Macular sparring
Reading File
Finding Sources
Searching the Web
macular sparing visual field defect mechanism occipital lobe
Reading File
Reading File
Reading File
Loading Image
Reading File
Excellent - I now have thorough information to compile a comprehensive answer. Here is the complete explanation:
Macular Sparing
Definition
Macular sparing is a visual field defect pattern in which the central (macular) region of vision is preserved despite significant peripheral or hemianopic loss. It is the opposite of macular splitting, where the vertical midline cuts precisely through the central field.
Anatomy Recap: Why the Macula Is Special
The macula (central ~5 degrees of the visual field) has a disproportionately large cortical representation at the occipital pole (tip of the occipital lobe). This area receives blood supply from two sources:
- The posterior cerebral artery (PCA) - supplies most of the visual cortex
- The middle cerebral artery (MCA) - gives collaterals to the occipital pole
This dual supply is the key to understanding macular sparing.
Mechanisms
1. Dual Vascular Supply (most accepted)
When a PCA stroke infarcts the occipital cortex, the MCA collaterals can still perfuse the occipital pole (macular cortex). Peripheral field cortex - further from the pole - loses its only PCA supply and infarcts. Central vision is thus spared.
2. Bilateral Macular Representation
The macula projects to both hemispheres to some degree (overlap around the vertical meridian), meaning a unilateral lesion may spare macular input from the contralateral hemisphere.
3. Cortical Magnification
The macular representation is so large relative to peripheral fields that a single lesion must extend a considerable distance to destroy all macular neurons. As Ganong states: "occipital lesions must extend considerable distances to destroy both macular and peripheral vision." - Ganong's Review of Medical Physiology, 26th Ed.
Classic Patterns
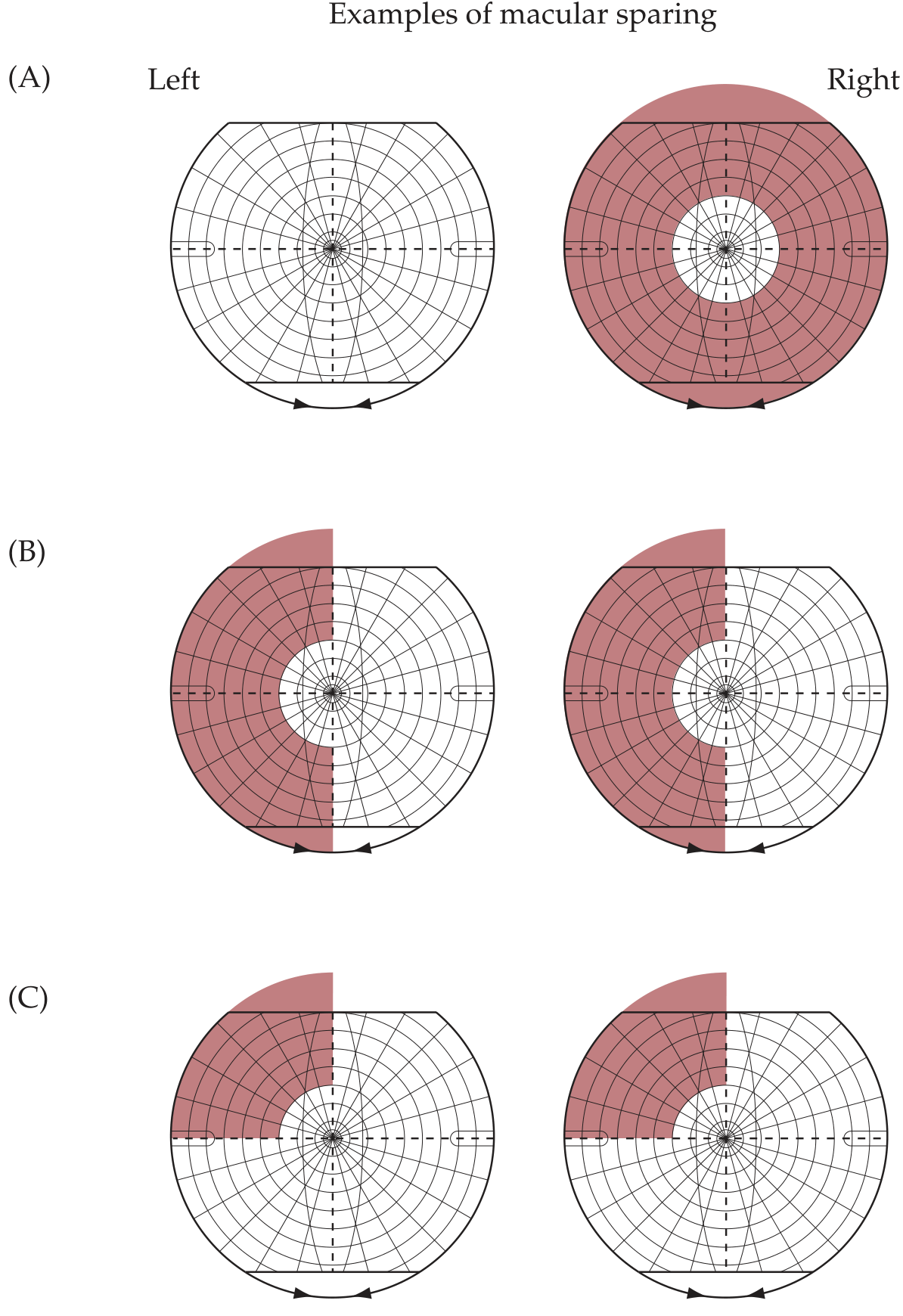
The diagram above (from Neuroanatomy through Clinical Cases) shows three classic patterns:
| Pattern | Description | Typical Cause |
|---|---|---|
| (A) Monocular concentric loss | Peripheral loss with central sparing in one eye | Chronic elevated ICP, retinitis pigmentosa |
| (B) Homonymous hemianopia with macular sparing | Left field lost in both eyes, central circle intact | Right PCA infarct sparing occipital pole |
| (C) Superior quadrantanopia with macular sparing | Left upper quadrant lost, macula intact | Lesion of inferior bank of right calcarine fissure |
