduncle, or upper pons. The reverse pattern - emotional facial paresis without volitional - is observed with lesions anterior to the precentral gyrus, especially the right hemisphere." - Localization in Clinical Neurology, 8e
"Fibers mediating emotional facial movements do NOT descend in the internal capsule in their course to the facial motor nuclei." - Localization in Clinical Neurology, 8e
This is why the patient with an internal capsule stroke can smile when they hear a joke but cannot voluntarily "show their teeth" on command - the voluntary (corticobulbar) pathway is damaged but the emotional pathway is intact.
Cortex vs. Internal Capsule: Differences
| Feature | Cortical Lesion | Internal Capsule Lesion |
|---|---|---|
| Facial weakness | Contralateral lower face | Contralateral lower face |
| Limb involvement | Often restricted to face + arm OR face + leg (somatotopic) | Usually face + arm + leg (pure motor hemiplegia - all fibers packed tightly together) |
| Sensory loss | May be present (if parietal cortex involved) | Usually ABSENT in pure IC lesion |
| Aphasia | May be present (dominant hemisphere) | Absent |
| Dysarthria | May be present | Common (dysarthria-clumsy hand syndrome) |
| Neglect/apraxia | May be present | Absent |
| Pattern | More restricted, focal deficits | "Pure motor hemiparesis" - face + arm + leg |
"Pure motor hemiplegia - without sensory abnormalities or cortical signs such as aphasia or neglect - can be localized to the contralateral corticobulbar and corticospinal tracts, most commonly in the internal capsule." - Neuroanatomy through Clinical Cases, 3rd Ed.
Associated Signs (UMN Pattern)
Because the corticobulbar and corticospinal tracts run together through the internal capsule:
- Hemiparesis/hemiplegia - contralateral face, arm, and leg
- Hyperreflexia - contralateral limbs (may be absent acutely - "spinal shock" equivalent)
- Upgoing plantar (Babinski sign) - contralateral
- Spasticity - develops over weeks (UMN release phenomenon)
- Dysarthria - from weakness of lip and tongue muscles
- No Bell's phenomenon - eye can still close (orbicularis spared)
- No loss of taste, no dry eye, no hyperacusis - these require actual facial nerve damage (LMN)
Bilateral UMN Lesions (Pseudobulbar Palsy)
When BOTH internal capsules or both cortical face areas are damaged:
- Bilateral facial diplegia - weakness of both sides
- Spastic dysarthria ("Donald Duck" speech)
- Dysphagia
- Pseudobulbar affect - pathological laughing and crying disproportionate to emotion (uninhibited, uncontrollable)
- Brisk jaw jerk
Summary Comparison: UMN vs. LMN Facial Palsy
| Feature | UMN (Cortex/IC lesion) | LMN (Bell's palsy/CN VII lesion) |
|---|---|---|
| Forehead | Spared | Involved (whole face) |
| Side | Contralateral | Ipsilateral |
| Voluntary smile | Weak | Weak |
| Emotional smile | Preserved | Weak |
| Taste | Normal | May be lost |
| Lacrimation | Normal | May be reduced |
| Hyperacusis | Absent | May be present |
| Associated signs | Hemiparesis, Babinski | Isolated CN VII |
| Cause | Stroke (MCA/lenticulostriate), tumor, MS | Viral (HSV-1), trauma, tumor, otitis media |
Common Causes of Cortex/Internal Capsule Lesions Causing This Pattern
- Ischemic stroke - most common; internal capsule supplied by lenticulostriate arteries (branches of proximal MCA) → lacunar infarcts
- Hemorrhage - hypertensive bleed into internal capsule or basal ganglia
- Tumor - infiltrating the motor strip or IC
- Demyelination (MS) - plaque in corona radiata or IC
- Trauma - cortical contusion
Sources: Localization in Clinical Neurology 8e; Neuroanatomy through Clinical Cases 3rd Ed.; Frameworks for Internal Medicine; Wills Eye Manual
I understood about facial nerve lesion Tell about cortical n internal capsule signs or symptoms
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Now I have excellent material from multiple authoritative textbooks. Here is the complete answer:
Signs & Symptoms: Cortical vs. Internal Capsule Lesions
The Fundamental Difference
The key to understanding these two locations is anatomy of fiber density:
- Cortex: Motor fibers are spread out over a large area (the homunculus). A small lesion hits only part of the body map.
