EXAMINATION OF SURGICAL PATIENTS, PATIENT SUPERVISION & MODERN TECHNOLOGIES IN SURGERY.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive, well-structured answer. Here it is:
Examination of Surgical Patients, Patient Supervision & Modern Technologies in Surgery
PART I — EXAMINATION OF SURGICAL PATIENTS
1. Principles of Preoperative Evaluation
The history and physical examination are the foundation of surgical patient assessment and have repeatedly been shown to be the most valuable parts of preoperative evaluation. The following steps must be completed before moving a patient to the operating room:
- A comorbidity-focused history and physical examination
- Appropriate laboratory studies and medical consultations
- An anesthesiologist's preoperative evaluation with assignment of an ASA physical status classification
- Discussion with the patient of options and risks
- Development and communication of the anesthetic plan to the patient and surgeon
- Acute optimization of any pertinent medical conditions
— Mulholland and Greenfield's Surgery, 7e
2. The Preoperative History
History-taking should focus on:
- Key comorbid conditions (e.g., diabetes, coronary artery disease) that pose known perioperative risks
- Full review of systems: chest discomfort, dyspnea, functional capacity
- Cardiovascular history: symptoms, exercise tolerance, prior cardiac events
- Past surgical history: ability to withstand surgical stress, previous anesthesia complications (bleeding, cognitive changes)
- Family history: bleeding disorders, malignant hyperthermia
- Medication history (complete, including OTC, herbal, opioids, illicit substances)
- Allergies: medications, foods, latex
- Social habits: smoking, alcohol (relevant for planning cessation and avoiding withdrawal)
A complete medication history is a key aspect because many recommendations will relate to the longitudinal management of medications during the perioperative period. — Goldman-Cecil Medicine, 26e
3. Functional Capacity Assessment
Functional capacity is quantified in metabolic equivalents (METs):
| METs | Activity |
|---|---|
| 1 MET | Self-care, walking indoors |
| 4 METs | Climbing one flight of stairs, walking on level ground at 4 mph |
| >4 METs | Heavy housework, running a short distance |
Patients sustaining ≥4 METs are considered lower risk even with existing medical illness. Frail patients unable to achieve this threshold are at higher risk. When functional status cannot be assessed (e.g., due to orthopedic problems), clinical assessment of comorbid conditions and specialized risk indices become especially important.
4. Physical Examination of the Surgical Patient
The examination must include:
- Basic physiologic measures: pulse, blood pressure, weight
- Cardiac: auscultation for murmurs (specifically assess for aortic stenosis), volume status (S₃ gallop, rales, peripheral edema)
- Pulmonary: oxygen saturation, auscultation for wheeze (especially in COPD), peripheral edema
- Neurological: baseline mental status, history of delirium or chronic cognitive impairment
- General survey: appropriate to patient's age, gender, and specific surgical region
- Airway/dentition: primarily assessed by the anesthesiologist; abnormalities must be relayed
Point-of-care ultrasound, though promising, is not currently part of standard preoperative evaluation.
5. Preoperative Diagnostic Testing
Testing in asymptomatic patients rarely provides useful information; testing should be targeted based on history and physical examination findings:
| Clinical Finding | Recommended Test |
|---|---|
| Family history of bleeding | Coagulation studies |
| Systolic murmur | Echocardiogram (rule out aortic stenosis) |
| Age >40 or cardiac disease | Baseline ECG |
| Inpatients under general anesthesia / lung disease | Chest radiograph |
| Chronic kidney disease | Baseline creatinine |
| COPD | Arterial blood gases, pulmonary function tests |
6. ASA Physical Status Classification
(Mulholland and Greenfield's Surgery, 7e)
| Class | Description | Perioperative Mortality |
|---|---|---|
| PS-1 | Normal healthy patient | <0.03% |
| PS-2 | Mild systemic disease, no functional limitation (e.g., hypertension, diabetes, obesity) | ~0.2% |
| PS-3 | Severe systemic disease with functional limitation (e.g., poorly controlled HTN, prior MI, angina) | ~1.2% |
| PS-4 | Severe disease, constant threat to life (e.g., CHF, unstable angina, advanced organ failure) | ~8% |
| PS-5 | Moribund, not expected to survive without surgery (e.g., ruptured AAA, massive PE) | ~34% |
| PS-6 | Brain-dead donor | |
| E | Emergency operation suffix (e.g., PS-1E) |
The combined risk of perioperative all-cause death, AMI, or ischemic stroke in adult patients undergoing major noncardiac surgery in the U.S. is approximately 3%.
