Bronchogenic carcinoma imaging radiology
Reading File
Finding Sources
Finding Sources
Searching PubMed
"bronchogenic carcinoma" AND "imaging" AND "radiology"
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive material. Let me compile the full answer.
Bronchogenic Carcinoma - Imaging & Radiology
Source: Grainger & Allison's Diagnostic Radiology
Overview of Imaging Approach
Thoracic imaging features of bronchial carcinoma are discussed under three headings:
- Peripheral tumours
- Central tumours (arising in a large bronchus at or close to the hilum)
- Staging intrathoracic spread
The routine imaging sequence is: Chest radiograph → CT → 18F-FDG PET/CT, with MRI and ultrasound reserved for specific indications.
1. Peripheral Tumours
About 40% of bronchial carcinomas arise beyond the segmental bronchi; in 30% a peripheral mass is the sole radiographic finding.
Tumour Shape and Margins
| Feature | Description |
|---|---|
| Shape | Approximately spherical or oval; lobulation common (reflects uneven growth rates) |
| Corona radiata | Numerous fine strands radiating from the central mass - highly suggestive of bronchial carcinoma (though not specific) |
| Pancoast (superior sulcus) tumour | Apical tumour that may resemble apical pleural thickening |
| Pleural tail | Peripheral line shadow between mass and pleura - represents plate-like atelectasis or lymphatic obstruction |
| Ill-defined edges | Seen especially in adenocarcinoma - can mimic pneumonia |
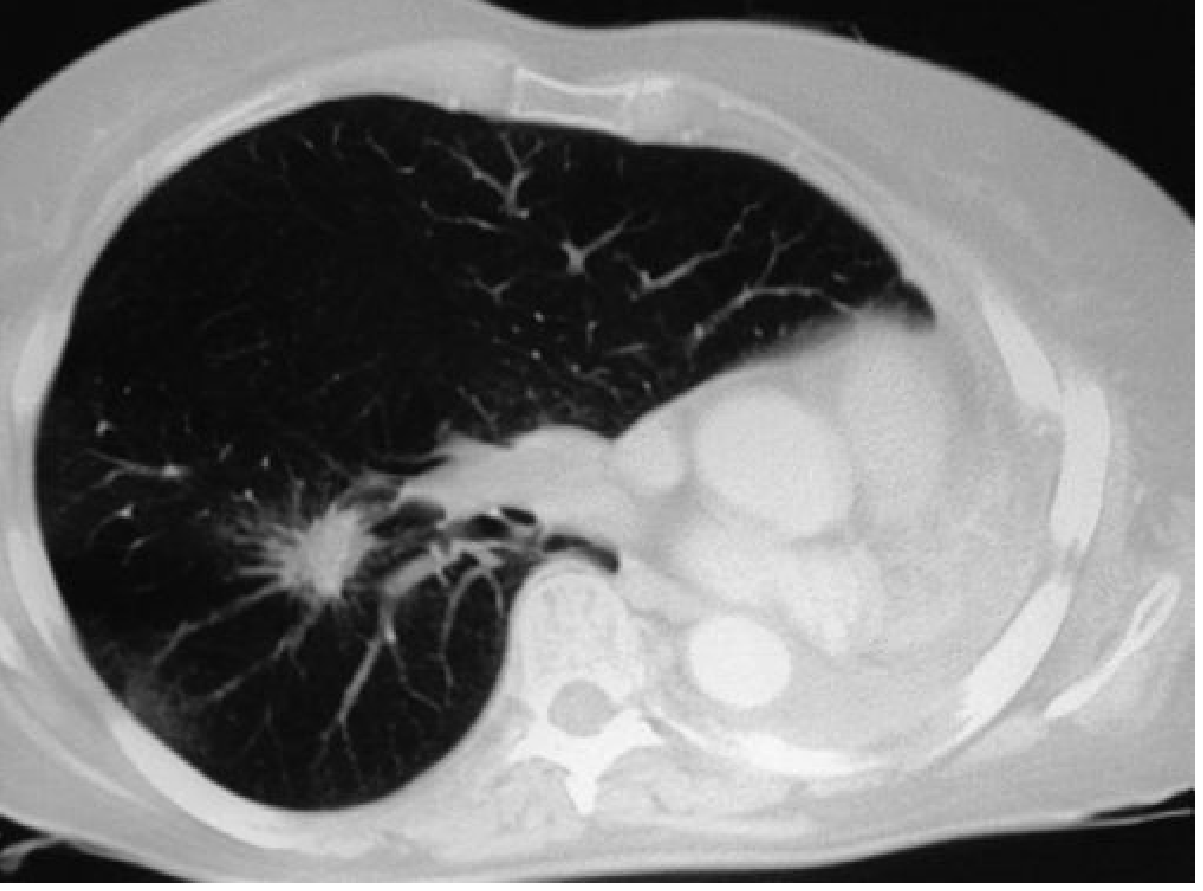
CT demonstrating corona radiata - second primary bronchogenic carcinoma (right lung) with spiculated, infiltrating edges:
Cavitation
- Can occur in tumours of any size; best demonstrated by CT