- Internal capsule: ALL motor and sensory fibers from the entire cortex converge into a tiny compact bundle. Even a tiny lesion hits everything - face + arm + leg equally.
1. CEREBRAL CORTEX LESION
Motor Signs
- Weakness is focal and disproportionate - follows the homunculus
- A small lesion causes weakness of only one body part (e.g., just the hand, just the face, just the leg)
- Full hemiplegia (arm + leg) requires a large, extensive cortical lesion (e.g., entire MCA territory)
- MCA territory (lateral cortex): face + arm + hand most affected; leg relatively spared
- ACA territory (parasagittal): leg most affected; arm and face spared
- Arm extensors and leg flexors preferentially weak (UMN pattern)
The "Cortical Signs" - Hallmark of Cortical Lesions
These are signs that are ONLY present with cortical damage, NOT with pure internal capsule lesions:
| Sign | Description | Hemisphere |
|---|---|---|
| Aphasia | Broca's (expressive) - lesion in posterior frontal; Wernicke's (receptive) - lesion in superior temporal | Dominant (Left) |
| Neglect / Hemispatial inattention | Patient ignores contralateral half of space | Non-dominant (Right) |
| Apraxia | Cannot perform learned motor tasks (e.g., "show me how to comb hair") | Dominant |
| Agraphesthesia | Cannot identify number written on skin | Parietal cortex |
| Astereognosis | Cannot identify object by touch alone | Parietal cortex |
| 2-point discrimination loss | Cortical sensory loss | Parietal cortex |
| Homonymous hemianopia | Visual field cut (optic radiations in deep white matter) | Either |
| Seizures | Cortical irritation → focal/Jacksonian seizures | Either |
| Todd's (postictal) paralysis | Transient hemiparesis after a seizure | Either |
| Gerstmann syndrome | Acalculia + agraphia + finger agnosia + left-right disorientation | Dominant parietal |
"Lesions of the cerebral cortex often result in disorders of language and visual-spatial integration (neglect), cortical sensory disturbances (agraphesthesia), apraxia, and seizure. The presence of any of these findings in addition to hemiparesis is suggestive of a lesion within the cerebral cortex." - Frameworks for Internal Medicine
Sensory Signs (Cortical)
- Contralateral hemisensory loss - primary sensory cortex (parietal)
- Mainly cortical/discriminative sensations lost: 2-point discrimination, stereognosis, graphesthesia, proprioception
- Basic pain/temperature may be intact (thalamus handles those)
2. INTERNAL CAPSULE LESION
Structure of the Internal Capsule - Recap
[Caudate nucleus] [Lentiform nucleus (Putamen + Globus pallidus)]
\ /
Anterior limb Genu Posterior limb
| | |
Frontopontine Corticobulbar Corticospinal
fibers (face) (arm + leg)
+ Sensory radiations
+ Optic radiations
Signs by Location Within the Internal Capsule
| Part | Fibers | Signs if Damaged |
|---|---|---|
| Anterior limb | Frontopontine + thalamocortical | Minimal motor deficit; cognitive/emotional changes |
| Genu | Corticobulbar fibers (face, tongue) | Contralateral lower face + tongue weakness, dysarthria |
| Posterior limb (anterior part) | Corticospinal (arm > leg) | Contralateral hemiparesis (arm prominent) |
| Posterior limb (posterior part) | Corticospinal (leg) + sensory thalamic radiations | Hemiparesis + hemisensory loss |
| Retrolenticular | Optic radiations | Contralateral homonymous hemianopia |
| Sublenticular | Auditory radiations, temporopontine | Auditory changes |
Classic Internal Capsule Lesion (Posterior Limb): Pure Motor Hemiplegia
This is the textbook presentation:
- Contralateral hemiplegia - face + arm + leg equally affected (proportionate)
- No sensory loss (if lesion spares the posterior part of posterior limb)
- No aphasia, no neglect, no agnosia (no cortical signs)
- Dysarthria - common (corticobulbar fibers at the genu)
- Hyperreflexia + Babinski sign contralaterally
- Spasticity develops over days-weeks
"More caudally, the descending motor fibers converge in the posterior limb of the internal capsule, so that even a small lesion there will cause pure motor hemiplegia in which the face, arm, hand, leg, and foot are affected to approximately the same degree." - Adams & Victor's Neurology, 12th Ed.
