Pneumothorax Detail explanations
Reading File
Finding Sources
Searching PubMed
pneumothorax management treatment
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to deliver a thorough, well-structured explanation of pneumothorax. Here it is:
Pneumothorax - Detailed Explanation
Definition
Pneumothorax is the presence of air in the pleural space - the potential space between the visceral and parietal pleura. Under normal conditions, this space has a slightly negative (subatmospheric) intrapleural pressure that keeps the lungs expanded against the chest wall. When air enters, the lung on the affected side collapses.
- Murray & Nadel's Textbook of Respiratory Medicine, Chapter 110
- Rosen's Emergency Medicine, Chapter 63
Classification
1. Primary Spontaneous Pneumothorax (PSP)
Occurs in patients with no clinically apparent underlying lung disease. Classically affects tall, thin young men (peak age 15-34 years). The male-to-female ratio is approximately 3:1.
Pathogenesis: PSP is caused by rupture of subpleural blebs or bullae - small thin-walled air pockets just beneath the visceral pleura. Despite having "normal-appearing" lungs on CXR, these patients often have microscopic emphysema-like changes, distal airway inflammation, and "pleural porosity" detectable on CT or biopsy. Smoking is a major risk factor and significantly increases recurrence risk.
Risk factors:
- Tall, thin body habitus (low weight-to-height ratio)
- Cigarette smoking
- Marfan syndrome, mitral valve prolapse
- Changes in ambient atmospheric pressure
- Genetic predisposition (rare)
2. Secondary Spontaneous Pneumothorax (SSP)
Occurs in patients with pre-existing lung disease. By definition, also 3x more common in men. SSP carries higher morbidity and mortality than PSP because of reduced pulmonary reserve. Even a small SSP can cause severe dyspnea - symptoms rarely resolve spontaneously.
Causes (Box 63.1 - Rosen's):
| Category | Examples |
|---|---|
| Airway disease | COPD (most common in developed world), asthma, cystic fibrosis |
| Infections | Tuberculosis (most common in developing world), necrotizing pneumonia, lung abscess, Pneumocystis jirovecii pneumonia (HIV patients) |
| Interstitial lung disease | Sarcoidosis, idiopathic pulmonary fibrosis, lymphangioleiomyomatosis, tuberous sclerosis |
| Neoplasms | Primary lung cancer, pulmonary/pleural metastases |
| Connective tissue diseases | Marfan syndrome, scleroderma, rheumatoid arthritis |
| Miscellaneous | Pulmonary infarction, endometriosis (catamenial PTX) |
3. Tension Pneumothorax
A life-threatening emergency where the pleural defect acts as a one-way valve - air enters the pleural space during inspiration but cannot escape during expiration. This leads to progressive accumulation of intrapleural air with rising intrathoracic pressure.
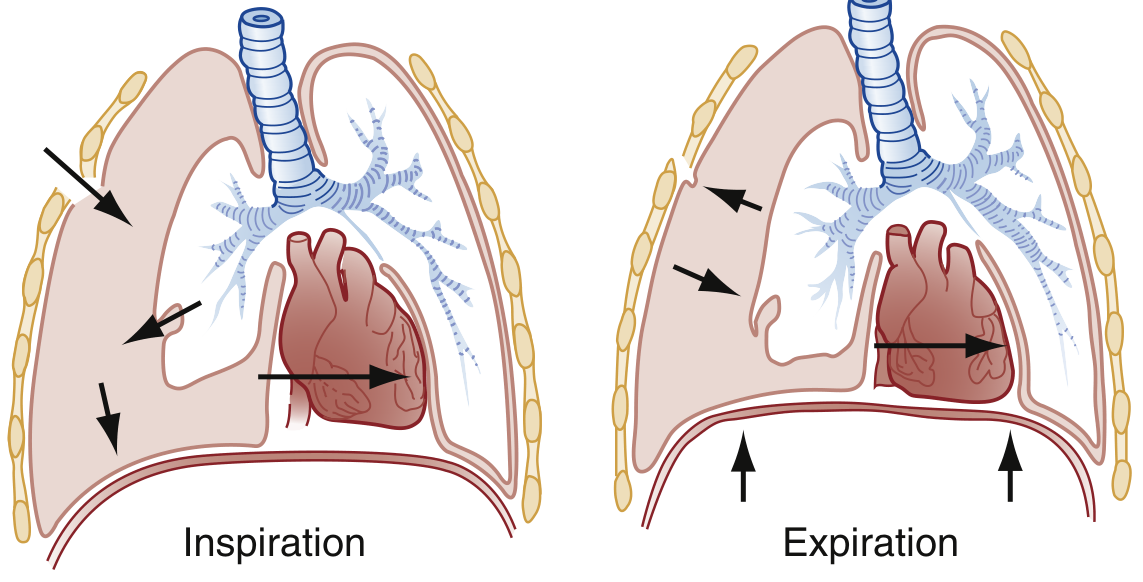
