In detail about FESS
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content to deliver a detailed, well-structured answer on FESS. Let me compile everything.
Functional Endoscopic Sinus Surgery (FESS)
1. Definition & Primary Objective
Functional Endoscopic Sinus Surgery (FESS) is a minimally invasive surgical approach performed entirely through the nostrils using a rigid endoscope. Its primary objective is to restore paranasal sinus function by reestablishing the physiologic pattern of ventilation and mucociliary clearance. The cilia of the maxillary and frontal sinuses transport mucus specifically toward the natural ostia — FESS is designed to alleviate osteomeatal complex (OMC) obstruction and thereby normalize this transport.
The goal is to:
- Remove irreversibly diseased mucosa and bone
- Preserve normal tissue and mucosal lining (skull base, lamina papyracea, sinus cavities)
- Judiciously widen the true natural ostia of the sinuses
- Leave uninvolved sinuses alone
The term "full-house" FESS refers to complete sphenoethmoidectomy with Draf IIA frontal sinusotomy.
— Cummings Otolaryngology Head and Neck Surgery
2. Historical Background
| Year | Milestone |
|---|---|
| 1675 | Molinetti described surgical approach to maxillary sinus via its anterior wall |
| 1890s | Caldwell, Spicer & Luc — Caldwell-Luc procedure (primary treatment for CRS for decades) |
| 1901 | Hirschmann — first endoscopic nasal examination with modified cystoscope |
| 1950s | Hopkins rod lens development enabled modern endoscopy |
| 1978 | Messerklinger published his ESS experience; highlighted the OMC's role in rhinosinusitis pathophysiology |
| 1985 | Kennedy introduced ESS to the United States |
Stamberger (Messerklinger's resident) was instrumental in popularizing the technique outside Germany and Austria.
3. Indications
FESS is indicated when adequate medical therapy has failed to control:
- Chronic Rhinosinusitis (CRS) — with or without nasal polyps (CRSwNP / CRSsNP)
- Allergic fungal sinusitis (AFS)
- Recurrent acute rhinosinusitis
- Complicated acute rhinosinusitis
- Mucocele or pyocele of sinuses
- Sinonasal polyposis
- Cystic fibrosis-related sinusitis
- Primary ciliary dyskinesia
- Orbital or intracranial extension of sinus disease (often urgent)
Patients should generally fail optimal medical therapy (intranasal corticosteroids, saline irrigation, appropriate antibiotics) before being considered surgical candidates.
4. Preoperative Assessment
History
Factors associated with poorer outcomes must be identified:
- Smoking
- Asthma
- Aspirin-exacerbated respiratory disease (Samter's triad)
- Allergies
- Immunodeficiency
- Depression
Physical Examination
- Complete head and neck examination
- Basic ocular examination
- Anterior rhinoscopy — detects septal deviation, nasal valve collapse
- Nasal endoscopy (rigid or flexible) — character of mucosa, sinus drainage pathways, purulent drainage, polyps, anatomic variations
Radiographic Assessment