Lacunar Syndromes of the Internal Capsule (Classic 4)
These are small strokes (lacunes) caused by occlusion of lenticulostriate arteries in hypertension/diabetes:
| Syndrome | Location | Features |
|---|---|---|
| Pure motor hemiparesis (most common, 50-66% of lacunes) | Posterior limb IC / basis pontis / corona radiata | Contralateral face + arm + leg weakness. NO sensory loss, NO cortical signs |
| Pure sensory stroke | Lateral thalamus (not IC) | Contralateral hemisensory loss only |
| Dysarthria-clumsy hand syndrome | Genu of IC / basis pontis | Slurred speech + contralateral hand clumsiness (minimal) |
| Ataxic hemiparesis | Posterior limb IC / basis pontis | Contralateral weakness + ipsilateral ataxia (out of proportion to weakness) |
Side-by-Side Comparison Table
| Feature | Cortical Lesion | Internal Capsule Lesion |
|---|---|---|
| Weakness distribution | Focal/partial (face, arm OR leg, rarely full hemi) | Full contralateral hemiplegia - face + arm + leg equally |
| Facial weakness | Contralateral lower face | Contralateral lower face |
| Aphasia | YES (dominant hemisphere) | NO |
| Neglect | YES (non-dominant) | NO |
| Apraxia | YES | NO |
| Cortical sensory loss | YES (if parietal) | Usually NO |
| Hemianopia | Sometimes | Rarely (retrolenticular only) |
| Seizures | YES (cortical irritation) | NO |
| Dysarthria | Sometimes | YES (genu involvement) |
| Babinski | YES (contralateral) | YES (contralateral) |
| Hyperreflexia | YES | YES |
| Spasticity | YES (delayed) | YES (delayed) |
| Bladder/bowel | May be affected (frontal) | Usually spared |
| Cause | Large MCA stroke, tumor, abscess, MS | Lacunar infarct (hypertension), small hemorrhage |
| Vessel involved | MCA, ACA, PCA cortical branches | Lenticulostriate arteries (branches of proximal MCA) |
Quick Memory Aid
CORTEX lesion = Focal weakness + CORTICAL SIGNS (AAAN)
• Aphasia
• Agnosia (astereognosis, agraphesthesia)
• Apraxia
• Neglect
+ Seizures possible
INTERNAL CAPSULE = PURE MOTOR HEMIPLEGIA (face + arm + leg)
• NO cortical signs
• Dysarthria common
• Tiny lesion = BIG deficit (all fibers packed together)
Sources: Adams & Victor's Principles of Neurology 12th Ed.; Localization in Clinical Neurology 8e; Bradley & Daroff's Neurology in Clinical Practice; Frameworks for Internal Medicine; Harrison's Principles of Internal Medicine 22e
Hyperacusis
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I have all the information needed for a thorough answer. Here it is:
Hyperacusis
Definition
Hyperacusis is an abnormal, painful sensitivity to ordinary sounds - sounds that most people tolerate comfortably become uncomfortably loud or even painful to the affected patient. In the context of the facial nerve, it specifically means the patient finds normal everyday sounds (rattling keys, a ringing phone, background noise) painfully loud in the affected ear.
Mechanism - Why Does It Happen?
