Analyze this text like a strategy consultant. Identify the key ideas, missed opportunities, and strategic implications I should act on immediately.Analyze the methodology, key findings, and limitations of this academic paper step by step Then, write a three-sentence summary focused on how the study's findings can be applied on practice.Read this text and point out the hidden assumptions, biases, or unspoken perceptions that most readers would overtook - but experts would noticeHodgkin's lymphoma and it's classification in detail
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive, authoritative content from three major textbooks. Here is the full multi-lens analysis you requested.
Hodgkin Lymphoma: A Multi-Lens Deep Analysis
🔍 PART 1 — Strategic Consultant Lens: Key Ideas, Missed Opportunities & Actionable Implications
Key Ideas
- HL is fundamentally a disease of the microenvironment, not just the tumor cell. Reed-Sternberg (RS) cells account for less than 10% of tumor mass; the rest is reactive host cells. The RS cells engineer their own sanctuary by secreting cytokines (IL-5, IL-10, M-CSF), chemokines (eotaxin), and immune checkpoint ligands (PD-L1, PD-L2). The tumor hijacks the immune system as a support network.
- NF-κB is the master oncogenic switch. Whether via EBV's LMP-1 protein, loss-of-function mutations in IκB, or copy number gains in the REL proto-oncogene (chromosome 2p), virtually all classic HL converges on NF-κB activation — making it a high-value therapeutic target.
- HL was the first human cancer cured by radiation + chemotherapy. It remains one of oncology's greatest success stories, with cure rates exceeding 80–90% in early-stage disease.
Missed Opportunities (What the Standard Narrative Glosses Over)
- The macrophage signal is underemphasized: A high number of tumor-associated macrophages is a strong independent predictor of treatment resistance — yet macrophage quantification is rarely part of standard clinical decision-making.
- The ICC renaming of NLPHL (now called "nodular lymphocyte-predominant B-cell lymphoma") signals a paradigm shift that has not fully penetrated clinical practice. Many practitioners still manage NLPHL as a subtype of HL when its biology — CD20+, CD30−, CD15−, EBV− — warrants a distinct therapeutic approach closer to indolent B-cell NHL.
- PD-L1/PD-L2 amplification on chromosome 9p means classic HL is among the tumors most biologically primed for checkpoint inhibitor therapy — yet PD-1 inhibitors (pembrolizumab, nivolumab) remain underused in first-line refractory settings in resource-limited environments.
Strategic Actions to Take Immediately
- In any relapsed/refractory classic HL case: Confirm PD-L1 status and consider checkpoint inhibitor eligibility. The biology mandates it.
- Reclassify NLPHL in your practice framework: Treat it more like indolent B-cell lymphoma (anti-CD20 therapy), not classic HL with ABVD.
- Assess tumor-associated macrophage density at diagnosis as an informal prognostic flag for treatment intensification.
📋 PART 2 — Academic Paper Methodology Lens: Step-by-Step Analysis
(Applied to the WHO Classification framework and its evidence base as represented in these authoritative texts)
Step 1 — Methodology
The WHO classification system is built on a morphology-first, immunophenotype-second, molecular-third tiered framework:
- Morphological criteria: Identification of RS cells (large, 45 µm, bilobed nuclei, "owl eye" nucleoli ~5–7 µm) and their variants (lacunar, mononuclear, lymphohistiocytic/L&H cells).
- Immunophenotyping: Panel including CD30, CD15, PAX5/BSAP, CD20, CD45, CD79a.
- Molecular confirmation: Used to resolve diagnostic ambiguity (clonal IGH rearrangements, somatic hypermutation signature).
The frequency data cited in Goldman-Cecil Medicine (n = 2,488 cases, British Columbia, 1998–2020) provides the epidemiological substrate for subtype prevalence.
