Non Hodgkin's lymphoma
Reading File
Finding Sources
Finding Sources
Reading File
Searching Images
Non-Hodgkin lymphoma classification histology
Reading File
Loading Image
I now have comprehensive content from Goldman-Cecil Medicine. Let me synthesize a thorough response.
Non-Hodgkin Lymphoma (NHL)
Definition
Non-Hodgkin lymphomas (NHL) are a heterogeneous group of solid tumors of the immune system arising from lymphoid cells (B cells, T cells, or NK cells) at various stages of differentiation. They differ from Hodgkin lymphoma principally by the absence of Reed-Sternberg cells and by their greater biologic and clinical diversity.
Epidemiology
- ~80,000 new cases/year in the United States; ~20,000 deaths/year
- Account for ~5% of all new cancers and ~3% of cancer deaths
- Lifetime risk: 2.4% (men), 1.9% (women)
- Incidence increases sharply with age; higher in Whites than other ethnic groups
- Highest rates in the US, Europe, and Australia; lower in Asia
- Incidence rose 3–4%/year from 1950 to the early 2000s, now plateaued; mortality is declining
Pathobiology & Risk Factors
Genetic Factors
- Familial clustering with modestly elevated risk in first-degree relatives
- Polymorphisms in immunity-related genes (TNF, IL-10, lymphotoxin-α, chemokines)
Immune System Abnormalities
| Condition | Mechanism |
|---|---|
| X-linked lymphoproliferative disorder | EBV dysregulation via SH2D1A mutations |
| Post-transplant lymphoproliferative disorder | Immunosuppression → EBV-driven B-cell proliferation (up to 20% of organ transplant recipients) |
| HIV/AIDS | Profound immunodeficiency |
| Rheumatoid arthritis | ~2-fold increased risk |
| Sjögren syndrome | ~30–40-fold increased risk for marginal zone lymphoma |
| Hashimoto thyroiditis | Increased thyroid lymphoma risk |
| Celiac disease | Associated with enteropathy-type T-cell lymphoma |
Infectious Agents
| Agent | Associated Lymphoma |
|---|---|
| Epstein-Barr virus (EBV) | >95% of endemic Burkitt; post-transplant lymphoproliferative disorders; HIV-associated lymphomas; plasmablastic lymphoma; extranodal NK/T-cell lymphoma |
| HTLV-1 | Virtually 100% of adult T-cell leukemia/lymphoma |
| HHV-8 | Primary effusion lymphoma (immunocompromised) |
| Hepatitis C virus | Lymphoplasmacytic lymphoma, nodal & splenic marginal zone lymphoma |
| H. pylori | Gastric MALT lymphoma |
| Borrelia burgdorferi | Marginal zone B-cell lymphoma of skin |
Environmental/Occupational Exposures
- Phenoxy herbicides (e.g., 2,4-D/Agent Orange), ionizing radiation, organic solvents
- High-fat diet, heavy smoking (follicular lymphoma)
- Prior Hodgkin lymphoma treatment (~20-fold increased risk)
- Anti-TNF agents (possible association with hepatosplenic T-cell lymphoma)
Classification (WHO)
NHL is broadly divided into:
B-Cell Neoplasms (majority, ~85–90%)
| Type | Key Features |
|---|---|
| Diffuse large B-cell lymphoma (DLBCL) | Most common (~30%); aggressive; potentially curable with R-CHOP |
| Follicular lymphoma | 2nd most common; indolent; CD10+, BCL2+, t(14;18) |
| Marginal zone lymphoma (MALT, nodal, splenic) | Indolent; antigen-driven |
| Mantle cell lymphoma | Aggressive; cyclin D1+, t(11;14) |
| Burkitt lymphoma | Highly aggressive; MYC translocation; "starry sky" pattern; EBV-associated (endemic) |
| Lymphoplasmacytic lymphoma | Produces IgM (Waldenström macroglobulinemia); HCV-associated |
| Primary effusion lymphoma | HHV-8+; immunocompromised patients |
T-Cell & NK-Cell Neoplasms (~10–15%)
| Type | Key Features |
|---|---|
| Peripheral T-cell lymphoma, NOS | Aggressive; poor prognosis |
| Anaplastic large cell lymphoma (ALCL) | CD30+; ALK+ (better prognosis) or ALK− |
| Adult T-cell leukemia/lymphoma | HTLV-1-associated; aggressive |
| Extranodal NK/T-cell lymphoma | EBV-associated; nasal type |
| Enteropathy-associated T-cell lymphoma | Celiac disease-associated |
| Hepatosplenic T-cell lymphoma | γδ T-cells; often in immunocompromised young males on anti-TNF therapy |
| Mycosis fungoides / Sézary syndrome | Cutaneous T-cell lymphoma; CD4+ |
Clinical Presentation
Most common: painless lymphadenopathy (cervical, axillary, inguinal)
B symptoms (present in ~30%):
- Fever >38°C, drenching night sweats, weight loss >10% body weight
Other features:
- Splenomegaly, hepatomegaly
- Extranodal involvement (GI tract, skin, CNS, bone marrow, lung) — more common in NHL than Hodgkin
- Cytopenias (from marrow infiltration or autoimmune mechanisms)
- Pruritus (less common than in Hodgkin lymphoma; occurs in ~10%)
- Waldeyer ring involvement (tonsils, nasopharynx)
Diagnosis
Each new NHL patient requires a systematic evaluation:
- Tissue biopsy — excisional lymph node biopsy preferred; core needle biopsy acceptable; FNA alone is insufficient
- Histology + immunophenotyping (IHC panel: CD20, CD3, CD5, CD10, CD30, BCL2, BCL6, Ki-67, etc.)