Normal physiology of the stapedius muscle:
The stapedius is a tiny muscle in the middle ear, attached to the neck of the stapes bone. It is the smallest skeletal muscle in the body. Its function:
- When a loud sound arrives, the stapedius reflexively contracts (the acoustic/stapedial reflex)
- This contraction stiffens the ossicular chain (malleus-incus-stapes)
- A stiffer chain transmits less energy to the cochlea - it dampens the sound
- This protects the inner ear from overstimulation by loud sounds
What happens when the facial nerve is damaged:
The nerve to stapedius is a branch of CN VII. It arises from the mastoid (vertical) segment, just below the second genu.
When this branch (or the facial nerve proximal to it) is damaged:
- Stapedius is paralyzed - it cannot contract
- The ossicular chain remains loose/floppy even when loud sounds arrive
- Sound vibrations are transmitted to the cochlea without any damping
- Normal sounds are perceived as excessively loud and distorted
- Patient describes sounds as "booming," "tinny," or uncomfortably loud in that ear
"Because the stapedius muscle dampens vibration of the stapes bone in the middle ear, paralysis of the facial nerve usually also includes hyperacusis on the ipsilateral side." - Rheumatology (Elsevier)
"In patients with injury to the facial nerve (e.g., Bell's palsy), the stapedial reflex is impaired, and the patient complains that sounds in that ear have a 'booming' quality (hyperacusis)." - Kandel's Principles of Neural Science, 6th Ed.
Localizing Value of Hyperacusis
This is where hyperacusis becomes extremely important clinically - it helps localize exactly where along the facial nerve the lesion is:
PROXIMAL DISTAL
Geniculate ──────────────────────────────────────────────────────►
ganglion Labyrinthine │ Tympanic │ Nerve to │ Chorda │ Stylomastoid
│ │ Stapedius │ Tympani │ Foramen
│ │ (branch) │ (branch) │
| Lesion Location | Facial Palsy | Hyperacusis | Taste Loss | Dry Eye (↓ lacrimation) |
|---|---|---|---|---|
| CPA (cerebellopontine angle) e.g., acoustic neuroma | Yes | No | Yes | Yes |
| Meatal/IAC segment | Yes | No | Yes | Yes |
| Labyrinthine / Geniculate ganglion e.g., Bell's palsy, Ramsay Hunt | Yes | YES | Yes | Yes |
| Tympanic segment (proximal to nerve to stapedius) | Yes | YES | Yes | Depends |
| Between nerve to stapedius & chorda tympani | Yes | NO (stapedius intact) | Yes | No |
| Below chorda tympani / near stylomastoid foramen | Yes | No | No | No |
| Distal to stylomastoid foramen (parotid) | Yes | No | No | No |
The key rule:
Hyperacusis = lesion is PROXIMAL to the nerve to stapedius branch No hyperacusis = lesion is DISTAL to the nerve to stapedius branch
"Lesions within this segment of the facial nerve (proximal to nerve to stapedius) result in ipsilateral peripheral facial paralysis, impaired taste, and hyperacusis." - Localization in Clinical Neurology, 8e
"Lesions within the facial canal between the exit of the nerve to stapedius and the exit of the chorda tympani cause facial paralysis and impaired taste - but as the lesion is DISTAL to the nerve to stapedius, hearing is SPARED." - Localization in Clinical Neurology, 8e
In Bell's Palsy
Bell's palsy (viral reactivation at the geniculate ganglion/labyrinthine segment) classically produces the full triad:
- Ipsilateral LMN facial palsy (entire half face including forehead)
- Hyperacusis (nerve to stapedius affected - proximal to it)
- Loss of taste on anterior 2/3 tongue (chorda tympani affected)
- Decreased lacrimation (GSPN affected - proximal to it)
- Retroauricular pain (somatic sensory component of CN VII)
The presence of all four features confirms a lesion at or proximal to the geniculate ganglion.
