Classify Corticosteroids. Describe the MoA, Pharmacological Actions, Adverse Effects, Therapeutic Uses, Drug Interactions & Contraindications for Prednisolone (
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
This is extremely comprehensive. I now have extensive data from Goodman & Gilman's. Let me compile the full answer from all the content retrieved.
Corticosteroids: Classification, and Prednisolone - Complete Pharmacology
(Source: Goodman & Gilman's The Pharmacological Basis of Therapeutics, 14th Ed.)
CLASSIFICATION OF CORTICOSTEROIDS
Corticosteroids are steroid hormones produced by the adrenal cortex. They are classified into two major groups based on their predominant physiological actions:
1. Glucocorticoids (21-carbon pregane structure)
Regulate carbohydrate metabolism and have anti-inflammatory/immunosuppressive actions.
A. Natural (Endogenous):
- Cortisol (hydrocortisone) - the main physiological glucocorticoid
- Cortisone (inactive prodrug form, converted to cortisol by 11β-HSD1)
- Corticosterone
B. Synthetic - Short-acting (8-12 h):
| Drug | Relative Glucocorticoid Potency | Relative Mineralocorticoid Potency |
|---|---|---|
| Cortisol (hydrocortisone) | 1 | 1 |
| Cortisone | 0.8 | 0.8 |
C. Synthetic - Intermediate-acting (18-36 h):
| Drug | GC Potency | MC Potency |
|---|---|---|
| Prednisone | 4 | 0.3 |
| Prednisolone | 4 | 0.3 |
| Methylprednisolone | 5 | 0 |
| Triamcinolone | 5 | 0 |
D. Synthetic - Long-acting (36-54 h):
| Drug | GC Potency | MC Potency |
|---|---|---|
| Dexamethasone | 25-30 | 0 |
| Betamethasone | 25-30 | 0 |
2. Mineralocorticoids
Regulate electrolyte and water balance.
- Natural: Aldosterone (main), Deoxycorticosterone
- Synthetic: Fludrocortisone (9α-fluorocortisol) - the prototype synthetic mineralocorticoid
3. Adrenal Androgens
- DHEA, DHEAS, Androstenedione (19-carbon androstane structure)
PREDNISOLONE
Prednisolone is the active form of prednisone (prednisone is an inactive 11-keto prodrug converted to prednisolone by 11β-HSD1 in the liver). It is the most commonly used intermediate-acting synthetic glucocorticoid.
MECHANISM OF ACTION (MoA)
Genomic (Classical) Mechanism
- Prednisolone crosses the cell membrane due to its lipophilic nature
- Binds to the cytoplasmic glucocorticoid receptor (GR-α), causing dissociation of heat shock proteins (hsp90, hsp70)
- The steroid-receptor complex undergoes conformational change and translocates to the nucleus
- Binds to glucocorticoid response elements (GREs) in DNA to:
- Transactivation: Upregulate anti-inflammatory proteins (lipocortin-1/annexin-1, IL-10, IκB)
- Transrepression: Downregulate pro-inflammatory genes (IL-1, IL-2, IL-6, TNF-α, COX-2, iNOS) by inhibiting transcription factors AP-1 and NF-κB
Non-Genomic Mechanisms
- Rapid effects (seconds to minutes) mediated via membrane-bound receptors and second messengers
- Inhibition of arachidonic acid release (via lipocortin-1 inhibiting phospholipase A2)
- Modulation of ion channels and signal transduction cascades
Key Anti-inflammatory Steps
- Induces synthesis of lipocortin (annexin-1) → inhibits phospholipase A2 → reduces arachidonic acid → reduces both prostaglandins/thromboxanes (COX pathway) AND leukotrienes (LOX pathway)
- Inhibits NF-κB activation → blocks transcription of multiple cytokines
- Reduces vascular permeability (vasoconstriction of small vessels)
PHARMACOLOGICAL ACTIONS
1. Anti-inflammatory Effects
- Stabilizes lysosomal membranes, reducing release of proteolytic enzymes
- Reduces capillary permeability and vasodilation
- Inhibits migration of leukocytes (especially neutrophils, monocytes) to site of inflammation
- Suppresses production of IL-1, IL-2, IL-6, TNF-α, IFN-γ
- Inhibits COX-2 expression and reduces prostaglandin synthesis
- Decreases fibroblast proliferation → reduced fibrin deposition and scar formation
2. Immunosuppressive Effects
- Redistributes lymphocytes from blood to lymphoid tissue (lymphopenia)
- Inhibits T-cell proliferation and cytokine production
- Reduces antibody production (high doses)
- Impairs cell-mediated immunity more than humoral immunity
- Causes involution of lymphoid tissue (thymus, spleen, lymph nodes)
- Neutrophilia (release from bone marrow + reduced margination) with lymphopenia, monocytopenia, eosinopenia
3. Metabolic Effects
Carbohydrate Metabolism:
- Stimulates gluconeogenesis in liver
- Decreases peripheral glucose uptake and utilization (anti-insulin effect)
- Net effect: hyperglycemia (steroid diabetes)
Protein Metabolism:
- Increases protein catabolism (muscle, skin, bone)
- Increased nitrogen excretion in urine (negative nitrogen balance)