- Squamous cell carcinoma is the most likely cell type to cavitate
- Wall: irregular thickness, usually ≥8 mm thick; may contain tumour nodules
- Fluid levels are common
Calcification
- Rarely seen on plain chest radiograph
- Identified on CT in 6-10% of cases
- May represent pre-existing calcified granuloma engulfed by tumour, or dystrophic tumour calcification
- Most calcified tumours are large (≥5 cm diameter)
Other CT Findings
- Air bronchograms and bubble-like lucencies (pseudo-cavitation) - especially adenocarcinoma
- Ground-glass attenuation (GGA): associated with greater malignancy risk; more common with adenocarcinoma (may present as purely GGA nodule)
- Bronchocele/mucocele: dilated mucus-filled bronchi distal to an obstructing carcinoma
2. Central Tumours
The cardinal imaging signs are:
- Collapse/consolidation of the lung beyond the tumour
- Hilar enlargement
These signs may appear in isolation or together.
Collapse/Consolidation - Key CT Signs
- A soft-tissue density within a collapsed or consolidated lobe, separate from the normal vessels and bronchi
- Irregular or tapered bronchial narrowing or cut-off (vs. smooth compression from extrinsic causes)
- A visible mass with irregular stenosis of a mainstem or lobar bronchus
- Enlarged central nodes on CT/MRI (simple pneumonia rarely causes radiographically visible hilar adenopathy)
- Mucus-filled dilated bronchi within collapsed lobes on CT: branching tubular low-density structures - should prompt search for a centrally obstructing tumour
3. Staging Intrathoracic Spread
Hilar Enlargement on CXR
- May reflect a proximal tumour, lymphadenopathy, consolidated lung, or a combination