7. Approach by Surgical Urgency
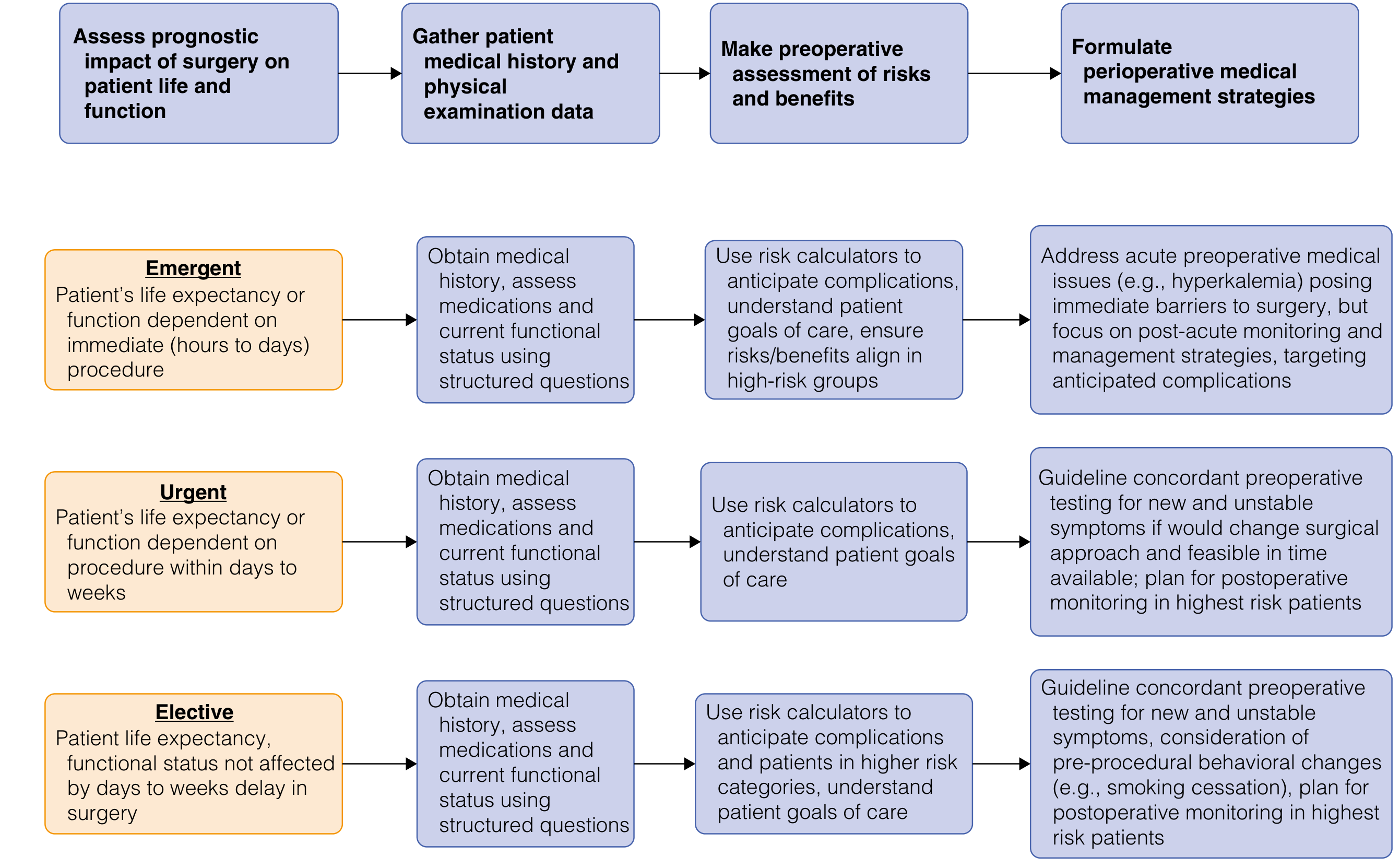
Emergent surgery: Focus on post-acute monitoring and management strategies; address only immediate barriers (e.g., hyperkalemia)
Urgent surgery: Guideline-concordant testing only if results would change surgical approach; plan for postoperative monitoring in highest-risk patients
Elective surgery: Full guideline-concordant testing; consideration of pre-procedural behavioral changes (e.g., smoking cessation); plan postoperative monitoring for highest-risk patients
PART II — PATIENT SUPERVISION (PERIOPERATIVE MONITORING)
1. Preoperative Supervision
- Assessment and preparation of the patient for anesthesia
- Cardiac evaluation using validated risk indices:
Revised Cardiac Risk Index (RCRI) — assign 1 point each for:
- History of ischemic heart disease
- History of heart failure
- History of cerebrovascular accident or TIA
- Insulin-dependent diabetes mellitus
- Serum creatinine ≥2.0 mg/dL
- Intraperitoneal, intrathoracic, or suprainguinal vascular surgery
NSQIP MICA calculator factors in: age, functional status, ASA class, creatinine, surgery type (available at riskcalculator.facs.org).