- Reduced protein synthesis in most tissues
Fat Metabolism:
- Lipolysis in extremities
- Redistribution of fat to face, neck, trunk ("buffalo hump," "moon face," "centripetal obesity")
- Stimulates appetite
Mineral/Electrolyte (Mineralocorticoid) Effects (mild for prednisolone):
- Sodium and water retention
- Potassium and hydrogen ion excretion
- Hypokalemic alkalosis (less pronounced than hydrocortisone)
4. Cardiovascular Effects
- Maintains cardiac contractility and vascular tone
- Sensitizes vessels to catecholamines (permissive effect)
- May cause hypertension (Na retention + sensitization to vasopressors)
5. Musculoskeletal Effects
- Inhibits osteoblast activity → reduces bone formation
- Increases osteoclast activity → bone resorption
- Reduces calcium absorption from gut and increases renal calcium excretion → osteoporosis
6. CNS Effects
- Euphoria, mood elevation at low doses
- Psychosis, depression at high doses
- Increases intracranial pressure (pseudotumor cerebri on withdrawal)
- Lowers seizure threshold
7. Endocrine Effects
- Suppresses HPA axis (hypothalamic-pituitary-adrenal) via negative feedback
- Reduces TSH and GH secretion
- Reduces gonadotropin levels
8. Hematologic Effects
- Neutrophilia, lymphopenia, eosinopenia, monocytopenia
- Thrombocytosis (high doses)
- Increased RBC production
9. Ophthalmic Effects
- Raises intraocular pressure (glaucoma)
- Posterior subcapsular cataracts with prolonged use
10. GI Effects
- Increases gastric acid secretion
- Reduces protective mucus production → peptic ulceration
ADVERSE EFFECTS
Metabolic/Endocrine
- Cushing's syndrome (iatrogenic): moon face, buffalo hump, centripetal obesity, striae
- Diabetes mellitus / hyperglycemia (steroid-induced)
- Hyperlipidemia
- Growth retardation in children
- Amenorrhea and menstrual irregularities
Musculoskeletal
- Osteoporosis (most serious long-term effect)
- Avascular necrosis (osteonecrosis) of femoral head
- Myopathy (proximal muscle wasting, especially Type II fiber atrophy)
Cardiovascular
- Hypertension (sodium and water retention)
- Atherosclerosis acceleration
- Hypokalemia (cardiac arrhythmias)
Gastrointestinal
- Peptic ulcer disease (especially combined with NSAIDs)
- Pancreatitis
- Gastric hemorrhage
Immunological / Infection Risk
- Increased susceptibility to infections (bacterial, fungal, viral - TB reactivation)
- Masks signs/symptoms of infection
- Candidiasis (especially oral)
Ophthalmic
- Posterior subcapsular cataracts (dose-dependent, chronic use)
- Glaucoma (raised IOP)
- Exacerbation of viral keratitis (herpes simplex)
CNS / Psychiatric
- Steroid psychosis (euphoria, mania, depression, frank psychosis)
- Insomnia
- Pseudotumor cerebri (benign intracranial hypertension) on withdrawal
Dermatologic
- Skin atrophy, thinning, easy bruising
- Acne, hirsutism
- Impaired wound healing
- Striae
HPA Axis Suppression
- Adrenal insufficiency on abrupt withdrawal (Addisonian crisis)
- Requires gradual tapering after prolonged therapy
- Cushingoid features from exogenous excess
Hematologic
- Thromboembolism risk
- Leukocytosis
THERAPEUTIC USES
Endocrine/Replacement Therapy
- Primary adrenal insufficiency (Addison's disease) - physiological replacement (with fludrocortisone for mineralocorticoid)
- Secondary adrenal insufficiency
- Congenital adrenal hyperplasia (CAH) - suppresses excess ACTH
- Adrenal crisis (IV hydrocortisone preferred acutely)
Rheumatologic / Connective Tissue Diseases
- Rheumatoid arthritis (bridge therapy, DMARDs-sparing)
- Systemic lupus erythematosus (SLE) - especially nephritis, serositis
- Polymyalgia rheumatica / giant cell arteritis
- Dermatomyositis / polymyositis
- Vasculitis (ANCA-associated)
- Mixed connective tissue disease, scleroderma
Respiratory
- Severe bronchial asthma (oral prednisolone burst for acute exacerbations)
- COPD exacerbations
- Sarcoidosis
- Eosinophilic pneumonia
- Interstitial lung disease (IPF with inflammatory component)
- Aspiration pneumonitis
Renal
- Nephrotic syndrome (especially minimal change disease - first line)
- Lupus nephritis
- Rapidly progressive glomerulonephritis (RPGN)
Gastrointestinal
- Inflammatory bowel disease (Crohn's disease, ulcerative colitis - induction of remission)
- Autoimmune hepatitis
- Alcoholic hepatitis (severe, Maddrey >32)
Neurological
- Multiple sclerosis relapses (high-dose IV methylprednisolone preferred, but oral prednisolone used)
- Bell's palsy (facial nerve palsy - early treatment)
- Myasthenia gravis
- Cerebral edema (dexamethasone preferred for CNS tumors)
Hematology/Oncology
- Immune thrombocytopenic purpura (ITP)
- Autoimmune hemolytic anemia (AIHA)