Fig. 63.1 - Tension pneumothorax: progressive mediastinal shift from one-way valve mechanism during inspiration vs. expiration (Rosen's Emergency Medicine)
Consequences:
- Compression of mediastinal venous structures
- Reduced venous return to the heart
- Contralateral lung compression
- Worsening hypoxemia → cardiovascular collapse → death if untreated
4. Traumatic Pneumothorax
Results from penetrating or blunt chest trauma (e.g., rib fractures lacerating the visceral pleura, stab wounds, gunshot wounds). Hemopneumothorax (blood + air) is common in trauma.
5. Iatrogenic Pneumothorax
Complicates medical procedures:
- Central venous line or pacemaker insertion
- Thoracentesis
- Transbronchial or transthoracic needle biopsy
- Barotrauma from mechanical ventilation (alveolar overdistension)
6. Catamenial Pneumothorax
Rare form occurring in women of reproductive age, typically within 24-72 hours of the onset of menstruation. Associated with intrathoracic endometriosis. Right-sided predominance.
Pathophysiology
Normally, the visceral and parietal pleura are held in apposition by negative intrapleural pressure. When the alveolar-pleural barrier is disrupted:
- Air flows into the pleural space until the defect seals or alveolar and intrapleural pressures equalize
- The ipsilateral lung collapses (partial or complete)
- Vital capacity, FRC, and total lung capacity fall (restrictive pattern)
- Poorly ventilated atelectatic lung creates a shunt, potentially causing hypoxemia (though hypoxic vasoconstriction in the collapsed lung partially compensates)
- In tension PTX: intrapleural pressure rises above atmospheric, causing mediastinal shift, vena caval compression, and reduced cardiac output
- Rosen's Emergency Medicine, p. 983
Clinical Features
Symptoms
| Feature | PSP | SSP | Tension PTX |
|---|---|---|---|
| Onset | Sudden | Sudden | Sudden, rapidly worsening |
| Chest pain | Ipsilateral, pleuritic (sharp) | Similar | Severe |
| Dyspnea | Mild to moderate | Severe (even with small PTX) | Severe, worsening rapidly |
| Time to presentation | Hours to days | Hours | Minutes |
In PSP, symptoms may resolve spontaneously within 24-72 hours even with the pneumothorax still present. In SSP, spontaneous resolution is rare.
Physical Examination
- Sinus tachycardia - earliest finding
- Decreased/absent breath sounds on affected side
- Hyper-resonance to percussion on affected side
- Reduced chest wall movement on affected side
- Absent tactile fremitus
- Unilateral hemithorax expansion
In Tension PTX (late signs):
- Tachycardia → hypotension (late) → cardiovascular collapse
- Jugular venous distension (may be subtle)
- Tracheal deviation away from affected side (late, not always present)
- Severe respiratory distress, diaphoresis, cyanosis
- Electromechanical dissociation / PEA cardiac arrest
Tracheal deviation is a classic teaching sign but is unreliable - its absence does NOT rule out tension pneumothorax. Treatment must not be delayed waiting for tracheal deviation.