Step 2 — Key Findings
| Subtype | Frequency | Key Feature |
|---|---|---|
| Nodular sclerosis (CHL) | ~60% | Lacunar RS cells; collagen bands; CD30+/CD15+ |
| Mixed cellularity (CHL) | ~9% | EBV-associated; eosinophil-rich |
| Lymphocyte-rich (CHL) | ~3% | Best prognosis among CHL |
| Lymphocyte-depleted (CHL) | ~1% | Worst prognosis; often HIV-associated |
| NLPHL | ~8% | CD20+, CD30−, CD15−, EBV−; L&H "popcorn" cells |
| HL, not otherwise classifiable | ~19% | Diagnostic limitation acknowledged |
Pathogenesis consensus: RS cells originate from germinal center or post-germinal center B cells with clonal IGH rearrangements — confirmed by single-cell molecular studies. Despite B-cell origin, classic RS cells lose B-cell gene expression through epigenetic reprogramming.
Step 3 — Limitations
- The 19% "not otherwise classifiable" category is a frank admission that the classification is incomplete — nearly 1 in 5 cases cannot be cleanly binned.
- Data source bias: The epidemiological frequency data derives from a single Canadian registry (British Columbia). Racial, geographic, and socioeconomic factors — known to influence HL subtype distribution — are not captured.
- Morphology dependence: RS cells can be mimicked in infectious mononucleosis, solid tumors, and certain NHLs. Misclassification risk is real without full immunophenotyping.
- ICC vs. WHO tension: The 2022 ICC reclassification of NLPHL away from the HL umbrella reveals ongoing expert disagreement — the classification is not settled science.
✏️ Three-Sentence Practical Summary
Classic Hodgkin lymphoma is diagnosed by identifying CD30+/CD15+ Reed-Sternberg cells in a reactive inflammatory background, and subtyped by morphology, immunophenotype, and EBV status — a framework that directly guides therapy intensity and choice of regimen. The fundamental distinction between classic HL (CD20−/CD30+/CD15+/EBV±) and nodular lymphocyte-predominant HL (CD20+/CD30−/CD15−/EBV−) has immediate therapeutic implications: NLPHL responds to anti-CD20 agents (rituximab) and carries a distinct relapse pattern, while classic HL is uniquely susceptible to PD-1 checkpoint blockade due to constitutive PD-L1/PD-L2 overexpression. Clinicians should treat the macrophage-rich tumor microenvironment as a prognostic variable and not merely histological background noise, as high macrophage infiltration independently predicts treatment failure.
🧠 PART 3 — Expert Lens: Hidden Assumptions, Biases & Unspoken Perceptions
Most readers absorb the classification table and move on. Experts notice these fault lines:
1. The "B-cell origin" fact is taken for granted — but it was revolutionary
The textbooks present RS cell B-cell origin as established fact. What is glossed over: this was unknwon for most of the 20th century because RS cells silenced their B-cell gene program so completely they appeared to be of uncertain lineage. The proof came only from elegant single-cell PCR studies in the 1990s. The pedagogy presents a solved puzzle; the actual science was a 50-year mystery. This matters because it implies further unknown epigenetic reprogramming mechanisms in HL remain undiscovered.
2. "Reactive cells make up >90% of the tumor" is treated descriptively, not strategically
The standard framing: RS cells are rare, surrounded by innocent bystanders. The expert reading: those reactive cells are not innocent — they are an active therapeutic target. The cytokine loops (RS cells activate eosinophils/T-cells → those cells activate CD30/CD40 on RS cells → NF-κB upregulated) represent a feedback circuit that chemotherapy alone does not interrupt cleanly. This is why residual disease and late relapses occur.
3. EBV association is presented as epidemiological — the mechanistic implication is downplayed
The text notes EBV-infected B cells in infectious mononucleosis resemble RS cells. This is an extraordinary observation presented almost as a footnote. It implies EBV may be a sufficient driver of the RS cell phenotype via LMP-1/NF-κB. The unstated corollary: EBV-seronegative young adults who develop HL may represent a biologically distinct disease from EBV+ cases — different oncogenic routes, possibly warranting different treatment.