- Lymphomas and leukemias (CLL, ALL - part of chemotherapy regimens)
- Multiple myeloma
Dermatology
- Pemphigus vulgaris
- Bullous pemphigoid
- Severe atopic dermatitis, urticaria
- Lichen planus
Transplantation
- Prevention and treatment of organ rejection (in combination with other immunosuppressants)
Allergic Conditions
- Severe anaphylaxis (after epinephrine)
- Angioedema
- Serum sickness
- Severe contact dermatitis
Other
- Preterm labor (betamethasone/dexamethasone preferred for fetal lung maturity)
- Infectious mononucleosis (severe, with airway compromise)
- Tuberculosis (with anti-TB drugs - for pericarditis, meningitis, severe pulmonary TB)
DRUG INTERACTIONS
| Interacting Drug/Class | Type of Interaction | Clinical Consequence |
|---|---|---|
| NSAIDs (aspirin, ibuprofen) | Additive GI toxicity | Increased risk of peptic ulcer, GI bleeding |
| Anticoagulants (warfarin) | Altered anticoagulant effect | Variable; may increase or decrease INR - monitor closely |
| Antidiabetic drugs (insulin, OHAs) | Antagonism of hypoglycemic effect | Hyperglycemia; dose adjustment needed |
| Antihypertensives | Antagonism of antihypertensive effect | Increased blood pressure (Na/water retention) |
| CYP3A4 inducers (rifampicin, phenytoin, carbamazepine, phenobarbital) | Increased prednisolone metabolism | Reduced prednisolone levels; therapeutic failure |
| CYP3A4 inhibitors (ketoconazole, itraconazole, erythromycin, ritonavir) | Decreased prednisolone metabolism | Increased prednisolone exposure; increased toxicity |
| Diuretics (thiazides, loop diuretics) | Additive hypokalemia | Severe hypokalemia, arrhythmias |
| Amphotericin B | Additive hypokalemia | Severe hypokalemia |
| Live vaccines | Immunosuppression | Disseminated infection from live vaccine; avoid |
| Cyclosporine / Tacrolimus | Mutual inhibition of CYP3A4 | Increased levels of both drugs; nephrotoxicity, steroid toxicity |
| Mifepristone | GR antagonist | Blocks glucocorticoid receptor effect |
| Antacids (Mg/Al hydroxide) | Reduced absorption | Reduced prednisolone bioavailability |
| Oral contraceptives / Estrogens | Increase CBG, reduce metabolism | Increased prednisolone half-life and effect |
| Neuromuscular blocking agents | Additive myopathy | Prolonged neuromuscular blockade |
| Somatropin (GH) | Antagonism of GH effect | Reduced growth in children |
CONTRAINDICATIONS
Absolute Contraindications
- Systemic fungal infections (e.g., disseminated candidiasis, aspergillosis)
- Active, untreated tuberculosis (without concurrent anti-TB therapy)
- Known hypersensitivity to prednisolone or any component
- Administration of live vaccines during immunosuppressive doses
Relative Contraindications (Caution/Risk-Benefit Assessment Required)
- Peptic ulcer disease (use with PPI cover if unavoidable)
- Diabetes mellitus (worsens glycemic control)
- Hypertension (worsens BP; monitor)
- Osteoporosis (add bisphosphonate prophylaxis)
- Psychiatric disorders / psychosis (may precipitate steroid psychosis)
- Congestive heart failure / fluid retention states (mineralocorticoid effects)
- Infections (viral, bacterial, parasitic) - may mask signs; treat infection first
- Herpes simplex keratitis (may cause corneal perforation - topically contraindicated)
- Pregnancy (category C; crosses placenta; risk of cleft palate - use lowest effective dose)
- Breastfeeding (excreted in breast milk - monitor infant)
- Cushing's syndrome (exogenous or endogenous)
- Glaucoma (raises IOP)
- Myasthenia gravis (initial worsening possible)
- Hypothyroidism (altered corticosteroid metabolism)
- Severe renal/hepatic impairment (altered pharmacokinetics)
QUICK REFERENCE SUMMARY
| Parameter | Prednisolone |
|---|---|
| Class | Intermediate-acting synthetic glucocorticoid |
| Glucocorticoid potency | 4x cortisol |
| Mineralocorticoid potency | 0.3x cortisol |
| Equivalent dose | 5 mg = 20 mg cortisol |
| Plasma t½ | ~3.5 hours |
| Biological t½ | 18-36 hours |
| Route | Oral (active form; unlike prednisone which needs hepatic conversion) |
| Protein binding | ~90% (CBG + albumin) |
Key distinction: Prednisolone is the active form; Prednisone is the inactive 11-keto prodrug activated by hepatic 11β-HSD1. This is why prednisolone (not prednisone) is preferred in liver disease.
Sources: Goodman & Gilman's The Pharmacological Basis of Therapeutics, 14th Ed.; Goodman & Gilman's The Pharmacological Basis of Therapeutics - Chapter 50 (Adrenocortical Steroids)
steroid hornones
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
I now have rich textbook content and diagrams to build a comprehensive answer on steroid hormones.
