Otomycosis treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
otomycosis treatment antifungal
Reading File
Reading File
Reading File
Reading Article
PMID: 41373129
Reading File
Reading File
Loading Image
I have comprehensive data from multiple authoritative sources. Let me now compile the full answer.
Otomycosis Treatment
Otomycosis (fungal otitis externa) accounts for approximately 9-10% of all otitis externa cases. Aspergillus species (80-90%, especially A. niger) and Candida (10-20%) are the dominant pathogens.
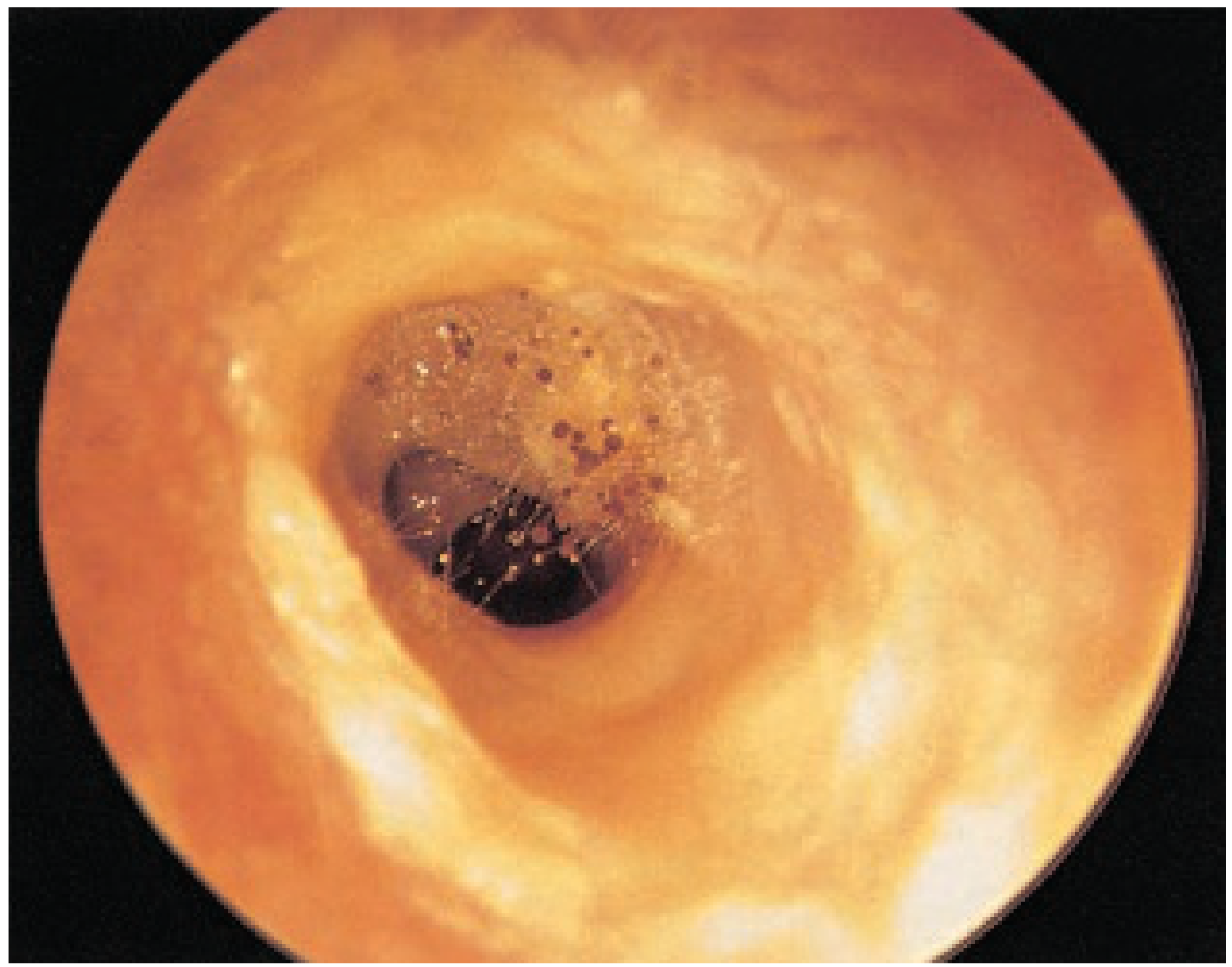
Otomycosis with Aspergillus niger (Scott-Brown's Otorhinolaryngology)
1. Core Treatment Principles
Treatment rests on three pillars:
- Elimination of predisposing factors - stop prolonged topical antibiotics, address hearing aid use, treat immunosuppression
- Thorough aural toilet - meticulous suction debridement and removal of fungal debris is the single most important step
- Antifungal agents - topical first-line in most cases
2. Topical Antifungal Agents
Specific Antifungals (first-line)
| Agent | Notes |
|---|---|
| Clotrimazole 1% (cream or solution) | Most widely used azole; efficacy 95-100%; single application after debridement gives ~96% symptom-free rate; low recurrence (<3%); broad-spectrum coverage with MIC <0.1 µg/mL for >94% of isolates |
| Miconazole 2% | Effective topically; adding acidifying drops (acetic acid 3% + alcohol 97%) does not significantly improve outcome |
| Ketoconazole | Better efficacy and lower recurrence vs cresylate and aluminum acetate |
| Econazole | Used topically; included in otomycosis protocols |
| Nystatin (polyene) | Broadest in-vitro spectrum; available as suspension, cream, or powder (no dedicated otic preparation); damages fungal membrane permeability |
| Ciclopirox olamine 0.77% | Equal efficacy to boric acid; better tolerated; no ototoxicity in animal models |
| Terbinafine 1% | In-vitro activity comparable to clotrimazole, miconazole, nystatin |
| Tolnaftate | Effective in vitro against all 59 fungal species tested (MIC <1 µg/mL) |
Non-Specific / Acidifying Agents
- Aluminum acetate (Burow solution) - >80% effective in mild cases
- Acetic acid + propylene glycol + hydrocortisone 1% (VoSol HC) - acidifying; good for mild disease
- Boric acid solution - comparable efficacy to ciclopirox but causes significantly more discomfort
- Acetic acid (Domeboro Otic)
Note: Acidifying agents work well for mild uncomplicated cases, especially combined with debridement. They do not add benefit when combined with miconazole.
3. Topical Antiseptics (Second-line / Refractory)
| Agent | Notes |
|---|---|
| Gentian violet | Useful in refractory cases; avoid with perforated tympanic membrane (ototoxic in animal studies) |
| Silver nitrate gel 1% | Single application cured 92% of ears with refractory otomycosis within 1 week |