4. The ICC/WHO split is mentioned briefly — its significance is underplayed
The reclassification of NLPHL as "nodular lymphocyte-predominant B-cell lymphoma" by the ICC is noted in passing. The hidden message: this is a landmark paradigm dispute between two competing international bodies (the ICC and the WHO 5th edition team) that reflects genuine scientific disagreement. Clinicians using one classification vs. the other will enroll patients in different trials and prescribe different therapies. The polite academic framing obscures a live clinical controversy.
5. The "bimodal age distribution" hides three distinct diseases
The bimodal peak (young adults + elderly >55) is cited as a single entity with a curious epidemiological pattern. Experts recognize that the Cummings Otolaryngology text makes the more precise observation: three distinct epidemiological forms exist — childhood HL (≤14), young adult HL (15–34), and older adult HL (55–74) — each with different EBV associations, subtype distributions, and outcomes. Collapsing them into "bimodal" is a pedagogical oversimplification that can mislead treatment planning.
6. The "curable in most cases" framing obscures late toxicity burden
The triumphalist framing — "first cancer cured by radiation and chemotherapy" — suppresses a critical counter-narrative: late effects of therapy (secondary malignancies, cardiac toxicity, pulmonary fibrosis from bleomycin, infertility) often emerge 10–20 years post-cure and rival the original disease in morbidity. The classification and staging framework was not designed with survivorship toxicity in mind.
Histology Reference
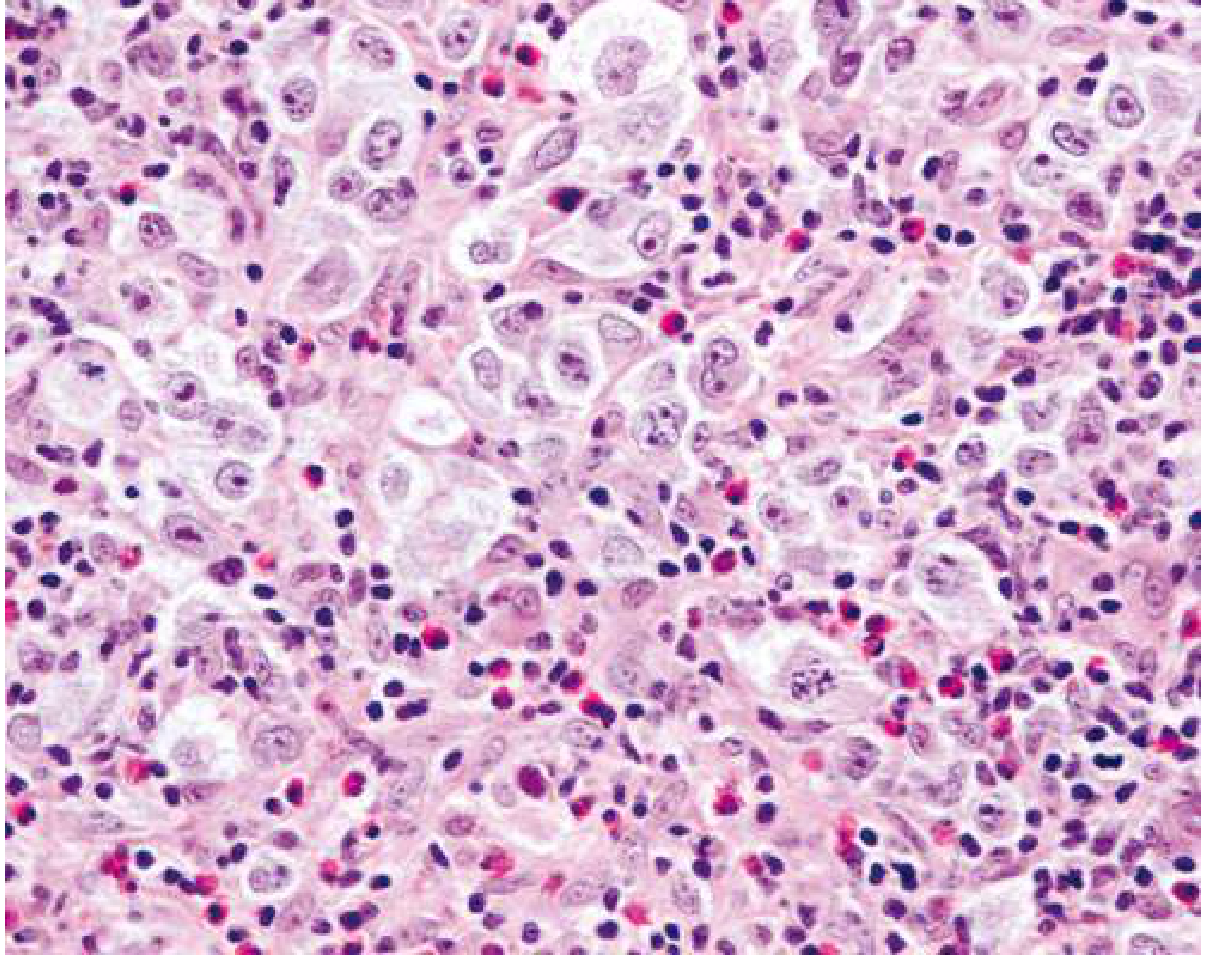
Nodular sclerosing Hodgkin lymphoma (H&E). Large lacunar RS cell variants are visible amid a mixed inflammatory background of lymphocytes and eosinophils — the classic histological signature of the most common HL subtype.
Sources:
- Robbins, Cotran & Kumar — Pathologic Basis of Disease (10th ed.)
- Robbins & Kumar — Basic Pathology
- Goldman-Cecil Medicine, International Edition (2-volume set)
- Cummings Otolaryngology — Head and Neck Surgery
Hodgkin's lymphoma
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive data from Goldman-Cecil Medicine, Robbins Basic Pathology, and Cummings Otolaryngology. Here is a complete, authoritative breakdown.
Hodgkin Lymphoma — Complete Clinical Overview
1. Definition