Steroid Hormones
(Sources: Lippincott's Illustrated Reviews: Biochemistry 8th Ed.; Medical Physiology; Berek & Novak's Gynecology; Goodman & Gilman's)
Definition & General Properties
Steroid hormones are lipid-soluble signaling molecules derived from cholesterol. Because of their hydrophobic nature, they:
- Freely diffuse across plasma membranes
- Must travel in blood bound to carrier proteins (albumin, specific binding globulins)
- Act via intracellular (nuclear) receptors to regulate gene transcription
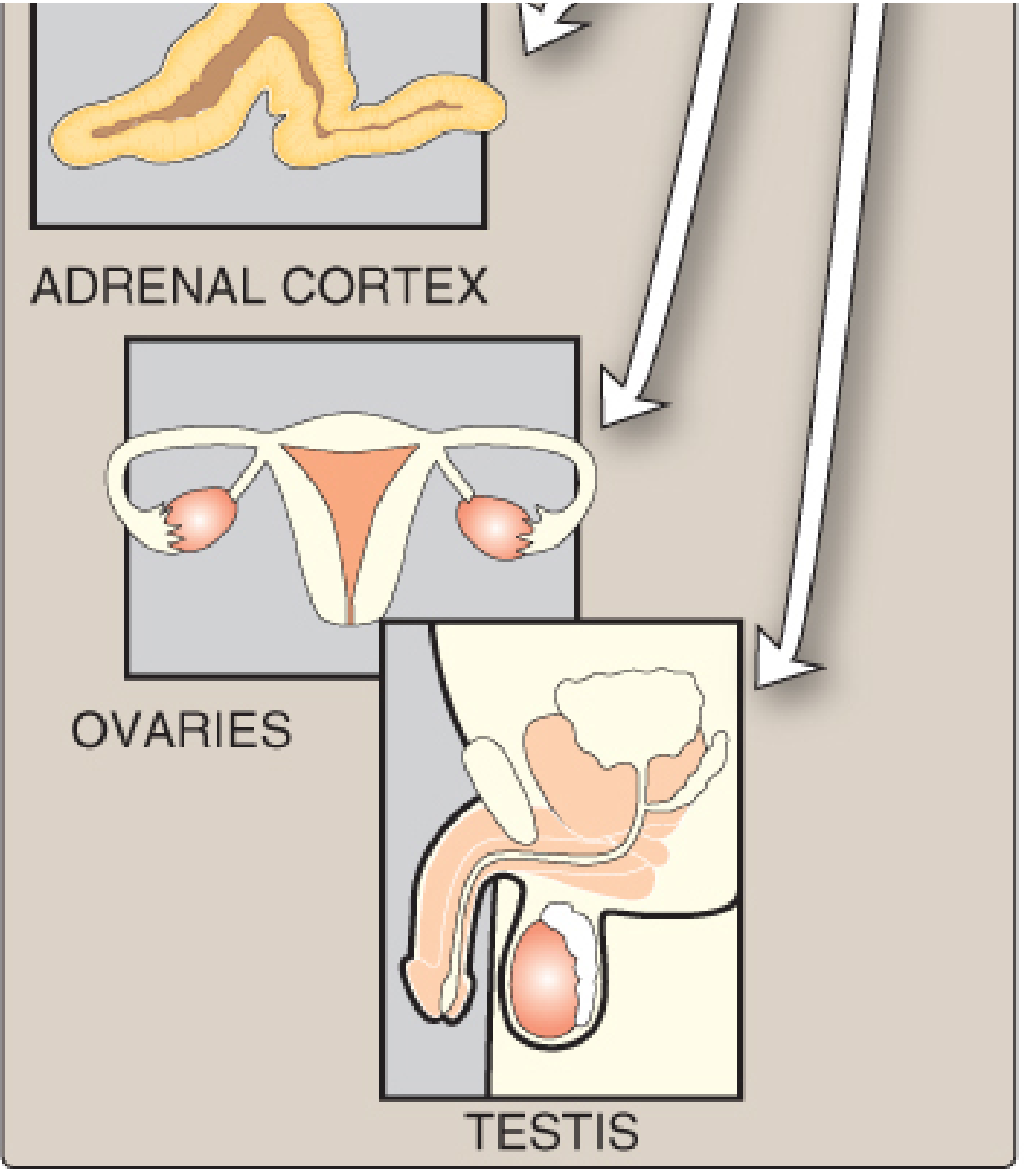
- Are synthesized in the adrenal cortex, gonads (testes and ovaries), and placenta
Classification
Steroid hormones are classified into 5 major classes based on their carbon number, site of synthesis, and physiological action:
| Class | Carbon Number | Main Example | Site of Synthesis | Receptor |
|---|---|---|---|---|
| Glucocorticoids | 21 C (pregnane) | Cortisol | Adrenal cortex (zona fasciculata) | GR (glucocorticoid receptor) |
| Mineralocorticoids | 21 C (pregnane) | Aldosterone | Adrenal cortex (zona glomerulosa) | MR (mineralocorticoid receptor) |
| Progestogens (Progestins) | 21 C | Progesterone | Ovary (corpus luteum), Placenta | PR |
| Androgens | 19 C (androstane) | Testosterone, DHEA | Testes (Leydig cells), Adrenal cortex (zona reticularis) | AR (androgen receptor) |
| Estrogens | 18 C (estrane) | Estradiol (E2) | Ovaries, Placenta, peripheral aromatization | ER-α, ER-β |
Note: Vitamin D (calcitriol) and thyroid hormones are not steroids structurally but share the same nuclear receptor superfamily mechanism and are sometimes classified alongside steroid hormones.