| Cresylate 25% | >80% effective; caution - shown ototoxic in some models |
| Mercurochrome | Found more effective than clotrimazole or miconazole in one trial |
4. Ototoxicity Considerations
This is clinically important, especially with tympanic membrane perforation or mastoid cavities:
- Safe (no ototoxicity): Clotrimazole, miconazole, tolnaftate, nystatin, ciclopirox
- Ototoxic - AVOID with perforation: Gentian violet, cresylate, acetic acid/propylene glycol preparations
- Conflicting data: Terbinafine
- Cummings Otolaryngology, p. 3825
5. Flumethasone + Clioquinol Drops
A combined antifungal-steroid preparation (flumethasone with clioquinol) is commonly used to expedite recovery alongside aural toilet - cited as a standard topical option in Scott-Brown's guidelines.
6. Resistant / Refractory Otomycosis
- Exclude fungal infection at remote sites ("foot and ear" dermatophytid/id reaction)
- If id reaction confirmed: immunotherapy with TOE (Trichophyton, Oidiomycetes, Epidermophyton) extracts and dust mite antigen
- Silver nitrate gel 1% is highly effective for refractory cases
7. Invasive / Malignant Fungal Otitis Externa
This is a medical emergency, particularly in diabetics and immunocompromised patients (84% of cases have immunocompromise; 44% have cranial nerve palsy):
- Amphotericin B - traditional systemic antifungal of choice
- Voriconazole - increasingly preferred due to tolerability and efficacy, especially for Aspergillus
- Aggressive systemic therapy is mandatory; skull base osteomyelitis carries high mortality
8. Latest Evidence (2026 Systematic Review & Meta-analysis)
A 2026 systematic review and meta-analysis (Hussain et al., Otology & Neurotology; 15 RCTs, 2,309 patients) found:
- Overall eradication rate across all topical therapies: 73.6%
- Eradication range: 29-98% depending on agent and protocol
- Clotrimazole is the most commonly studied and used agent
- Adverse effects were generally mild (otalgia, pruritus, burning)
- No consensus yet on a single superior agent; future unified-protocol trials are needed
Summary Algorithm
Otomycosis confirmed
↓
Aural toilet + debridement (mandatory)
↓
Topical antifungal (first-line): Clotrimazole 1% cream/solution
↓
No response?
├── Check: tympanic membrane intact? → avoid ototoxic agents
├── Switch or add: ketoconazole, miconazole, nystatin
├── Refractory: silver nitrate 1% gel (single application)
└── Immunocompromised + invasive signs?
→ Systemic voriconazole or amphotericin B
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1, p. 256
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2, p. 1000
- Cummings Otolaryngology Head and Neck Surgery, pp. 3792-3825
- Hussain S et al. Management of Otomycosis: A Systematic Review and Meta-analysis. Otol Neurotol, 2026 (PMID: 41373129)
This is a shared conversation. Sign in to Orris to start your own chat.