- Rosen's Emergency Medicine, p. 983; Washington Manual of Medical Therapeutics
Diagnosis
Chest Radiograph (CXR) - Primary imaging
Classic finding: a thin visceral pleural line running parallel to the chest wall, separated from the chest wall by a radiolucent band devoid of lung markings.

Fig. 63.2 - CXR showing classic pneumothorax appearance (Rosen's Emergency Medicine)
Sizing by CXR:
- BTS criteria (intrapleural distance at hilum level): Small <1 cm | Moderate 1-2 cm | Large >2 cm
- ACCP criteria (apex to cupola distance): Small <3 cm | Large ≥3 cm
Special situations:
- Supine patient (ICU): look for the "deep sulcus sign" - unusually deep lateral costophrenic angle and excessive lucency over upper abdomen (air migrates anteriorly)
- COPD: reduced lung markings mimic PTX; large bullae can resemble PTX (bullae tend to have concave appearance; PTX line is parallel to chest wall)
- Tension PTX: complete ipsilateral lung collapse, contralateral mediastinal shift, flattened/inverted ipsilateral hemidiaphragm
CT Thorax
More sensitive than CXR - detects occult pneumothorax. Indications:
- Nondiagnostic CXR in symptomatic patient
- Underlying COPD/emphysema (distinguish bullae from PTX)
- Assess for underlying blebs/bullae to guide surgical planning
- Traumatic chest injury
Ultrasound (POCUS)
Rapid bedside tool, especially in trauma and critical care.
- Lung sliding (shimmering movement at pleural line on B-mode): presence excludes PTX at that location
- Sea-shore sign (M-mode): normal finding - linear chest wall pattern interrupted by granular "sandy beach" pattern below pleura
- Bar code / Stratosphere sign (M-mode): loss of lung sliding - horizontal lines throughout screen; suggests PTX (or apnea, pleural adhesions)
- B-lines: their presence excludes PTX at that location
- Lung point: highly specific for PTX - the edge where sliding transitions to absent sliding; represents margin of the PTX
Ultrasound can exclude PTX at an imaged location with high sensitivity but diagnosing PTX requires integration of multiple findings. Sensitivity is operator-dependent.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 585
ECG (supplementary)
- Diminished anterior QRS amplitude
- Anterior axis shift
- Electromechanical dissociation in severe tension PTX
Management
Tension Pneumothorax - IMMEDIATE EMERGENCY
Tension PTX is a clinical diagnosis. Do NOT wait for imaging.
- Needle decompression (emergency first step): 14-16G needle, 2nd intercostal space (ICS), midclavicular line (or 4th/5th ICS, anterior axillary line)
- A recent 2025 meta-analysis (PMID: 40383767) examined optimal needle length and site for tension PTX decompression, noting that standard needle length may be insufficient in obese patients
- Followed immediately by tube thoracostomy (definitive management): chest drain placed at 5th ICS, anterior axillary line
Simple/Spontaneous Pneumothorax Management
Step 1 - Assess clinical stability and size:
| Situation | Management |
|---|---|
| Hemodynamically unstable | Immediate intervention regardless of size |
| Small PSP (<1-2 cm), stable, no dyspnea | Observation with supplemental O₂ (accelerates air reabsorption 4x), repeat CXR in 4-6 hours; discharge if stable |
| Moderate-large PSP, symptomatic | Aspiration or chest drain |
| Any SSP | Chest drain (even small SSP has high risk of progression) |
| Mechanically ventilated patient with any PTX | Chest drain immediately (any simple PTX can rapidly become tension PTX on positive pressure ventilation) |
Supplemental O₂: High-flow O₂ increases the gradient for nitrogen reabsorption from the pleural space, accelerating resolution 3-4x faster than room air breathing.
Aspiration: Simple needle aspiration can manage first-episode PSP. Less traumatic than chest drain. If >2.5 L aspirated without success, proceed to chest drain.