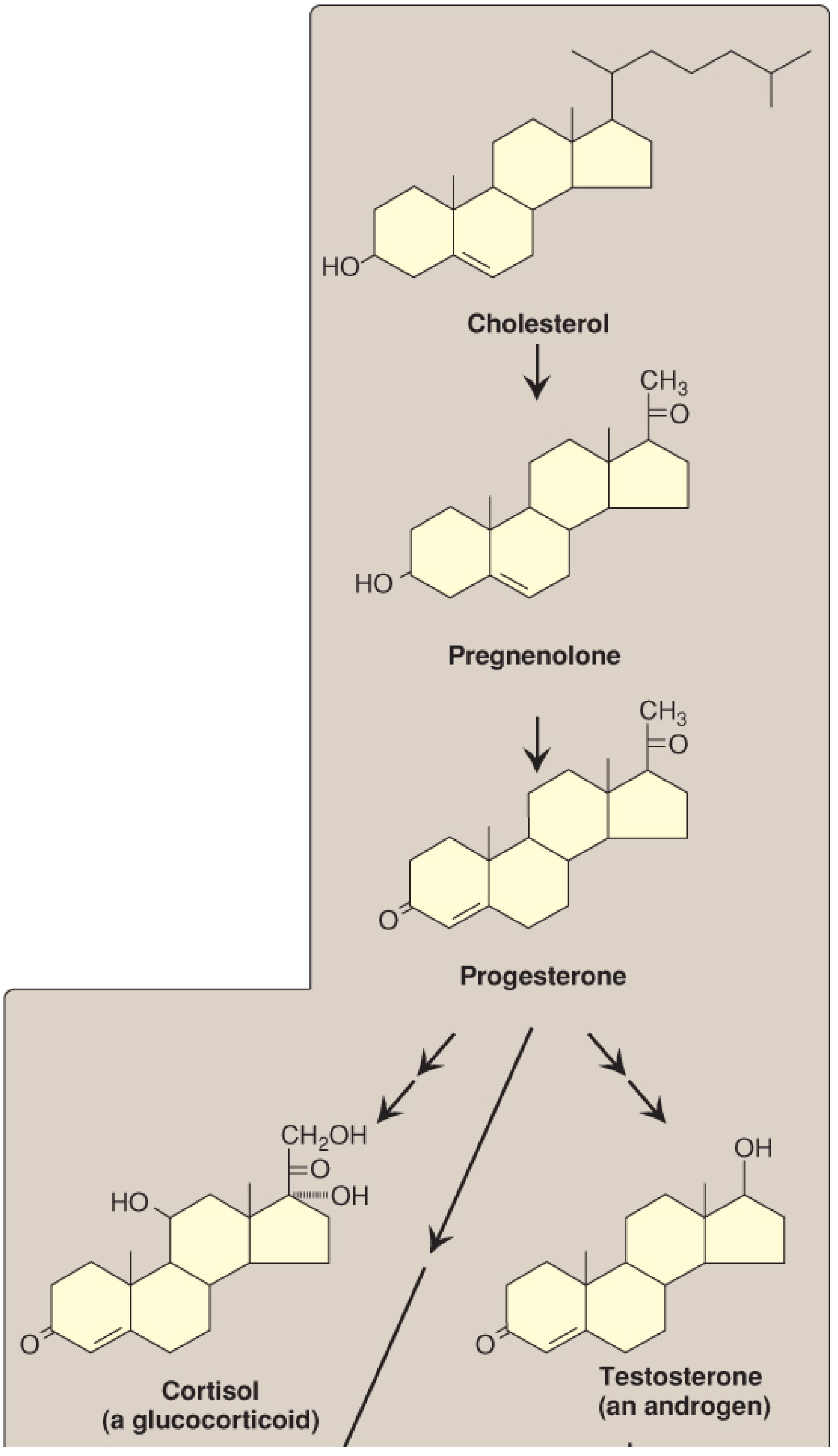
Biosynthesis - From Cholesterol to Steroid Hormones
All steroid hormones are synthesized from cholesterol through a cascade of enzymatic reactions. The key pathway:
Step-by-Step Pathway
Rate-limiting step: Cholesterol → Pregnenolone
- Enzyme: Desmolase (cholesterol side-chain cleavage enzyme, CYP11A / P450scc)
- Location: Inner mitochondrial membrane
- Cofactors: NADPH + O₂
- Regulated by: StAR protein (steroidogenic acute regulatory protein) - transports cholesterol from outer to inner mitochondrial membrane; ACTH activates via cAMP → PKA → StAR
Full Biosynthesis Pathway
Cholesterol (27C)
↓ Desmolase (CYP11A) - rate limiting
Pregnenolone (21C)
↓ 3β-Hydroxysteroid dehydrogenase (3β-HSD)
Progesterone (21C)
↓ ↓
[via 17α-Hydroxylase] [via 21α-Hydroxylase]
17α-Hydroxyprogesterone 11-Deoxycorticosterone
↓ 17,20-Lyase ↓ 11β-Hydroxylase (CYP11B1)
Androstenedione (19C) Corticosterone
↓ 17β-HSD ↓ Aldosterone synthase (CYP11B2)
Testosterone (19C) ALDOSTERONE
↓ Aromatase (CYP19)
Estradiol (18C)
Also:
17α-Hydroxyprogesterone → 11-Deoxycortisol → CORTISOL (via 11β-Hydroxylase)
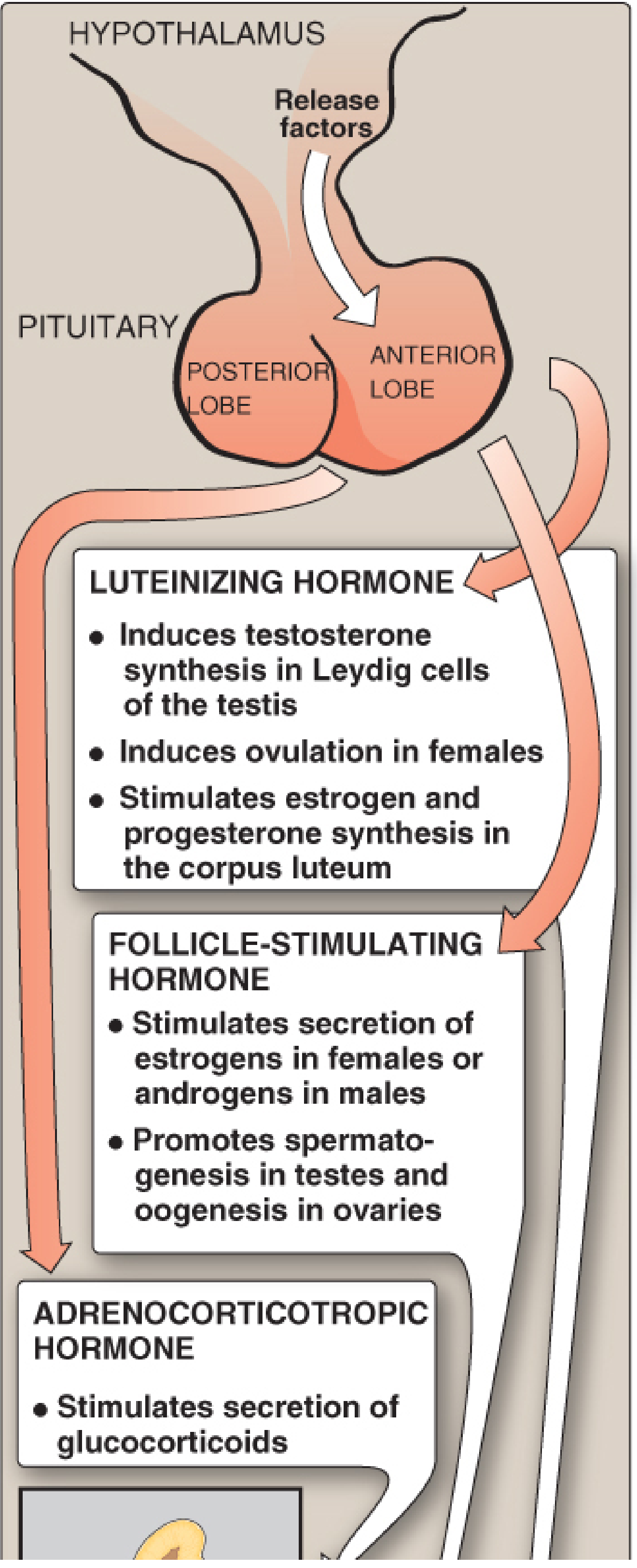
Regulation of Secretion
The hypothalamic-pituitary axis controls steroid hormone secretion:
1. Glucocorticoids (Cortisol)
- CRH (hypothalamus) → ACTH (anterior pituitary) → Cortisol (zona fasciculata)
- ACTH acts via cAMP → PKA pathway (Gs-coupled receptor)
- Cortisol exerts negative feedback on both hypothalamus and pituitary
- Diurnal rhythm: peak in early morning, nadir at midnight
2. Mineralocorticoids (Aldosterone)
- Primary regulators: Low Na⁺/K⁺ ratio and Angiotensin II (from RAAS)
- Ang II acts via PLC → IP₃/DAG pathway (not cAMP)
- Also stimulated by: hyperkalemia, ACTH (minor role)
3. Sex Steroids
- GnRH (hypothalamus) → LH + FSH (anterior pituitary) → Gonads
- LH acts via cAMP → PKA (Gs-coupled)
- LH → Testosterone (Leydig cells), Estrogen + Progesterone (corpus luteum)