Where in the Visual Pathway Does It Occur?
Macular sparing is characteristic of lesions at or behind the geniculocalcarine tract (optic radiations) / visual cortex.
- Optic nerve, chiasm, or optic tract lesions do NOT produce macular sparing - they split the macula cleanly
- Geniculocalcarine tract lesions: cause homonymous hemianopia with macular sparing
- Primary visual cortex (V1/calcarine cortex) lesions: most common cause; sparing of the occipital pole = sparing of macula
Key rule: Macular sparing suggests an occipital (cortical) origin of the hemianopia, rather than a tract or radiation lesion. - Neuroanatomy through Clinical Cases, 3rd Ed.
Bilateral Occipital Lesions
Bilateral occipital infarcts can cause bilateral homonymous hemianopia (cortical blindness) but may leave a small "keyhole" of central vision intact - this is called keyhole vision or tunnel of central macular sparing. Rarely, patients with cortical blindness deny their defect (Anton syndrome). - Localization in Clinical Neurology, 8th Ed.
Clinical Significance
- Lesion localization - Macular sparing points to an occipital cortex lesion (typically PCA territory infarct), distinguishing it from optic tract or LGN lesions, which produce macular splitting.
- Preserved reading ability - Because the macula handles fine detail/central vision, macular sparing can preserve the ability to read, recognize faces, and perform tasks requiring central acuity, even with large peripheral field loss.
- Differential diagnosis - Not all central sparing is macular sparing. Tunnel vision (e.g., glaucoma, retinitis pigmentosa) is monocular peripheral loss; true macular sparing is binocular and homonymous.
Macular Sparing vs. Macular Splitting
| Feature | Macular Sparing | Macular Splitting |
|---|---|---|
| Central field | Intact | Lost (bisected by midline) |
| Typical location | Occipital cortex (PCA territory) | Optic tract, LGN, optic radiation |
| Vascular cause | PCA infarct with MCA collaterals | MCA territory infarct |
| Reading ability | Usually preserved | Often impaired |
Sources:
- Neuroanatomy through Clinical Cases, 3rd Ed. (Blumenfeld), Figures 11.16, p. 501
- Costanzo Physiology, 7th Ed., Optic Pathways section
- Ganong's Review of Medical Physiology, 26th Ed., Effect of Lesions in the Optic Pathways
- Localization in Clinical Neurology, 8th Ed., Chiasmal Syndrome chapter
This is a shared conversation. Sign in to Orris to start your own chat.