Hodgkin lymphoma (HL) is a B-cell lymphoid neoplasm characterized by rare, large neoplastic cells called Reed-Sternberg (RS) cells embedded in an extensive reactive inflammatory background of lymphocytes, eosinophils, plasma cells, and histiocytes. It encompasses two major categories:
- Classic Hodgkin Lymphoma (CHL) — ~90% of cases
- Nodular Lymphocyte-Predominant Hodgkin Lymphoma (NLPHL) — ~10% of cases
Both have distinct natural histories but share an excellent response to treatment, with the large majority of patients being cured.
— Goldman-Cecil Medicine
2. Epidemiology
| Feature | Detail |
|---|---|
| Annual incidence (North America + Europe) | ~30,000 new cases/year |
| Age-adjusted incidence | ~2.7 per 100,000 |
| Age-adjusted mortality | ~0.5 per 100,000 |
| Sex | Slightly more common in males |
| Age distribution | Bimodal — peak at 25–30 yrs, second peak >50 yrs |
| Geographic variation | Highest in USA, Canada, northern Europe; lowest in eastern Asia |
| Childhood HL | Strong bias toward the Indian subcontinent |
Cumulative lifetime risk in North America is approximately 1 in 250 to 1 in 300. — Goldman-Cecil Medicine
3. Etiology & Pathobiology
Epstein-Barr Virus (EBV)
- EBV is the leading suspect but no definitive causal proof exists
- A history of infectious mononucleosis triples the subsequent risk of HL
- EBV-encoded RNA is demonstrable in RS cells in ~50% of all HL cases and up to 70% of mixed-cellularity subtype
- The EBV genome is monoclonal in all RS cells within a given case, indicating infection precedes transformation
- EBV-encoded LMP-1 protein activates NF-κB, the master survival switch in RS cells
Origin of Reed-Sternberg Cells
RS cells originate from germinal center or post-germinal center B cells — established by single-cell microdissection studies demonstrating identical clonal IGH rearrangements with somatic hypermutation signatures. Despite B-cell origin, RS cells in classic HL paradoxically silence most B-cell genes, including immunoglobulin expression, through widespread epigenetic reprogramming. — Robbins Basic Pathology
NF-κB — The Master Oncogenic Axis
Virtually all classic HL converges on NF-κB activation via multiple routes:
- EBV LMP-1 signaling (EBV+ cases)
- Loss-of-function mutations in IκB (negative regulator of NF-κB)
- Copy number gains in the REL proto-oncogene (chromosome 2p)
NF-κB is hypothesized to rescue "crippled" germinal center B cells that can no longer express immunoglobulin from apoptosis — setting the stage for malignant transformation.