- CT scan (non-contrast) — modality of choice; provides excellent bone detail; assesses sinonasal anatomy and disease extent; used for preoperative planning and image-guided navigation
- Lund-Mackay score — quantifies disease burden on CT
- MRI — indicated if bony dehiscence or erosion of skull base / lamina papyracea is present (to differentiate inflammatory disease from tumors or encephaloceles)
- CT should be obtained 3–4 weeks after maximal medical therapy to avoid operating on acute inflammatory changes
5. Key Anatomy Relevant to FESS
Osteomeatal Complex (OMC)
The OMC is a functional concept, not a discrete anatomic structure. It is the final common pathway for drainage and ventilation of the ethmoidal, maxillary, and frontal sinuses. It comprises:
- Uncinate process
- Ethmoidal infundibulum
- Hiatus semilunaris
- Anterior ethmoidal cells
- Maxillary sinus ostium
- Frontal recess
Critical Landmarks
- Lamina papyracea — medial orbital wall; breach causes orbital fat herniation or orbital hematoma
- Skull base / fovea ethmoidalis — breach causes CSF leak
- Optic nerve — at risk in posterior ethmoid / sphenoid surgery
- Internal carotid artery — lies within the sphenoid sinus walls
- Keros classification of olfactory cleft depth determines skull base risk
- Asymmetry in ethmoid roof height — increases risk of intracranial penetration
6. Surgical Technique: Step-by-Step
FESS typically proceeds in a lateral-to-medial (Messerklinger) approach:
Step 1 — Uncinectomy
- The uncinate process is the first structure removed
- A sickle knife or backbiter punch is used to detach it
- Retrograde uncinectomy: initiated at the junction of upper two-thirds and lower one-third, extending anteriorly to the anterior maxillary line (M)
- Removal exposes the ethmoidal infundibulum and the maxillary sinus ostium
Step 2 — Anterior Ethmoidectomy
- Anterior ethmoidal air cells (agger nasi, bulla ethmoidalis) are systematically opened
- The bulla ethmoidalis — the largest and most consistent anterior ethmoid cell — is opened
- A thorough ethmoidectomy with complete removal of cells is critical for successful maxillary antrostomy and frontal sinusotomy
Step 3 — Maxillary Antrostomy
- The maxillary ostium is elliptical and found in the floor of the infundibulum lateral to the lower third of the uncinate
- Requires a 30° or 45° angled endoscope for optimal visualization
- The ostium is gently dilated posteriorly with a maxillary sinus seeker
- Key principle: the antrostomy must incorporate the natural ostium — opening an accessory ostium while missing the natural ostium leads to mucus recirculation and persistent infection
- Any accessory ostia present must be incorporated into the antrostomy
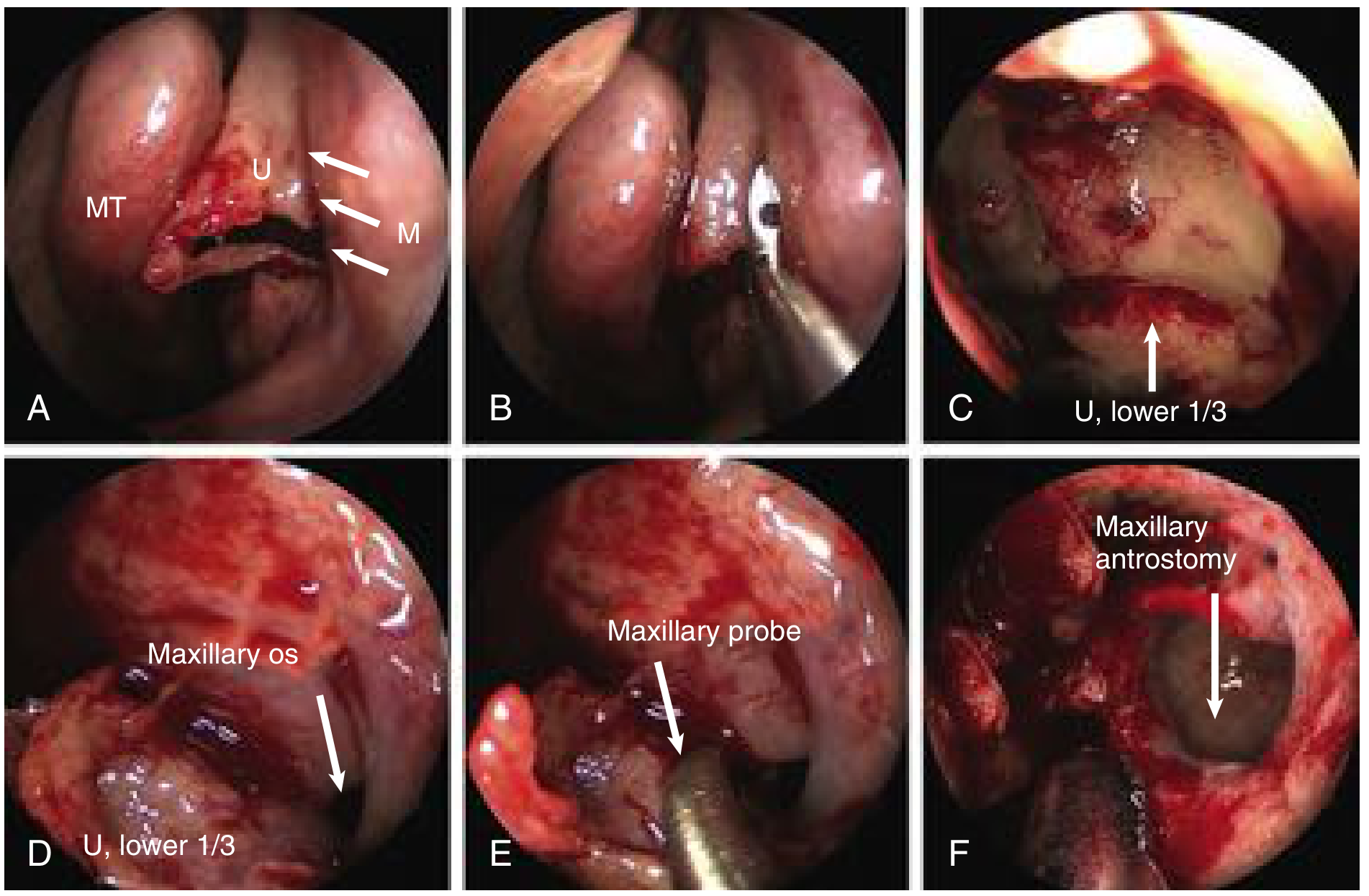
Endoscopic views of retrograde uncinectomy and maxillary antrostomy. (A) Uncinectomy initiated with backbiter at junction of upper two-thirds/lower one-third. (B) Upper uncinate removed. (C–D) Lower one-third uncinate exposed; maxillary os visible. (E) Maxillary probe dilating ostium. (F) Completed pear-shaped maxillary antrostomy. MT = middle turbinate.