If estimated cardiovascular risk >1% and poor functional capacity, consider pharmacologic stress testing (adenosine/dipyridamole nuclear stress test or dobutamine echocardiography) — only if the patient is a candidate for revascularization and delay is feasible.
2. Surgical Risk Stratification by Procedure Type
| Risk Category | Cardiac Risk | Examples |
|---|---|---|
| High (>5%) | Emergent, aortic/major vascular surgery | Ruptured AAA repair, major vascular surgery |
| Intermediate (1–5%) | Intraperitoneal, intrathoracic, carotid endarterectomy, head/neck, orthopaedic, prostate | Abdominal surgery, EVAR |
| Low (<1%) | Superficial, cataract, breast, ambulatory | Cataract surgery, skin surgery |
3. Intraoperative Monitoring
Key intraoperative parameters monitored by the anesthesiologist include:
- Continuous ECG, pulse oximetry, capnography
- Blood pressure (non-invasive or invasive arterial line for high-risk cases)
- Temperature monitoring (prevention of hypothermia)
- Spinal cord monitoring (somatosensory/motor evoked potentials) for spine surgery
- Neuromuscular blockade monitoring
4. Postoperative Supervision
Postoperative care involves assessment, evaluation, and preparation for discharge, encompassing:
- ICU-level monitoring for high-risk patients (neurosurgery, major vascular, cardiac): 24-hour monitoring with frequent neurologic checks, then step-down to floor on POD 1
- Vital signs (HR, BP, SpO₂, temperature, urine output)
- Pain management and mobilization
- Vigilance for:
- Respiratory: hypoxia, atelectasis, pneumonia
- Cardiovascular: arrhythmias, MI, DVT/PE
- Surgical site: wound infection, dehiscence, anastomotic leak
- Fluid/electrolytes: fluid overload vs. hypovolemia
- Cognitive: postoperative delirium (especially elderly)
Hospital mortality increases substantially with age and comorbidities — e.g., combined CHF + renal failure + abdominal surgery in patients >70 years carries a 37% elective / 76% emergency mortality rate (Mulholland and Greenfield's Surgery, 7e).
PART III — MODERN TECHNOLOGIES IN SURGERY
1. Minimally Invasive Surgery (MIS)
Minimally invasive techniques — laparoscopy and robotics — are now the standard of care for many procedures. Key advantages over open surgery:
- Smaller incisions with decreased postoperative pain
- Decreased blood loss
- Shorter length of hospital stay
- Faster overall recovery
- Lower surgical site infection rates
2. History of Robotic Surgery
The concept originated from NASA Ames Research Center / Stanford University research in the mid-1980s, integrating virtual reality with robotics. DARPA and the US Department of Defense provided critical early funding, motivated by the goal of treating wounded soldiers remotely.
Three system types:
- Active: Works autonomously under surgeon control with preprogrammed tasks (e.g., PROBOT, 1988 — first robotic system used in humans, for TURP)
- Semiactive: Surgeon-driven elements completing preprogrammed tasks
- Master-slave: No autonomous elements; translates surgeon's hand movements to instruments — the dominant modern system
Key milestones:
- 1993: AESOP — first FDA-approved robotic arm (DARPA-funded)
- 2000: da Vinci Surgical System (Intuitive Surgical, Inc.) received FDA approval
- 2002: First transoceanic telesurgery — robotic cholecystectomy across the Atlantic
- 2003: Intuitive Surgical acquired Computer Motion, dominating the field
— Sabiston Textbook of Surgery, 21e
3. Da Vinci System Evolution
| Generation | Year | Key Advances |
|---|---|---|
| Original da Vinci | 2000 | 3-arm system |
| 4-arm system | 2002 | Reduced need for assistant, improved exposure |
| da Vinci S | 2006 | Greater range of motion, longer instruments, multi-quadrant operation |
| da Vinci Si | 2009 | HD visualization, dual console for training |
| da Vinci Xi | 2014 | Overhead architecture, slimmer arms, guided targeting, single-dock multi-quadrant surgery |
| da Vinci X | 2017 | Lower-cost entry-point system |
| da Vinci SP | Recent | Single-port — camera + 3 instruments through one port |
4. Advantages of Robotic Surgery Over Conventional Laparoscopy
| Feature | Conventional Laparoscopy | Robotic Surgery |
|---|---|---|
| Degrees of freedom | Limited (rigid instruments) | 7 degrees of freedom (EndoWrist technology) |
| Visualization | 2D or basic 3D | High-definition 3D, 10× magnification |