Immune Evasion
RS cells evade host immunity through:
- PD-L1 and PD-L2 overexpression (chromosome 9p amplification) — inhibiting cytotoxic T-cell responses
- Loss of β₂-microglobulin → failure to express class I MHC molecules → invisible to CD8+ T cells
- Secretion of IL-10, a broadly immunosuppressive cytokine
This biology makes classic HL uniquely sensitive to PD-1 checkpoint inhibitors (nivolumab, pembrolizumab).
The Reactive Microenvironment
RS cells engineer their own tumour sanctuary by secreting:
- IL-5 → attracts eosinophils
- TGF-β → fibrogenesis (nodular sclerosis)
- IL-13 → autocrine RS cell growth stimulation
- Eotaxin → eosinophil chemotaxis
In turn, the recruited eosinophils and T cells express ligands activating CD30 and CD40 on RS cells → further NF-κB upregulation. The microenvironment is not innocent — it is an active co-conspirator.
4. Classification (WHO)
| Subtype | Type | Frequency | Key Features |
|---|---|---|---|
| Nodular sclerosis | Classic | ~60% | Lacunar RS cells; collagen bands; young adults; mediastinal mass |
| Mixed cellularity | Classic | ~9% | EBV-rich; eosinophils; older/HIV+ patients |
| Lymphocyte-rich | Classic | ~3% | Best prognosis among CHL |
| Lymphocyte-depleted | Classic | ~1% | Worst prognosis; fibrosis; older/immunocompromised |
| Nodular lymphocyte-predominant (NLPHL) | Non-classic | ~8% | CD20+, CD30−, CD15−, EBV−; "popcorn" L&H cells |
| Not otherwise classifiable | — | ~19% | Unresolved diagnostic category |
Immunophenotype comparison:
| Marker | Classic HL | NLPHL |
|---|---|---|
| CD30 | ✅ 90–100% | ❌ |
| CD15 | ✅ 75–85% | ❌ |
| CD20 | ~40% (weak/focal) | ✅ strong |
| CD45 | ❌ | ✅ |
| PAX5/BSAP | ✅ (dim) | ✅ |
| EBV | Variable | ❌ |
5. Clinical Features
- Painless peripheral lymphadenopathy — most common presentation; typically cervical and supraclavicular
- Mediastinal mass — classic in nodular sclerosis; may cause cough, dyspnoea, SVC syndrome
- Severe generalised pruritus — common in HL, rare in NHL; may precede diagnosis by months
- B symptoms (present in ~25% of patients):
- Fever >38°C (unexplained, recurrent)
- Drenching night sweats