- FSH → Spermatogenesis, follicular growth, estrogen secretion
Transport in Blood
Because steroids are lipophilic, they require carrier proteins:
| Steroid | Carrier Protein | % Bound |
|---|---|---|
| Cortisol | Corticosteroid-binding globulin (CBG/Transcortin) | >95% |
| Aldosterone | Albumin (loosely) | ~60% |
| Testosterone | Sex hormone-binding globulin (SHBG) | ~98% |
| Estradiol | SHBG | ~98% |
| Progesterone | CBG, albumin | ~98% |
- Only the free (unbound) fraction is biologically active
- Carrier proteins extend hormone half-life and buffer fluctuations
- Liver disease, pregnancy, and drugs can alter binding globulin levels
Mechanism of Action
Steroid hormones act primarily via nuclear receptors (genomic mechanism):
Genomic Mechanism (Primary)
- Lipophilic steroid diffuses freely across the cell membrane
- Binds to specific cytosolic or nuclear receptor (part of the nuclear receptor superfamily)
- Hormone-receptor complex undergoes conformational change - DNA-binding domain is uncovered (zinc finger motif)
- Complex dimerizes and translocates to nucleus
- Binds to specific Hormone Response Elements (HREs) in DNA promoter/enhancer regions
- Recruits coactivators or corepressors to either:
- Activate (transactivation) gene transcription → new protein synthesis
- Suppress (transrepression) gene transcription → reduced protein synthesis
- Effects are delayed (hours) due to the time needed for new mRNA and protein synthesis
Non-Genomic Mechanism (Secondary - Rapid)
- Membrane-bound receptors activate second messengers (cAMP, IP₃, Ca²⁺)
- Effects within seconds to minutes
- Important for rapid responses (e.g., aldosterone's rapid effect on renal tubular ion channels)
Nuclear Receptor Superfamily
All steroid hormone receptors share a common domain structure:
- A/B domain: N-terminal, activation function-1 (AF-1) - ligand-independent activation
- C domain: DNA-binding domain (DBD) - two zinc fingers
- D domain: Hinge region