- Cytogenetics/FISH — key translocations: t(14;18) follicular, t(11;14) mantle cell, MYC/BCL2/BCL6 in DLBCL
- Molecular studies — gene rearrangements, mutational profiling
Staging (Lugano/Ann Arbor):
| Stage | Description |
|---|---|
| I | Single lymph node region or single extranodal site |
| II | ≥2 regions, same side of diaphragm |
| III | Both sides of diaphragm |
| IV | Diffuse/disseminated involvement (bone marrow, liver, lung) |
A = no B symptoms; B = B symptoms present
Workup:
- CBC, CMP, LDH, β2-microglobulin, uric acid
- CT chest/abdomen/pelvis (PET-CT preferred for FDG-avid lymphomas)
- Bone marrow biopsy
- HIV, HBV, HCV serologies
- ECHO (if anthracycline-based chemo planned)
- Lumbar puncture (if CNS involvement suspected or high-risk NHL)
Prognostic Score — International Prognostic Index (IPI) for DLBCL:
Each scores 1 point: age >60, LDH elevated, ECOG performance status ≥2, Ann Arbor stage III/IV, >1 extranodal site
- Low (0–1): ~73% 5-year survival
- High (4–5): ~26% 5-year survival
Treatment
Indolent NHL (e.g., Follicular Lymphoma)
- Asymptomatic, low tumor burden: Watch and wait (observation)
- Symptomatic/progressive: R-CVP (rituximab + cyclophosphamide, vincristine, prednisone) or R-CHOP; bendamustine + rituximab
- Maintenance rituximab prolongs remission
- Targeted therapy: Idelalisib (PI3Kδ), lenalidomide + rituximab (R²)
- Relapsed/refractory: CAR-T cell therapy, PI3K inhibitors, EZH2 inhibitors (tazemetostat for EZH2-mutant)
- Gastric MALT: H. pylori eradication first-line (antibiotic triple therapy)
Aggressive NHL (e.g., DLBCL)
- Standard: R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone) ×6 cycles
- CNS prophylaxis: High-dose methotrexate for high-risk patients
- Relapsed/refractory: Salvage chemo (R-ICE, R-DHAP) → autologous stem cell transplant (ASCT) if chemosensitive
- CAR-T therapy: Axicabtagene ciloleucel (axi-cel), tisagenlecleucel — approved for relapsed/refractory DLBCL after ≥2 prior lines; now also approved in second-line setting
- Bispecific antibodies: Epcoritamab, glofitamab (CD20×CD3)
Highly Aggressive NHL (Burkitt Lymphoma)
- Intensive regimens: hyper-CVAD, CODOX-M/IVAC, DA-EPOCH-R
- CNS prophylaxis essential (intrathecal chemotherapy)
- High cure rates with appropriate intensive treatment
Mantle Cell Lymphoma
- Younger, fit patients: Rituximab-based induction + ASCT
- R-CHOP or BR (bendamustine + rituximab); ibrutinib (BTK inhibitor)
- Relapsed: Ibrutinib, acalabrutinib, venetoclax
T-Cell Lymphomas
- Generally poorer prognosis than B-cell counterparts
- CHOP-based regimens; brentuximab vedotin (for CD30+ ALCL)
- Pralatrexate, romidepsin (histone deacetylase inhibitor) for relapsed PTCL
- Allogeneic SCT for eligible patients
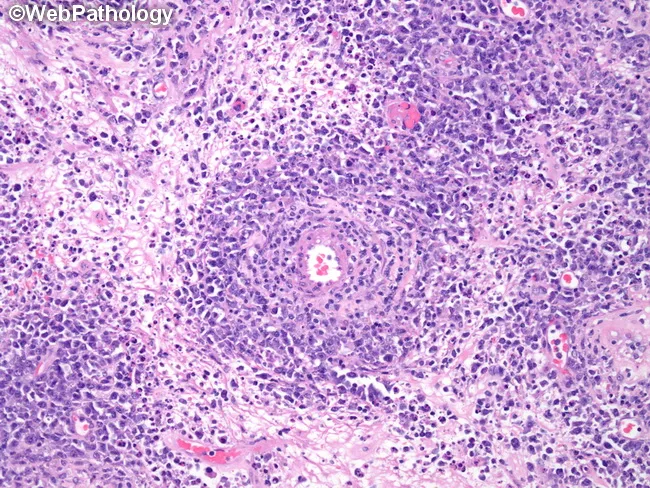
Histopathology Image
DLBCL — diffuse large B-cell lymphoma (testicular, extranodal NHL), H&E stain showing sheets of large atypical lymphoid cells with vesicular nuclei, prominent nucleoli, and perivascular cuffing:
Prognosis
| Subtype | 5-Year Survival |
|---|---|
| Follicular lymphoma (grade 1–2) | ~75–85% (indolent, rarely cured) |
| DLBCL (with R-CHOP) | ~60–70% overall; >80% in low-risk |
| Burkitt lymphoma (intensive chemo) | ~70–90% |
| Mantle cell lymphoma | ~50–70% (variable) |
| Peripheral T-cell lymphoma, NOS | ~30–40% |
| Adult T-cell leukemia/lymphoma | Poor (<1 year median) |
Overall, the 5-year survival for NHL has improved significantly over the past four decades. Beneficial treatment exists for essentially every NHL subtype, and many aggressive lymphomas are potentially curable.
— Goldman-Cecil Medicine, Chapter 171 (Vose & Armitage)
This is a shared conversation. Sign in to Orris to start your own chat.