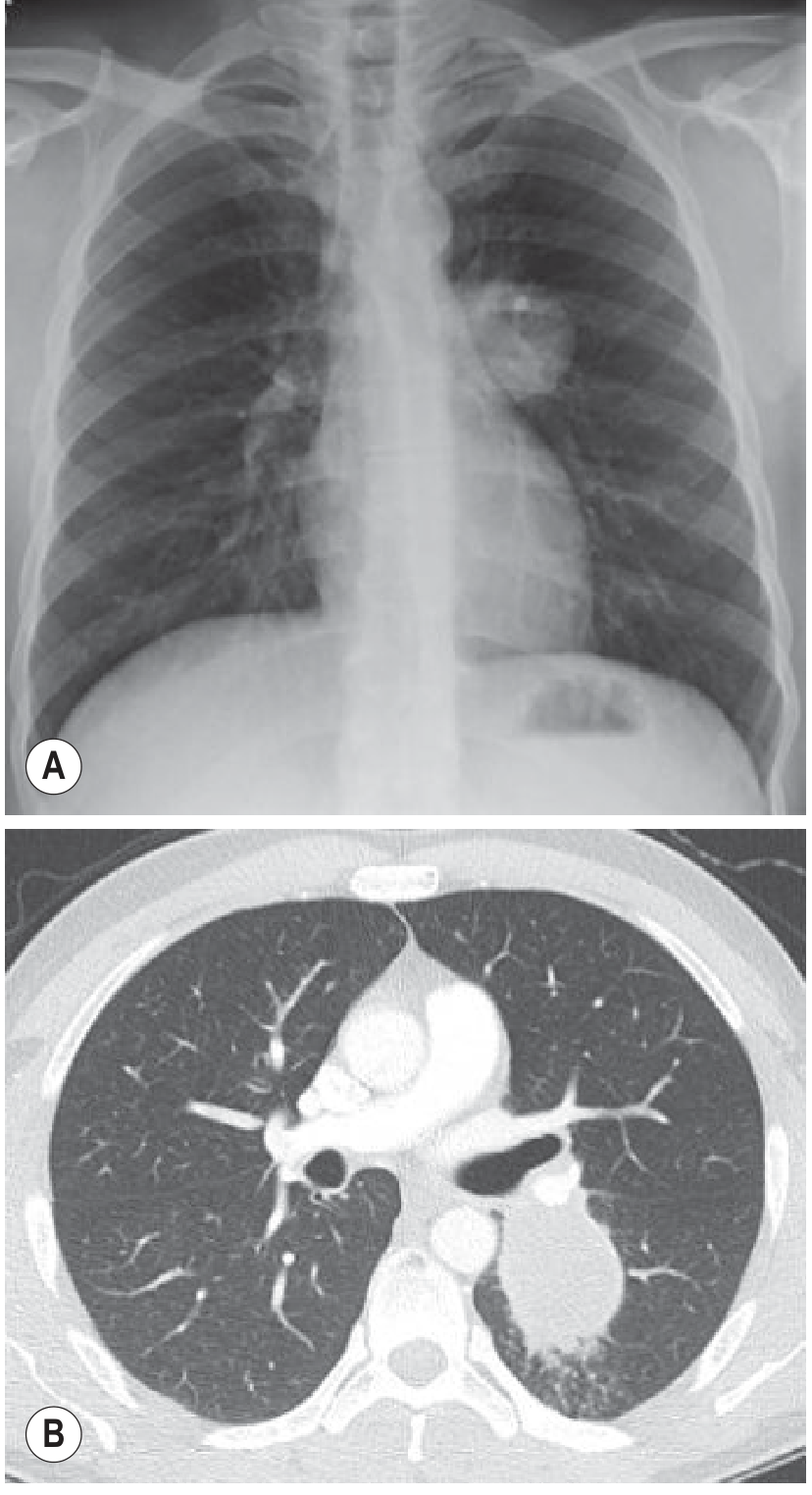
- A "dense hilum" sign: mass superimposed on the hilum increases density due to summation - may be the only indication of lung cancer on frontal CXR
- Must always inspect the lateral radiograph when a dense hilum is suspected
CXR (A) showing dense left hilum; CT (B) demonstrating mass lying behind the left hilum - proven squamous cell carcinoma:
Mediastinal Invasion
- CXR: phrenic nerve paralysis (high hemidiaphragm) - but caution: lobar collapse, sub-pulmonary effusion, and diaphragmatic eventration can mimic this
- CT/MRI signs: visible tumour deep within mediastinal fat, especially if surrounding mediastinal vessels, oesophagus, or proximal mainstem bronchi
- Criteria suggesting resectability (Glazer criteria):
- <3 cm contact with the mediastinum
- <90° circumferential contact with the aorta
- A visible mediastinal fat plane between mass and vital mediastinal structures
- Even clear-cut contact is not enough for diagnosis of invasion; apparent interdigitation can be misleading
Pleural Effusion
- CT/MRI density measurements for distinguishing malignant vs. reactive pleural fluid have not proven useful
- PET may have a role in evaluating pleural effusion
PET/CT in Nodal Staging
CT (A) showing malignant left hilar nodes from small peripheral NSCLC; PET/CT (B) confirming high FDG uptake:
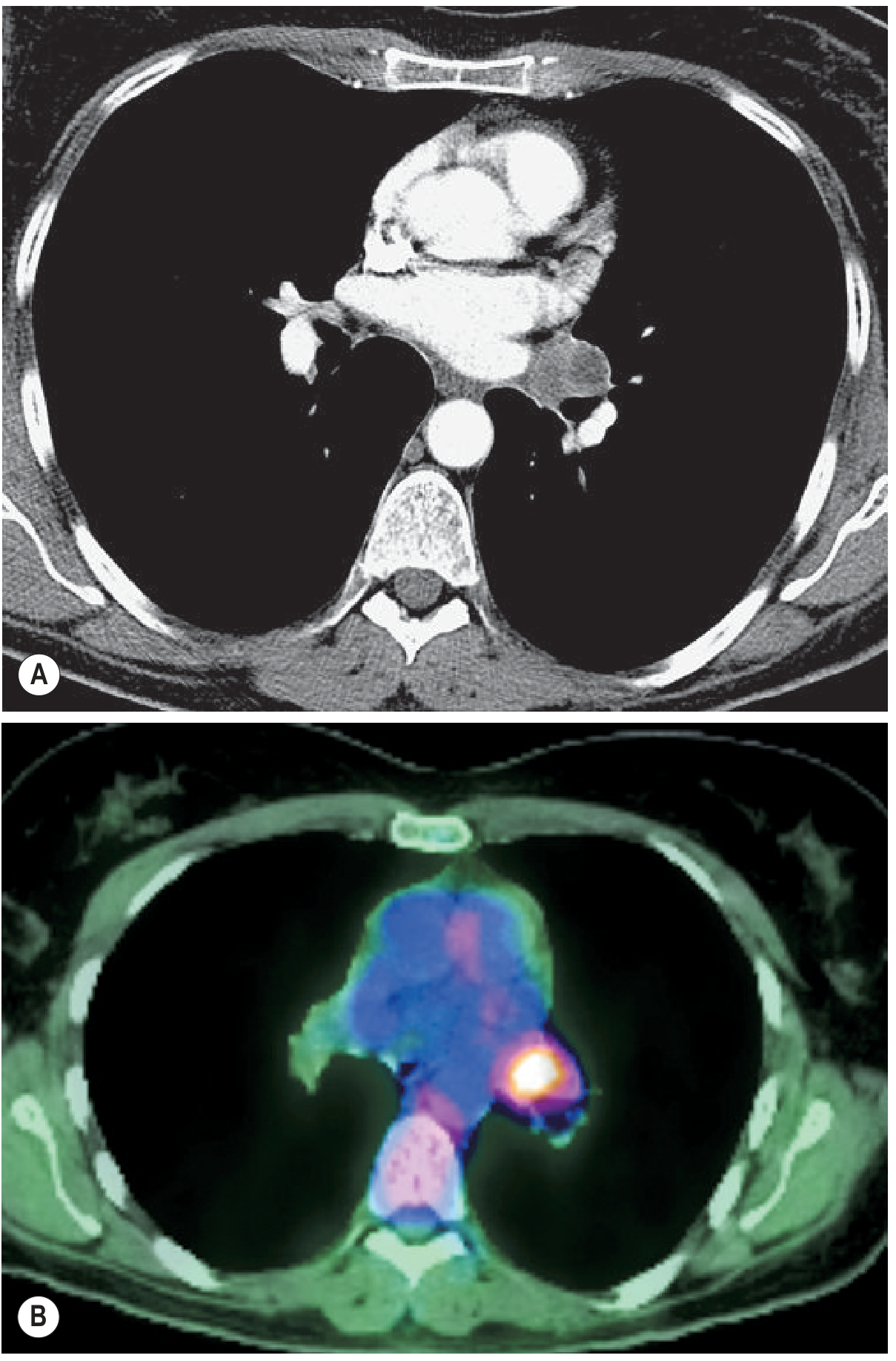
- CT limitations: poor specificity for nodal involvement - enlarged nodes may be reactive, due to coincidental benign disease, or associated consolidation/atelectasis
- Positive PET does not obviate need for histological confirmation of nodal involvement