| Surgeon ergonomics | Suboptimal (fatigue) | Ergonomic seated console, reduced fatigue |
| Tremor | Present | Electronically filtered |
| Training | Steep learning curve | Shorter learning curve via simulation |
| Cost | Lower | Higher (platform + consumables) |
| Haptic feedback | Present | Limited/absent |
Robotic surgery provides surgeons with enhanced visualization, augmented dexterity and precision, sophisticated articulating instruments, reduced fatigue, and improved ergonomics. — Sabiston Textbook of Surgery, 21e
5. Applications in General Surgery
Robotic surgery is now applied broadly across general surgery:
- Hernia repair (inguinal, ventral, hiatal)
- Colorectal surgery (especially pelvic — lower rectal dissection)
- Hepatobiliary/pancreatic: Robotic pancreaticoduodenectomy (RPD), liver resection
- Bariatric surgery: Sleeve gastrectomy, Roux-en-Y gastric bypass
- Endocrine: Thyroid and parathyroid, adrenalectomy
- Gynecology: Hysterectomy, staging for endometrial cancer (especially morbidly obese patients)
- Urology: Robotic-assisted radical prostatectomy (RARP) is now the global standard
6. Robotic Surgery vs. Laparoscopy — Limitations
- Longer operative times (especially early in the learning curve)
- Higher cost of the platform and consumables
- No haptic feedback (loss of tactile sensation)
- Limited access to systems in lower-resource settings
- Dependency: system malfunction can necessitate emergency conversion
- Superiority over laparoscopy in outcomes has been difficult to demonstrate uniformly
7. Training in Robotic Surgery
Modern training follows a graduated curriculum:
- Virtual simulation: Console-attached simulators with games and drills at varying complexity; web-based performance tracking
- Inanimate simulation: Robotic arm drills, suturing and knot-tying exercises, anastomotic models with lifelike biotissue
- Animate/cadaveric simulation: Animal models for realistic tissue handling
- Video review: Easy recording capability supports procedure video libraries for self-analysis
- Dual console: Attending surgeon can seamlessly take control or assist robotically during trainee cases
Comprehensive training at the fellow level results in a smoother transition to high-volume robotic practice; early outcomes for RPD are equivalent to or superior to established benchmarks post–learning curve. — Sabiston Textbook of Surgery, 21e
8. Other Modern Surgical Technologies
| Technology | Description |
|---|---|
| Endoscopy | Flexible and rigid endoscopes for diagnostic and therapeutic GI, airway, and joint procedures |
| Fluorescence imaging | Near-infrared (NIR) / indocyanine green (ICG) for perfusion assessment, bile duct visualization, sentinel lymph node mapping |
| 3D printing | Patient-specific anatomic models for preoperative planning; custom implants |
| Augmented/Virtual Reality (AR/VR) | Surgical planning, intraoperative navigation, resident training |
| Artificial Intelligence (AI) | Intraoperative image analysis, tissue identification, anastomotic leak prediction |
| NOTES | Natural orifice transluminal endoscopic surgery (scarless procedures) |
| SILS/LESS | Single-incision laparoscopic surgery (cosmetic advantage, reduced trauma) |
| Image-guided surgery | Intraoperative CT/MRI, ultrasound, fluoroscopy for navigation |
| Enhanced Recovery After Surgery (ERAS) | Multimodal protocols integrating preoperative optimization, MIS techniques, and structured postoperative monitoring to reduce LOS and complications |
Summary Table
| Domain | Key Points |
|---|---|
| Examination | History + physical = foundation; ASA classification; functional capacity (METs); targeted testing |
| Supervision | Risk-stratified perioperative monitoring; RCRI/NSQIP for cardiac risk; ICU for high-risk postoperative |
| Modern Technology | Robotic (da Vinci), laparoscopy, endoscopy, AI, ICG fluorescence, ERAS |
Sources:
- Goldman-Cecil Medicine, 26th ed. — Preoperative evaluation
- Mulholland and Greenfield's Surgery, 7e — Preoperative assessment, ASA classification, mortality data
- Sabiston Textbook of Surgery, 21e — Robotic surgery history, da Vinci evolution, training
- Fishman's Pulmonary Diseases and Disorders — Preoperative pulmonary evaluation
More details
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.