- Unexplained weight loss >10% body weight over 6 months
- Pel-Ebstein fever — cyclical high fever, pathognomonic but rare
- Alcohol-induced pain at nodal sites — characteristic though uncommon
6. Staging — Modified Ann Arbor System
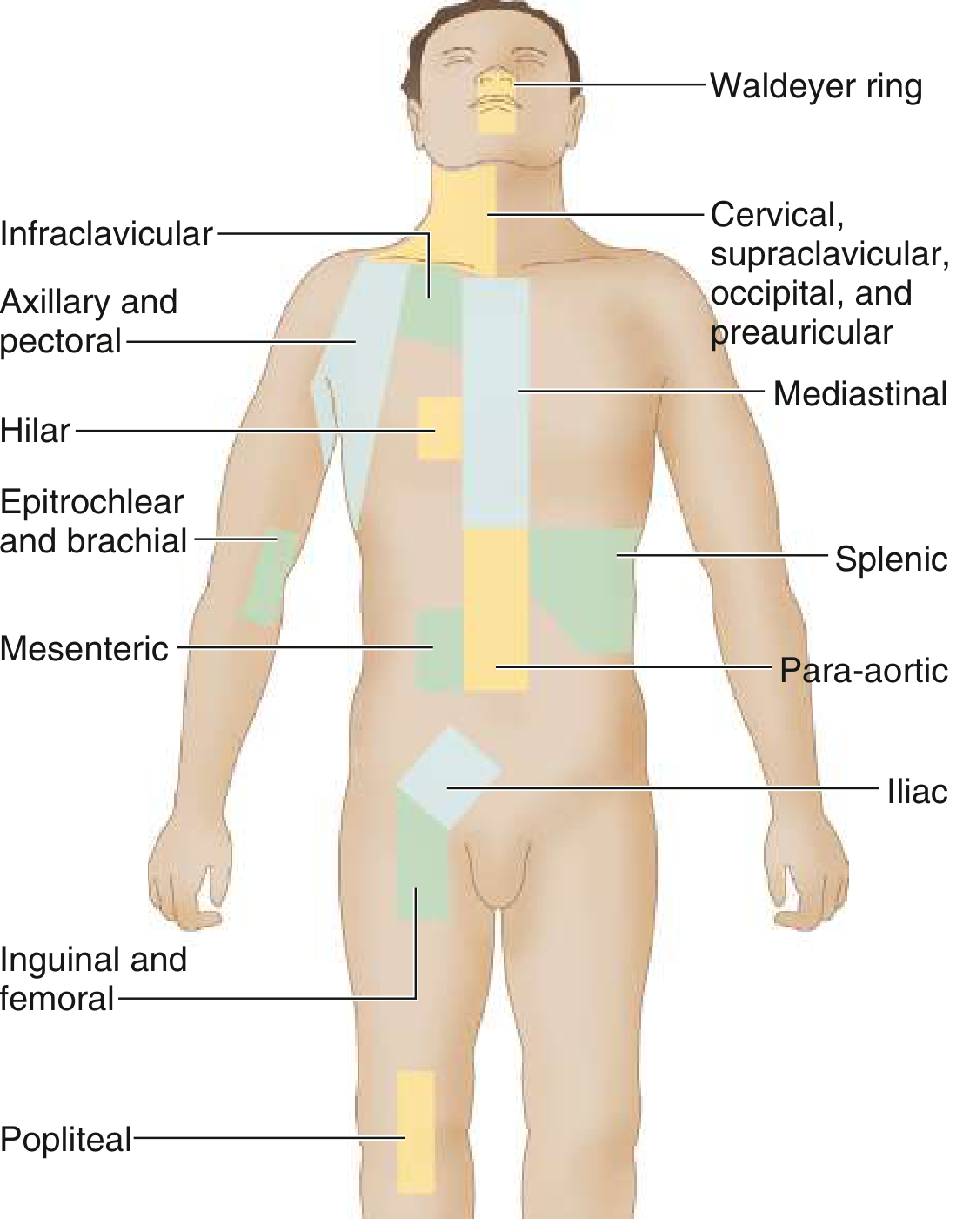
Anatomic lymph node regions for HL staging — Goldman-Cecil Medicine
| Stage | Definition |
|---|---|
| I | Single lymph node region or one extralymphatic site |
| II | ≥2 lymph node regions, same side of diaphragm |
| III | Lymph node regions on both sides of diaphragm |
| IV | Diffuse extralymphatic organ involvement |
Suffixes:
- A = no B symptoms
- B = fever, night sweats, or weight loss present
- E = limited contiguous extranodal extension
- X = bulky disease (mass ≥10 cm or mediastinal mass ratio >1/3 thoracic diameter)
Limited stage = stages I–II without bulky disease
Advanced stage = stage III, IV, or any bulky disease
7. Workup & Investigations
Required for staging (Goldman-Cecil Medicine):
- Full history (B symptoms) + physical examination
- Complete blood count, ESR
- Serum creatinine, alkaline phosphatase, LDH, bilirubin, albumin, protein electrophoresis
- HIV, hepatitis B/C serology
- Chest radiograph (PA + lateral)
- CT scan — neck, thorax, abdomen, pelvis (≤1 cm slice intervals)
- FDG-PET/CT — more sensitive/specific than CT or gallium for both staging and post-treatment response assessment; bone marrow biopsy is no longer required when PET is performed
8. Treatment
Limited-Stage (Stages IA/IIA, non-bulky) — Cure rate >95%
| Approach | Details |
|---|---|
| Standard | ABVD × 2 cycles + involved-region radiotherapy (IRRT) |
| Chemo-only | ABVD × 3 cycles — if PET shows complete metabolic remission, no radiation needed |
| Checkpoint inhibitor | Nivolumab/pembrolizumab + AVD × 4 — emerging for PET-positive after chemo |
Advanced-Stage (Stages IB, IIB, III, IV, or bulky) — Cure rate 60–80%
| Regimen | Details |
|---|---|
| A+AVD | Brentuximab vedotin + doxorubicin + vinblastine + dacarbazine × 6 cycles — now standard; improves 5-yr PFS and OS vs ABVD |
| ABVD | Doxorubicin + bleomycin + vinblastine + dacarbazine × 6 cycles — bleomycin dropped if PET negative after cycle 2 |
