Pancreatitis everthing about it
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
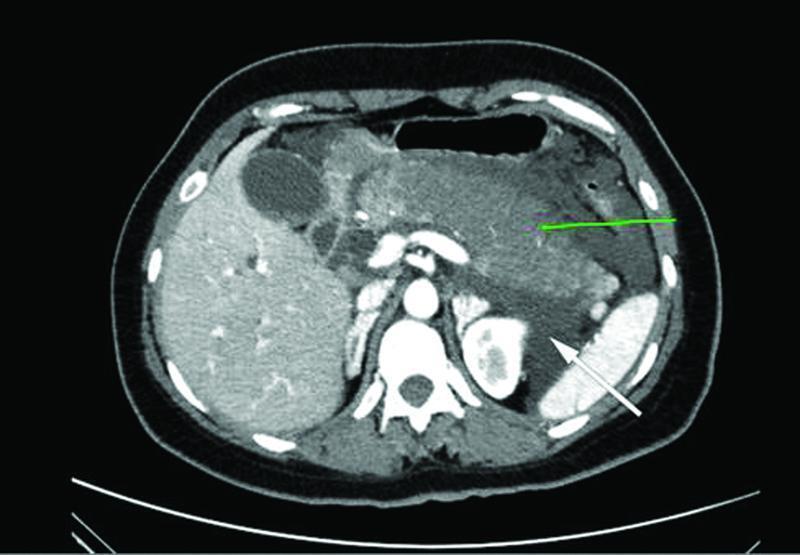
acute pancreatitis CT scan pathology
I now have comprehensive information from the textbooks. Let me compile the full answer:
Pancreatitis — Complete Overview
Definition
Pancreatitis is inflammation of the pancreas. It exists on a spectrum:
- Acute pancreatitis — a discrete episode of cellular injury with potential for full recovery
- Chronic pancreatitis — irreversible parenchymal destruction and fibrosis
- Recurrent acute episodes can transition into chronic pancreatitis; the two are on a continuum
— Goldman-Cecil Medicine, p. 1521
Epidemiology
- Incidence: ~40 cases per 100,000 in the United States; ~300,000 hospital admissions/year
- One of the most common GI discharge diagnoses in US hospitals
- Cost: $4–6 billion annually
- Incidence is rising — driven by the obesity epidemic, increasing gallstone prevalence, and more frequent diagnostic testing
- Overall mortality: ~5% (higher in necrotizing disease)
- Alcoholic pancreatitis peaks in ages 20–50; more common in men
— Goldman-Cecil Medicine, p. 1519–1521; Robbins Basic Pathology, p. 635
Causes & Risk Factors
Gallstones and alcohol together account for ~80% of all cases.
| Category | Examples |
|---|---|
| Gallstones | Passage of stone through ampulla of Vater; microlithiasis/biliary sludge |
| Alcohol | Typically >5 years of >5–8 drinks/day; mechanism = direct toxicity + oxidative stress |
| Drugs/Toxins | Azathioprine, 6-mercaptopurine (up to 4% attack rate), valproic acid, thiazides, furosemide, pentamidine, didanosine, L-asparaginase, sulfonamides, scorpion venom, organophosphates |
| Metabolic | Hypertriglyceridemia (>1000 mg/dL; 5–10% of cases), hypercalcemia, hyperparathyroidism |
| Trauma | Post-ERCP (5–10% incidence; up to >20% in high-risk), blunt/penetrating trauma, postoperative |
| Obstruction | Pancreatic/ampullary strictures, pancreatic cancer, IPMN, Crohn's disease, periampullary diverticulum |
| Infections | Mumps, Coxsackievirus B, CMV, rubella, Candida, Ascaris lumbricoides, Clonorchis sinensis |
| Genetic | PRSS1 (cationic trypsinogen) mutations, SPINK1 (trypsin inhibitor) mutations, CFTR mutations |
| Autoimmune | Type 1 (IgG4-related), Type 2 |
| Idiopathic | 10–20% of cases |
Key facts:
- Only ~5% of patients with gallstones develop pancreatitis; those with smaller stones (≤5 mm) are at highest risk
- Most patients with a first episode of alcoholic pancreatitis already have underlying chronic pancreatitis
— Goldman-Cecil Medicine, p. 1522; Robbins Basic Pathology, p. 635
Pathophysiology
The final common pathway is premature intracellular activation of digestive proenzymes within acinar cells:
- Trigger (stone obstruction, alcohol, toxin, etc.) disrupts normal secretion of zymogens
- Trypsinogen → Trypsin (via elevated intracellular calcium) — the critical initiating step
- Trypsin then activates other proteases (elastase, phospholipase A2, lipase, kallikrein)
- Autodigestion of pancreatic parenchyma → fat necrosis, cell death, hemorrhage
- Release of pro-inflammatory cytokines (IL-1, IL-6, TNF-α) and activated enzymes into systemic circulation → SIRS → organ failure (hypotension, AKI, ARDS)
- Fluid extravasation into retroperitoneal spaces ("third space" losses)
Genetic context: Mutations in PRSS1 cause gain-of-function (easier trypsin activation); SPINK1 mutations reduce trypsin inhibition; CFTR mutations alter ductal fluid composition — all lower the threshold for autodigestion.