Acoustic Reflex Testing
In clinical practice, the stapedial (acoustic) reflex is tested formally using tympanometry:
- A loud tone is delivered to one ear
- Impedance change from stapedius contraction is measured in the other ear (or same ear)
- Absent acoustic reflex on the ipsilateral side = stapedius paralysis = confirms hyperacusis/CN VII lesion proximal to nerve to stapedius
- This is an objective test - does not rely on patient reporting
Quick Summary
Stapedius (CN VII branch) → contracts → dampens ossicular chain → protects cochlea
Facial nerve lesion → stapedius paralysis → no dampening → all sounds amplified
→ HYPERACUSIS
Localizing value:
Hyperacusis PRESENT → Lesion ABOVE nerve to stapedius (geniculate, labyrinthine, IAC, CPA*)
Hyperacusis ABSENT → Lesion BELOW nerve to stapedius (mastoid segment distal, parotid)
*CPA lesions: usually NO hyperacusis because stapedius branch is spared at that level
Sources: Neuroanatomy through Clinical Cases 3rd Ed.; Localization in Clinical Neurology 8e; Kandel's Principles of Neural Science 6th Ed.; Rheumatology (Elsevier); Adams & Victor's Principles of Neurology 12th Ed.
Stapedial reflex
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
All the information I need is now available. Here is the complete answer:
Stapedial (Acoustic) Reflex
What It Is
The stapedial reflex (also called the acoustic reflex or middle ear muscle reflex) is a bilateral, involuntary protective reflex of the middle ear. When a sufficiently loud sound is heard in either ear, both stapedius muscles contract simultaneously, stiffening the ossicular chains in both ears to protect the cochlea from damage by intense sounds.
Anatomy Recap: The Stapedius Muscle
- Smallest skeletal muscle in the human body
- Attached to the neck of the stapes (third ossicle)
- Housed inside the pyramidal eminence on the posterior wall of the middle ear
- Innervated by the nerve to stapedius - a branch of CN VII (facial nerve), arising from the mastoid/vertical segment just below the second genu
Reflex Arc - The Complete Pathway
Stimulus: Loud sound (~70-100 dB HL in a normal ear)
TWO arcs exist depending on which ear is stimulated:
A. Ipsilateral Arc (stimulus and recording in the SAME ear)
Loud sound → Cochlea (outer/inner hair cells)
↓
CN VIII (Cochlear nerve / Acoustic nerve)
↓
Ipsilateral Ventral Cochlear Nucleus (VCN)
↓
Trapezoid body
↓
Ipsilateral Facial Motor Nucleus (OR Medial Superior Olive → Facial nucleus)
↓
Ipsilateral CN VII (Facial nerve) → Nerve to stapedius branch
↓
Ipsilateral Stapedius muscle contracts
↓
Stiffens ipsilateral ossicular chain → Sound damped
B. Contralateral Arc (stimulus in one ear, recording/contraction in the OTHER ear)
Loud sound in RIGHT ear → Cochlea
↓
Right CN VIII → Right Ventral Cochlear Nucleus
↓
Crosses midline via Trapezoid body
↓
LEFT Medial Superior Olive
↓
LEFT Facial Motor Nucleus
↓
LEFT CN VII → Left Nerve to stapedius
↓
LEFT Stapedius muscle contracts
"The contralateral acoustic reflex arc includes the acoustic nerve and ventral cochlear nucleus, the medial superior olive, the contralateral motor nucleus of CN VII, and the contralateral stapedius muscle." - Cummings Otolaryngology
"The sensory pathway is through the cochlear nerve and nucleus to the reticular formation adjacent to the facial motor nucleus and from there to the stapedial motor neurons, which run in the facial nerve." - Kandel's Principles of Neural Science, 6th Ed.
Key point: A single loud sound in one ear triggers bilateral stapedius contraction - both ipsilateral AND contralateral.
Normal Threshold
- Reflex occurs at 70-100 dB HL in normal hearing ears
- In cochlear hearing loss with recruitment (loudness intolerance): reflex may occur at levels as low as 60 dB SL (occurs at lower sensation levels because of abnormal loudness growth)
Clinical Testing: Tympanometry / Impedance Audiometry
The stapedius contraction changes the stiffness (compliance) of the tympanic membrane, which is detected by the probe in the ear canal. The test is objective - no patient response needed.