Step 4 — Posterior Ethmoidectomy
- Posterior ethmoidal cells are entered by piercing the basal lamella (ground lamella) of the middle turbinate
- Care taken around the lamina papyracea and skull base
Step 5 — Sphenoidotomy
- The sphenoid sinus is accessed via the natural ostium (found ~1–1.5 cm above the choanal arch)
- Key risks: optic nerve (superolateral wall), internal carotid artery (lateral wall)
Step 6 — Frontal Sinusotomy (Draf Procedures)
- Draf I: removal of anterior ethmoidal cells that block frontal recess
- Draf IIA: unilateral frontal sinusotomy (medial to middle turbinate insertion)
- Draf IIB: removal of floor of frontal sinus from septum to lamina papyracea
- Draf III (modified Lothrop): bilateral Draf IIB with removal of upper nasal septum — creates single drainage pathway; maximum frontal exposure
7. Extent of Surgery
The extent is individualized based on disease subtype and patient factors:
| Disease | Approach |
|---|---|
| Limited CRS | Limited surgery (targeted OMC opening) |
| Eosinophilic CRS / CRSwNP | More extensive surgery |
| Complicated acute rhinosinusitis | Extensive surgery |
| "Large hole" surgery | For optimizing topical drug delivery postoperatively |
8. Image-Guided Surgery (IGS / Navigation)
- CT-based intraoperative navigation helps identify landmarks in complex or revision cases
- Particularly useful in: revision surgery, extensive polyposis, skull base or orbital wall dehiscence, anatomic distortion
- Does not replace surgical knowledge of anatomy
9. Postoperative Care
Postoperative care is critical for outcomes:
- Nasal saline irrigation — clears crusts and debris
- Intranasal corticosteroid sprays or rinses
- Endoscopic debridement in the office — removes crusts, adhesions, and residual secretions in the weeks following surgery
- Systemic steroids and antibiotics as indicated
- Detailed postoperative follow-up reduces adhesion formation and scarring
10. Complications
Minor Complications
- Bleeding / epistaxis
- Periorbital bruising or edema
- Adhesion formation (synechiae)
- Hyposmia / anosmia
Major Complications
| Complication | Cause |
|---|---|
| CSF leak | Skull base breach (fovea ethmoidalis or cribriform plate) |
| Blindness | Optic nerve injury or retrobulbar hematoma |
| Diplopia | Medial rectus or inferior rectus injury |
| Internal carotid artery injury | Lateral sphenoid wall breach — potentially fatal |
| Orbital hematoma | Lamina papyracea breach with arterial injury |
| Death | Rare; from massive hemorrhage or intracranial injury |
Risk of intracranial penetration is higher when there is asymmetry in ethmoid roof height (a Keros classification consideration).
11. Causes of Failure / Revision Surgery
Technical Failures (Surgical)
- Lateralized middle turbinate — obstructs the operated sinus
- Failure to incorporate maxillary ostium in middle meatal antrostomy → mucus recirculation
- Maxillary ostium stenosis
- Frontal recess scarring
- Residual ethmoidal air cells
- Adhesions / synechiae
- Unidentified Haller cells (infraorbital ethmoid cells) or Onodi cells (sphenoethmoid cells) causing persistent obstruction
- Incomplete uncinate removal
Disease-Related Failures
- Middle turbinate lateralization
- Neo-osteogenesis — new bone formation
- Recurrent nasal polyposis
Patient Conditions with Higher Revision Rates
- CRS with nasal polyps (CRSwNP)
- Allergic fungal sinusitis
- Disorders of mucociliary clearance (e.g., primary ciliary dyskinesia, cystic fibrosis)
- Underlying biofilms
- Immunodeficiencies
- Aspirin-exacerbated respiratory disease (AERD)
Failure to recognize non-sinogenic or comorbid systemic disease prior to primary FESS often results in poor outcomes.
12. Outcomes
- FESS provides significant improvement in overall and disease-specific quality of life
- High success rate when combined with appropriate medical therapy
- Symptom improvement rates of 80–90% in well-selected patients for CRS
- Surgery must be coupled with lifelong postoperative medical management (especially in CRSwNP, AERD, AFS)
Summary
| Feature | Detail |
|---|---|
| Goal | Restore mucociliary clearance via OMC opening |
| Primary target | Osteomeatal complex |
| Imaging | CT (preoperative); intraoperative CT navigation in select cases |
| First step in OR | Uncinectomy |
| Most critical principle | Preserve mucosa; open natural (not accessory) ostia |
| Major risks | CSF leak, blindness, carotid injury |
| Key to success | Adequate surgery + postoperative medical care + office debridement |
— Cummings Otolaryngology Head and Neck Surgery; K J Lee's Essential Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.