- Negative CT + negative PET: very high likelihood that mediastinal nodes are clear - surgical resection can proceed without invasive mediastinal staging
Imaging Modality Summary
| Modality | Role |
|---|---|
| Chest X-ray (CXR) | First-line; detects peripheral mass, central hilar enlargement, dense hilum sign, collapse, effusion |
| CT (HRCT/contrast) | Characterises tumour (shape, margins, cavitation, calcification, GGA); evaluates mediastinal and hilar nodes, chest wall/mediastinal invasion; guides biopsy |
| 18F-FDG PET/CT | Nodal and distant staging; identifies occult metastatic disease; evaluates pleural effusion; assesses treatment response |
| MRI | Selected indications: chest wall invasion (superior sulcus tumours), cardiac/vascular involvement, patients who cannot have IV contrast |
| Ultrasound | Guidance for pleural fluid sampling or peripheral lesion biopsy |
Summary of Staging Decision Algorithm
- If CXR + CT ± PET show no spread beyond the lung (other than to ipsilateral hilar nodes) and bronchoscopy confirms resectability → proceed to surgical resection
- Spread to ipsilateral nodes: adverse prognosis, but surgery not necessarily precluded
- Biopsy confirmation of neoplastic nodal involvement (mediastinoscopy, mediastinotomy, or needle aspiration) is usually required before denying surgery to a patient with enlarged nodes on CT
Staging is a multidisciplinary process combining imaging, bronchoscopy, and biopsy, reviewed in lung cancer MDT (multidisciplinary team) discussion.
- Grainger & Allison's Diagnostic Radiology, Chapter 8 (Thoracic Imaging Features of Bronchial Carcinoma)
This is a shared conversation. Sign in to Orris to start your own chat.