— Goldman-Cecil Medicine, p. 1521; Robbins Basic Pathology, p. 635–636
Classification (Revised Atlanta, 2012)
By Type
| Type | CT Finding | Key Feature |
|---|---|---|
| Interstitial edematous pancreatitis | Diffuse enlargement, peripancreatic fat stranding | Necrosis NOT visible on CT — milder |
| Necrotizing pancreatitis | Non-enhancing areas of pancreatic parenchyma | Necrosis visible on contrast-enhanced CT |
By Severity
| Severity | Features | Mortality |
|---|---|---|
| Mild | No organ failure, no local complications | <1% |
| Moderately severe | Transient organ failure (<48 h) and/or local complications | ~1–5% |
| Severe | Persistent organ failure (>48 h) — single or multiorgan | Up to 30–50% (infected necrosis) |
Clinical Presentation
- Abdominal pain — hallmark; typically epigastric or periumbilical, radiating to the back; constant, severe, often "boring" in quality; worse supine, better leaning forward
- Nausea and vomiting — nearly universal
- Fever — low-grade initially; high fever suggests infection/sepsis
- Tachycardia, hypotension — from third-space losses and SIRS
- Abdominal tenderness — diffuse or localized to epigastrium; guarding/rigidity in severe cases
- Distension/ileus — from peritoneal irritation
Rare physical signs (severe/hemorrhagic pancreatitis):
- Cullen's sign — periumbilical ecchymosis (retroperitoneal hemorrhage tracking anteriorly)
- Grey Turner's sign — flank ecchymosis (same mechanism)
- Jaundice — if common bile duct compression or concomitant choledocholithiasis
— Goldman-Cecil Medicine, p. 1521
Diagnosis
Diagnostic Criteria (any 2 of 3 required):
- Characteristic abdominal pain
- Serum amylase or lipase ≥ 3× upper limit of normal
- Characteristic findings on imaging (CT/MRI/US)
Laboratory Tests
| Test | Significance |
|---|---|
| Serum lipase | Preferred over amylase — more sensitive and specific; remains elevated longer (up to 14 days) |
| Serum amylase | Rises within hours, returns to normal in 3–5 days; less specific (also elevated in salivary gland disease, renal failure, bowel obstruction) |
| Liver enzymes (ALT, AST, bilirubin) | ALT >3× ULN has ~95% positive predictive value for gallstone pancreatitis |
| CBC | Leukocytosis common; hemoconcentration (Hct >44%) indicates severe disease |
| BUN/Creatinine | BUN >20 mg/dL or rising BUN = poor prognosis |
| CRP | CRP >150 mg/L at 48 h correlates with necrosis |
| Triglycerides | Check if no obvious cause |
| Calcium | Hypocalcemia in severe disease (saponification of peripancreatic fat) |
Imaging
Ultrasound — first-line for all patients:
- Identifies gallstones, biliary dilation
- Limited pancreatic visualization due to bowel gas
Contrast-enhanced CT (CECT) — standard for severity assessment:
- Indicated when diagnosis is uncertain, or if no improvement in 48–72 hours
- Identifies necrosis (areas of non-enhancement), fluid collections, vascular complications
- CT Severity Index (Balthazar score) grades A–E based on inflammation and necrosis
MRI/MRCP — excellent for:
- Choledocholithiasis without ERCP radiation risk
- Identifying duct disruption
- Allergy to iodinated contrast

Severity Scoring
| Score | Parameters | Use |
|---|---|---|
| BISAP | BUN >25, impaired mental status, SIRS, age >60, pleural effusion — 1 point each | Early (first 24 h) |
| Ranson's criteria | 11 criteria (5 on admission, 6 at 48 h) | Classic but cumbersome |
| APACHE-II | Physiologic + age + chronic health | Any time; complex |
| CTSI (Balthazar) | CT grade + % necrosis | At 48–72 h |