Chest tube (tube thoracostomy):
- Small-bore tube (7-14 Fr) - adequate for uncomplicated PSP
- Medium (20-28 Fr) - SSP
- Large (28-40 Fr) - trauma, mechanical ventilation, hemopneumothorax
- Connected to water-seal drainage system with 20 cmH₂O suction for persistent air leaks
- Reduce to water seal only after air leak resolves
- Remove tube after resolution confirmed on CXR (after 4-hour clamp test)
Persistent air leak: Defined as air leak >5-7 days. Warrants surgical evaluation (VATS).
Prevention of Recurrence
After a first PSP, recurrence risk is 30-50%. After second episode, risk rises to ~80%. Options to prevent recurrence:
- Video-assisted thoracoscopic surgery (VATS): Bullectomy + pleural abrasion or pleurectomy. Most effective (recurrence <5%). Indicated after second ipsilateral PTX, first contralateral PTX, persistent air leak, bilateral simultaneous PTX, high-risk occupation (pilots, divers)
- Chemical pleurodesis: Talc, doxycycline, or tetracycline via chest tube. Less invasive but lower success rate (~75%)
- Blood patch pleurodesis: Autologous blood instilled into pleural space
Return to Activity
-
Return to play after sports-related PTX: generally 3-4 weeks (after confirmed resolution)
-
Aviation/diving: requires formal clearance and may require definitive pleurodesis
-
Textbook of Family Medicine 9e; Roberts & Hedges' Clinical Procedures in Emergency Medicine
Recurrence and Complications
| Complication | Details |
|---|---|
| Recurrence | 30-50% after first PSP; 80% after second; higher in SSP |
| Re-expansion pulmonary edema | Can occur after rapid re-expansion of a long-standing large PTX |
| Hemopneumothorax | Simultaneous blood + air; occurs in ~5% of PTX from torn adhesion |
| Respiratory failure | Especially in SSP with poor pulmonary reserve |
| Death | Rare in PSP; not uncommon in SSP |
Special Populations
HIV/AIDS patients: P. jirovecii pneumonia (PCP) is a major cause of SSP. PTX in HIV patients with PCP carries very high mortality (>50%).
Mechanically ventilated patients: Any PTX must be drained urgently - positive pressure ventilation continuously forces air into the pleural space through the defect. Even a small PTX can become a lethal tension PTX within minutes.
Cystic fibrosis: PTX is a serious complication. Management is complicated by the need to preserve lung tissue for possible future transplantation (limits aggressive pleurodesis options).
Pregnant women: Tension PTX in pregnancy also endangers the fetus via maternal cardiovascular compromise. Immediate decompression is mandatory.
Summary Table
| Type | Cause | Patient | Severity | Management |
|---|---|---|---|---|
| Primary spontaneous | Bleb rupture | Young, tall, thin male | Mild-moderate | Observation/aspiration/small drain |
| Secondary spontaneous | Underlying lung disease | Older, smoker, COPD/ILD etc. | Severe (poor reserve) | Chest drain ± VATS |
| Tension | One-way valve mechanism | Any (trauma, ventilated) | Life-threatening | Immediate needle + chest drain |
| Traumatic | Chest trauma | Trauma patient | Variable | Chest drain |
| Iatrogenic | Procedure complication | Post-procedure | Variable | Observation or drain based on size |
| Catamenial | Endometriosis | Reproductive-age women | Recurrent | Hormonal ± surgery |
Sources:
- Murray & Nadel's Textbook of Respiratory Medicine, Chapter 110 (PNEUMOTHORAX)
- Rosen's Emergency Medicine: Concepts and Clinical Practice, Chapter 63
- Washington Manual of Medical Therapeutics
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
- Current Surgical Therapy, 14th Edition
- Textbook of Family Medicine, 9th Edition
Recent evidence note: A 2025 meta-analysis (PMID: 40383767) found that standard needle lengths used for tension PTX decompression may fail in up to 50% of patients due to chest wall thickness, suggesting the anterior axillary line (4th/5th ICS) may be more reliable than the traditional 2nd ICS midclavicular line approach, prompting updates to ATLS/ETC guidelines.
This is a shared conversation. Sign in to Orris to start your own chat.