- E domain: Ligand-binding domain (LBD) - binds hormone; activation function-2 (AF-2)
- F domain: C-terminal (variable)
The same superfamily includes thyroid hormone receptor, retinoic acid receptor, and vitamin D receptor.
Individual Classes - Actions
1. Glucocorticoids (Cortisol)
| System | Effect |
|---|---|
| Carbohydrate | ↑ Gluconeogenesis, ↓ peripheral glucose uptake → hyperglycemia |
| Protein | ↑ Catabolism, negative nitrogen balance |
| Fat | Lipolysis in extremities, fat redistribution centrally |
| Immune/Inflammation | Anti-inflammatory, immunosuppressive |
| Bone | ↓ Osteoblast activity, ↓ Ca²⁺ absorption → osteoporosis |
| CVS | Permissive effect on catecholamines, maintains BP |
| Stress response | "Fight or flight" metabolic support |
2. Mineralocorticoids (Aldosterone)
| System | Effect |
|---|---|
| Kidney (principal cells) | ↑ Na⁺ reabsorption (collecting duct), ↑ K⁺ and H⁺ excretion |
| Blood | Hypertension, hypokalemia, metabolic alkalosis |
| Regulation | RAAS-driven; maintains ECF volume and BP |
3. Androgens (Testosterone, DHEA)
| Phase | Effect |
|---|---|
| Fetal | Male sexual differentiation |
| Puberty | Secondary sexual characteristics, spermatogenesis, libido |
| Adult | Anabolic effects (muscle, bone), erythropoiesis, sebaceous gland activity |
| Adrenal androgens | DHEA is a precursor for peripheral sex steroid synthesis |
4. Estrogens (Estradiol)
| System | Effect |
|---|---|
| Reproductive | Female sexual development, endometrial proliferation, ovulation |
| Bone | Protective against bone loss (↑ osteoblast activity, ↓ resorption) |
| Cardiovascular | Protective (pre-menopause) |
| Breast | Ductal growth |
| CNS | Mood regulation, neuroprotection |
5. Progestogens (Progesterone)
| System | Effect |
|---|---|
| Uterus | Prepares endometrium for implantation, maintains pregnancy |
| Breast | Lobular-alveolar development |
| Temperature | Raises basal body temperature (thermogenic) |