Complications
Local Complications
| Complication | Description |
|---|---|
| Acute peripancreatic fluid collection (APFC) | Early (<4 wk), no defined wall; most resolve spontaneously |
| Pancreatic pseudocyst | Mature APFC with defined wall, >4 weeks; fluid only (no solid debris) |
| Acute necrotic collection (ANC) | Early necrotic material; solid + liquid |
| Walled-off necrosis (WON) | Mature ANC with defined wall, >4 weeks; contains solid necrotic debris |
| Infected necrosis | Fever + rising WBC + gas on CT; mortality 15–30% even with treatment |
| Pancreatic duct disruption | Can cause pseudocyst, pancreatic fistula, or "disconnected duct syndrome" |
Systemic Complications
- ARDS / respiratory failure (pleural effusion, atelectasis, ARDS)
- Acute kidney injury
- Shock (distributive, hypovolemic)
- DIC
- Hypocalcemia (fat saponification)
- Hyperglycemia
- Ileus
- Splenic/portal/mesenteric vein thrombosis
- Pseudoaneurysm (splenic artery most common) → can rupture
Management
Acute Pancreatitis — General Principles
1. Fluid Resuscitation
- Most critical early intervention
- Lactated Ringer's (LR) preferred over normal saline — lower risk of acidosis and possibly reduced SIRS
- Goal-directed: 250–500 mL/hr initially; reassess at 6 and 24 hours
- Aggressive hydration (>4 L in first 24 h) may be harmful in elderly/cardiac patients
- Markers of adequate resuscitation: urine output >0.5 mL/kg/hr, decreasing BUN, HR normalization
2. Pain Control
- IV opioid analgesia (e.g., hydromorphone or fentanyl) — morphine historically avoided but current evidence shows no increased sphincter-of-Oddi pressure clinically
- NSAIDs and epidural analgesia used in some centers
3. Nutrition
- Oral feeding should be started as early as tolerated (as soon as pain improving and patient hungry)
- Enteral nutrition (via nasojejunal or even nasogastric tube) preferred over parenteral in severe pancreatitis
- Total parenteral nutrition (TPN) only if enteral route is not feasible
- "NPO" protocols are now discouraged in mild pancreatitis
4. No Role for Routine Antibiotics
- Prophylactic antibiotics do NOT prevent infected necrosis and are not recommended
- Antibiotics only if confirmed/strongly suspected infected necrosis (imipenem or meropenem ± antifungal)
5. Cause-Specific Interventions
- Gallstone pancreatitis: Urgent ERCP (within 24 h) ONLY if concurrent acute cholangitis; cholecystectomy should be performed during the same admission (mild) or after resolution (severe) to prevent recurrence
- Hypertriglyceridemia: Insulin infusion (activates lipoprotein lipase), plasmapheresis in extreme cases
- Alcohol: Cessation counseling; treat withdrawal
- Drug-induced: Discontinue offending drug
6. Management of Complications
- Infected necrosis: Step-up approach — percutaneous drainage first, then endoscopic (transluminal) or minimally invasive surgical necrosectomy if failing
- Pancreatic pseudocyst: Expectant management if asymptomatic; endoscopic drainage (cyst-gastrostomy) if symptomatic or enlarging
- Walled-off necrosis: Endoscopic transmural drainage ± necrosectomy (lumen-apposing metal stent)
- Open surgical necrosectomy is a last resort due to high morbidity
— Goldman-Cecil Medicine, p. 1521–1522
Chronic Pancreatitis
Definition & Pathology
Chronic pancreatitis is irreversible parenchymal destruction with fibrosis, replacement of exocrine tissue, and eventual endocrine failure. Unlike acute pancreatitis, normal function is not restored.