Two main measures:
| Test | What It Measures | Normal | Abnormal |
|---|---|---|---|
| Acoustic Reflex Threshold (ART) | Softest sound level that triggers contraction | 70-100 dB HL | Elevated or absent |
| Acoustic Reflex Decay | Can stapedius sustain contraction for 10 sec? (signal at 10 dB above ART for 10 sec) | Amplitude maintained | Drops to ≤50% in <5 sec = ABNORMAL → suggests retrocochlear disease |
Localizing Value: Acoustic Reflex Patterns
This diagram shows the different patterns of reflex presence (filled square) or absence (open square) with different lesion sites:
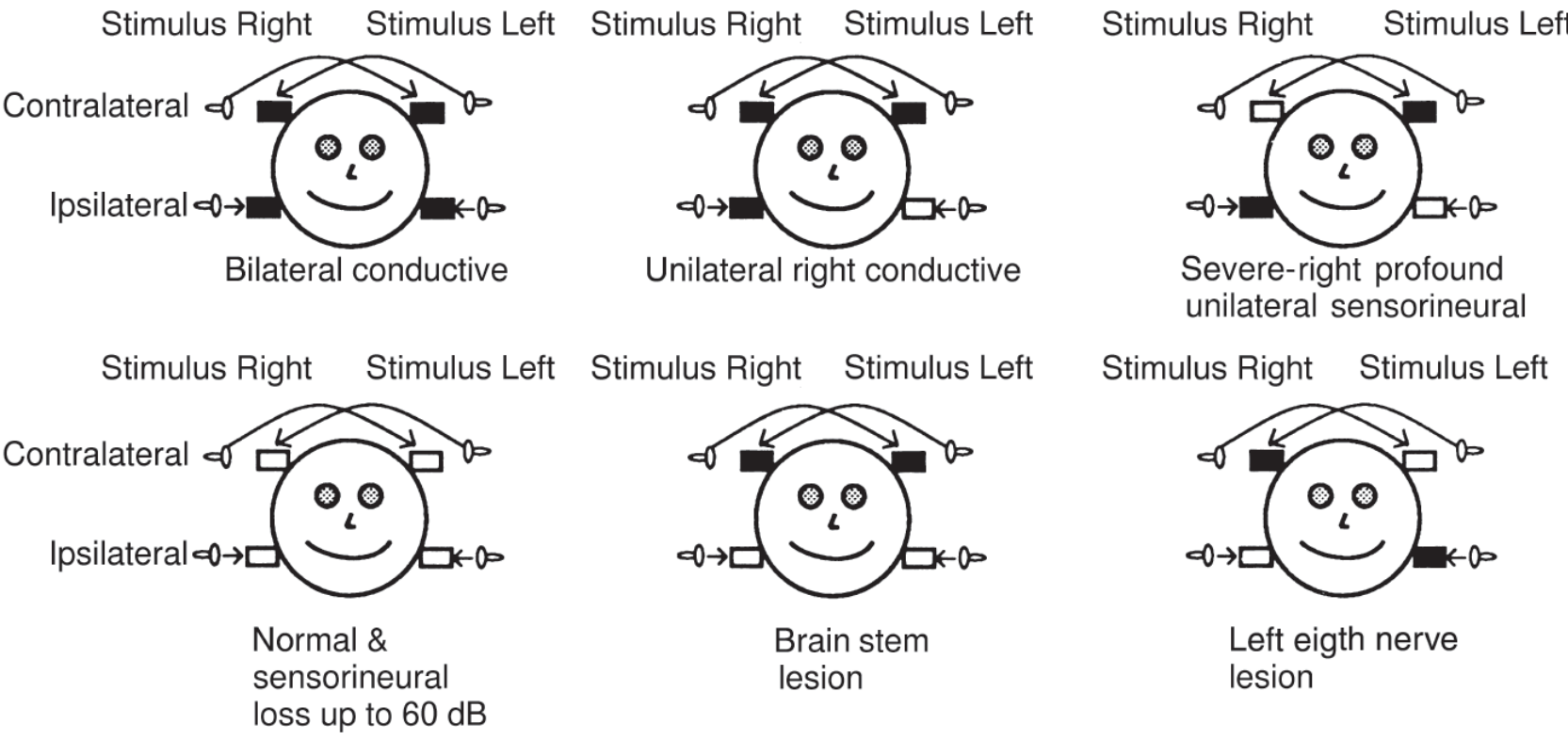
Acoustic reflex patterns: filled = present, open = absent. Each pattern helps localize the site of lesion - KJ Lee's Essential Otolaryngology
Pattern Analysis Table
| Condition | Ipsilateral reflex | Contralateral reflex | Reason |
|---|---|---|---|
| Normal / Cochlear SNHL ≤60 dB | Present | Present | Both arcs intact |
| Cochlear SNHL with recruitment | Present at low SL | Present | Loudness recruitment activates reflex earlier |
| Conductive hearing loss (recording ear) | Absent | Absent | Middle ear stiffness prevents compliance change from being detected regardless of stimulus side |
| Conductive loss (stimulated ear) | Absent | Absent | Sound doesn't reach cochlea at sufficient intensity |
| Severe/Profound SNHL (>65 dB) - stimulated ear | Absent | Absent | Not enough cochlear output to drive reflex |
| Retrocochlear (CN VIII lesion e.g. acoustic neuroma) | Absent when stimulated | Absent when stimulated | Afferent limb damaged; efferent (contralateral) reflexes intact when other ear stimulated |
| Retrocochlear - Acoustic reflex decay | May be present but DECAYS | - | CN VIII fatigue |
| Brainstem lesion (crosses midline pathways) | Ipsilateral intact | Contralateral ABSENT | Crossed brainstem pathway interrupted; uncrossed intact |
| CN VII lesion (proximal to nerve to stapedius) | Absent ipsilateral | Absent | Efferent limb damaged - stapedius cannot contract |