| CNS | Sedative, anxiolytic (via allopregnanolone-GABA-A) |
Metabolism & Excretion
- Metabolized primarily in the liver by:
- Reduction of unsaturated C=C bonds
- Hydroxylation (additional -OH groups)
- Products conjugated with glucuronic acid or sulfate (by SULT, UGT enzymes) → water-soluble
- Conjugated metabolites excreted in urine and feces (no carrier protein needed)
- Example: 11β-HSD2 in kidney inactivates cortisol → cortisone (protects mineralocorticoid receptor from cortisol)
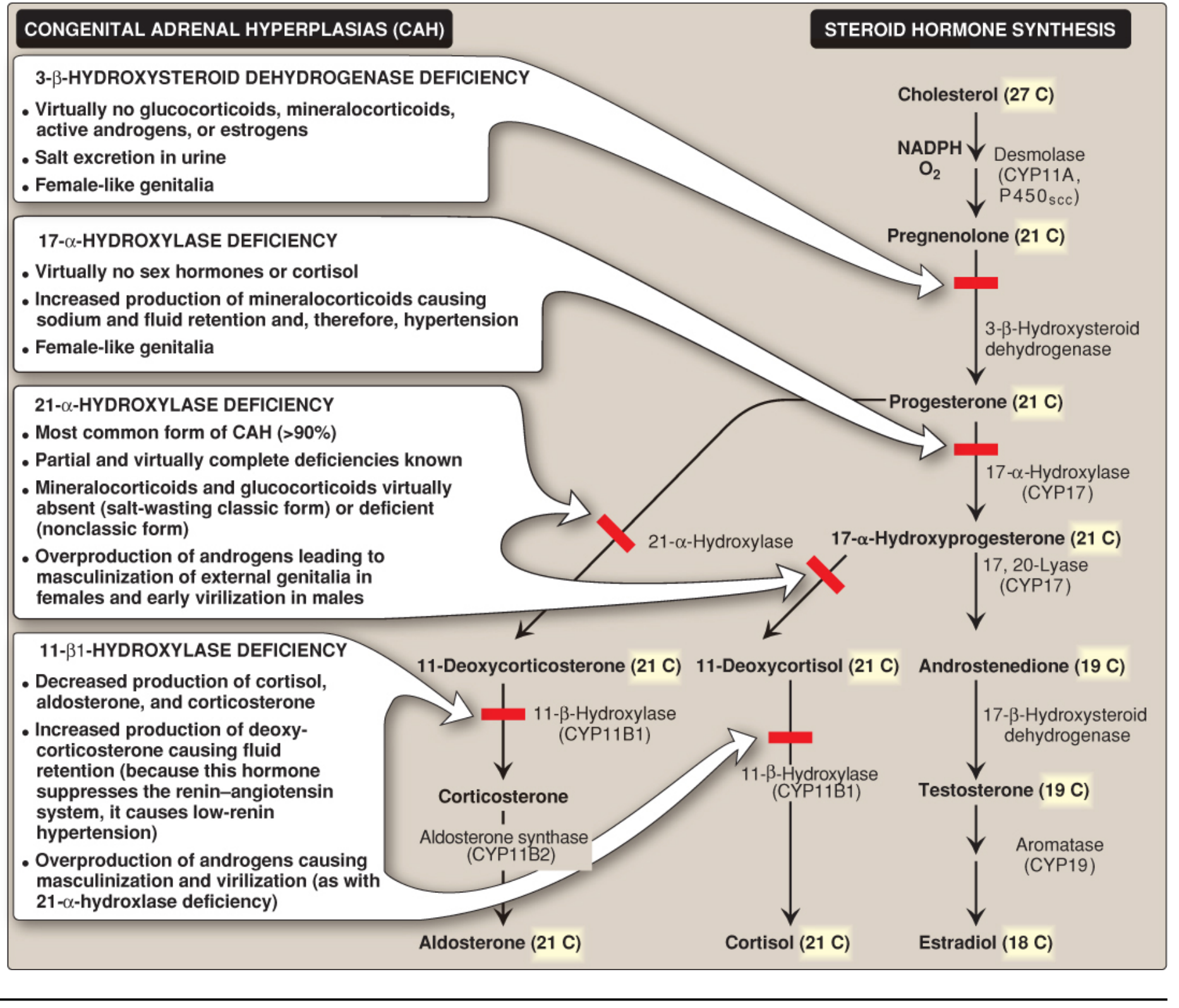
Key Enzyme Deficiencies (Congenital Adrenal Hyperplasia - CAH)
As shown in the biosynthesis pathway diagram above:
| Enzyme Deficiency | Frequency | Key Features |
|---|---|---|
| 21α-Hydroxylase | >90% of CAH | No cortisol/aldosterone; ↑ androgens → female virilization, salt-wasting |
| 11β-Hydroxylase | ~5% | ↓ Cortisol; ↑ 11-deoxycorticosterone → low-renin hypertension |
| 17α-Hydroxylase | Rare | No sex hormones or cortisol; ↑ mineralocorticoids → hypertension |
| 3β-HSD | Rare | No glucocorticoids, mineralocorticoids, androgens, or estrogens |
Summary Comparison Table
| Feature | Glucocorticoids | Mineralocorticoids | Androgens | Estrogens | Progestins |
|---|---|---|---|---|---|
| Precursor | Cholesterol | Cholesterol | Cholesterol | Testosterone | Progesterone |
| Primary organ | Adrenal (ZF) | Adrenal (ZG) | Testes/Adrenal (ZR) | Ovaries | Corpus luteum |
| Carbon number | 21 | 21 | 19 | 18 | 21 |
| Receptor | GR | MR | AR | ERα/β | PR |
| Key action | Anti-inflammatory, metabolism | Na/K balance | Masculinization, anabolic | Feminization, bone protection | Implantation, thermogenesis |
| Binding protein | CBG (transcortin) | Albumin | SHBG | SHBG | CBG |
(Sources: Lippincott's Illustrated Reviews: Biochemistry, 8th Ed., pp. 661-669; Medical Physiology; Berek & Novak's Gynecology; Goodman & Gilman's Pharmacological Basis of Therapeutics, 14th Ed.)
This is a shared conversation. Sign in to Orris to start your own chat.