Causes
- Chronic alcohol use — most common in adults
- Genetic — PRSS1, SPINK1, CFTR mutations (especially in young patients)
- Autoimmune (IgG4-related — Type 1; duct-centric — Type 2)
- Tropical pancreatitis — malnourishment, cassava toxin (Southeast Asia, Africa)
- Obstructive — pancreatic duct stricture, tumor
- Idiopathic — significant proportion
Clinical Features
- Chronic abdominal pain — epigastric, radiating to back; often persistent; can be paroxysmal
- Exocrine insufficiency (late):
- Steatorrhea (>90% exocrine function must be lost before malabsorption occurs)
- Weight loss, malnutrition
- Fat-soluble vitamin deficiencies (A, D, E, K)
- Endocrine insufficiency (late):
- Diabetes mellitus (Type 3c or "pancreatogenic diabetes")
- Brittle insulin-dependent diabetes (also loss of glucagon → hypoglycemia risk)
- Obstructive jaundice — fibrotic compression of common bile duct
- Pancreatic cancer risk — significantly increased (cumulative lifetime risk ~4%)
Diagnosis of Chronic Pancreatitis
- CT scan: Pancreatic calcifications (pathognomonic), ductal dilation, atrophy
- MRCP/EUS: Ductal changes (chain-of-lakes), parenchymal changes
- Fecal elastase-1 (<200 µg/g stool) — most widely used test for exocrine insufficiency
- 72-hour fecal fat — quantifies fat malabsorption
- Secretin-stimulated MRI/MRCP — functional assessment
- Serum IgG4 — elevated in autoimmune pancreatitis Type 1
Management of Chronic Pancreatitis
| Problem | Treatment |
|---|---|
| Pain | Analgesic ladder (NSAIDs → opioids); pancreatic enzyme supplements (reduce CCK-stimulated secretion); celiac plexus block; endoscopic duct drainage/stone removal; ESWL (extracorporeal shockwave lithotripsy); surgery (Whipple, Puestow/Partington procedure, Frey procedure) |
| Exocrine insufficiency | Pancreatic enzyme replacement therapy (PERT) with meals — lipase ≥40,000–50,000 IU/meal; add PPI to prevent enzyme inactivation |
| Endocrine insufficiency | Insulin therapy; tight glucose control; caution — glucagon also deficient → hypoglycemia risk |
| Obstruction/ductal dilation | Endoscopic stenting, ESWL, or surgery depending on anatomy |
| Autoimmune pancreatitis | Steroids (prednisone) — dramatic response is diagnostic; relapse treated with azathioprine |
Pathology (Gross & Microscopic)
Acute Pancreatitis
- Mild/interstitial: Edema, focal fat necrosis, mild inflammatory infiltrate
- Severe/necrotizing: Widespread hemorrhagic necrosis; chalky white fat necrosis (calcium soap deposits); destruction of acini, ducts, and islets; pseudocyst formation possible
Chronic Pancreatitis
- Irreversible fibrosis, loss of acinar tissue
- Dilated ducts filled with inspissated protein plugs and calculi
- Relatively preserved islets of Langerhans (initially), then progressive islet loss
- Eventual atrophy of the entire gland
— Robbins Basic Pathology, p. 635–636; Goldman-Cecil Medicine, p. 1522
Prevention of Recurrence
| Cause | Prevention Strategy |
|---|---|
| Gallstones | Cholecystectomy (same admission if mild; after recovery if severe) |
| Alcohol | Complete cessation |
| Hypertriglyceridemia | Fibrates, diet, omega-3s |
| Drugs | Discontinue and avoid offending agent |
| Post-ERCP | Prophylactic pancreatic stent placement; rectal indomethacin (NSAIDs) in high-risk patients |
Key Points Summary
| Feature | Acute | Chronic |
|---|---|---|
| Reversibility | Yes (if cause removed) | No |
| Main causes | Gallstones (most common), alcohol | Alcohol, genetic, autoimmune |
| Key enzyme | Lipase (preferred), amylase | Fecal elastase (exocrine function) |
| Best imaging | CECT (severity/necrosis) | CT (calcifications), MRCP/EUS |
| Critical treatment | IV fluids (LR), early oral feeding | PERT, pain management, insulin |
| Dreaded complication | Infected necrosis (30–50% mortality) | Pancreatic cancer, brittle diabetes |
Sources: Goldman-Cecil Medicine 26th ed., pp. 1519–1522 | Robbins & Kumar Basic Pathology, pp. 635–636 | Sleisenger & Fordtran's GI and Liver Disease | Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.