| CN VII lesion (distal to nerve to stapedius) | Present | Present | Branch to stapedius intact, facial palsy spares the reflex |
Localizing CN VII Lesions with Stapedial Reflex
This is the most clinically used application:
GSPN Nerve to Chorda Stylomastoid
branch Stapedius Tympani Foramen
| | | |
──────────────────────────────────────────────────► Facial nerve (distal)
↑
If lesion HERE (proximal to nerve to stapedius):
→ Stapedial reflex ABSENT
→ Hyperacusis present
↑
If lesion HERE (distal to nerve to stapedius):
→ Stapedial reflex PRESENT (stapedius branch intact)
→ No hyperacusis
"The stapedius reflex provides valuable clinical information regarding the level of a facial nerve lesion. If the lesion is proximal, an absent stapedius reflex may be expected. If the lesion is distal to the stapedius branch, an intact reflex may be expected. Stapedius reflex measurement should be included ROUTINELY in the evaluation of patients with facial paralysis." - Cummings Otolaryngology
In Bell's Palsy: Prognostic Value
The stapedial reflex has prognostic importance in Bell's palsy:
- Reflex PRESENT = the lesion is incomplete / distal → better prognosis for recovery
- Reflex ABSENT = lesion at or proximal to the nerve to stapedius → more severe, may indicate degeneration → poorer prognosis, higher chance of incomplete recovery
Quick Summary
STAPEDIAL REFLEX ARC:
Loud sound → CN VIII → VCN → (cross via trapezoid body) →
Facial motor nucleus → CN VII → Nerve to stapedius → Stapedius contracts
→ Ossicular chain stiffens → Sound damped → Cochlea protected
BILATERAL: One loud sound triggers BOTH stapedii simultaneously
CLINICAL USE:
1. Differentiate cochlear vs. retrocochlear hearing loss
2. Detect brainstem lesions (contralateral absent, ipsilateral present)
3. Localize CN VII lesions (absent = proximal; present = distal to stapedius branch)
4. Prognosis in Bell's palsy
Sources: KJ Lee's Essential Otolaryngology; Cummings Otolaryngology; Kandel's Principles of Neural Science 6th Ed.; Localization in Clinical Neurology 8e
This is a shared conversation. Sign in to Orris to start your own chat.