| Escalated BEACOPP | Bleomycin + etoposide + doxorubicin + cyclophosphamide + vincristine + procarbazine + prednisone — higher disease control but more toxicity; option for <60 yrs |
Relapsed/Refractory
- Second-line chemotherapy (e.g., ICE, DHAP)
- High-dose chemoradiotherapy + autologous hematopoietic cell transplantation
- PD-1 inhibitors (nivolumab, pembrolizumab) — highly active due to constitutive PD-L1/L2 expression on RS cells
9. Prognosis
- Early-stage (IA/IIA): Cure rate >90–95%
- Advanced-stage: Cure rate 60–80% depending on International Prognostic Score (IPS) factors
- IPS adverse factors (advanced disease): Male sex, age ≥45, stage IV, haemoglobin <10.5 g/dL, WBC ≥15,000/µL, lymphocyte count <600/µL or <8%, serum albumin <4 g/dL
- Patients event-free at 2 years have an excellent long-term outlook, though retain an enduring elevated risk of death from all causes vs. general population
Late Treatment Toxicities (the hidden burden)
- Secondary malignancies (particularly breast cancer with mediastinal radiation, lung cancer)
- Cardiac toxicity (doxorubicin cardiomyopathy, radiation-induced coronary artery disease)
- Pulmonary fibrosis (bleomycin toxicity)
- Hypothyroidism (cervical/mediastinal radiation)
- Infertility (alkylating agents, particularly procarbazine in BEACOPP)
10. NLPHL — Distinct Entity
NLPHL behaves differently from classic HL and warrants separate consideration:
- Neoplastic cells are lymphocytic and histiocytic (L&H) "popcorn" cells
- CD20+, CD79a+, CD45+, CD30−, CD15−, EBV−
- Indolent course with late relapses; rarely transforms to diffuse large B-cell lymphoma
- Responds well to anti-CD20 therapy (rituximab)
- The 2022 International Consensus Classification has renamed it "nodular lymphocyte-predominant B-cell lymphoma" — dropping the Hodgkin designation entirely — reflecting its fundamentally different biology
Sources:
- Goldman-Cecil Medicine, International Edition (2-vol set)
- Robbins & Kumar — Basic Pathology
- Cummings Otolaryngology — Head and Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.