Hello, chron disease
Reading File
Finding Sources
Searching PubMed
"Crohn disease"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive answer. Here is a full overview of Crohn's disease:
Crohn's Disease
Definition
Crohn's disease (CD) is a chronic, relapsing inflammatory bowel disease (IBD) that can affect any segment of the gastrointestinal tract from mouth to anus, characterized by transmural inflammation, skip lesions, and non-caseating granulomas. - Robbins & Kumar Basic Pathology
Epidemiology & Etiology
CD is most common in Western populations, with rising incidence in previously low-prevalence areas. Risk factors include:
- Genetics: Over 200 IBD-associated risk alleles identified. The most important is NOD2 (encodes an intracellular sensor for muramyl dipeptide, a bacterial cell wall component) - present in ~30% of CD patients vs. 5% of healthy individuals in European populations. CD is polygenic - accumulated polymorphisms in immune signaling, bacterial response, and epithelial defense genes all contribute. - Robbins, Cotran & Kumar Pathologic Basis of Disease
- Environmental: Tobacco use is implicated in etiology and exacerbation. Oral contraceptive use and alcohol have also been linked. - Schwartz's Principles of Surgery
- Microbiome: Dysregulated host-microbe interactions are central to disease initiation
Pathophysiology
IBD arises from a combination of:
- Genetic susceptibility (NOD2 and >200 other loci)
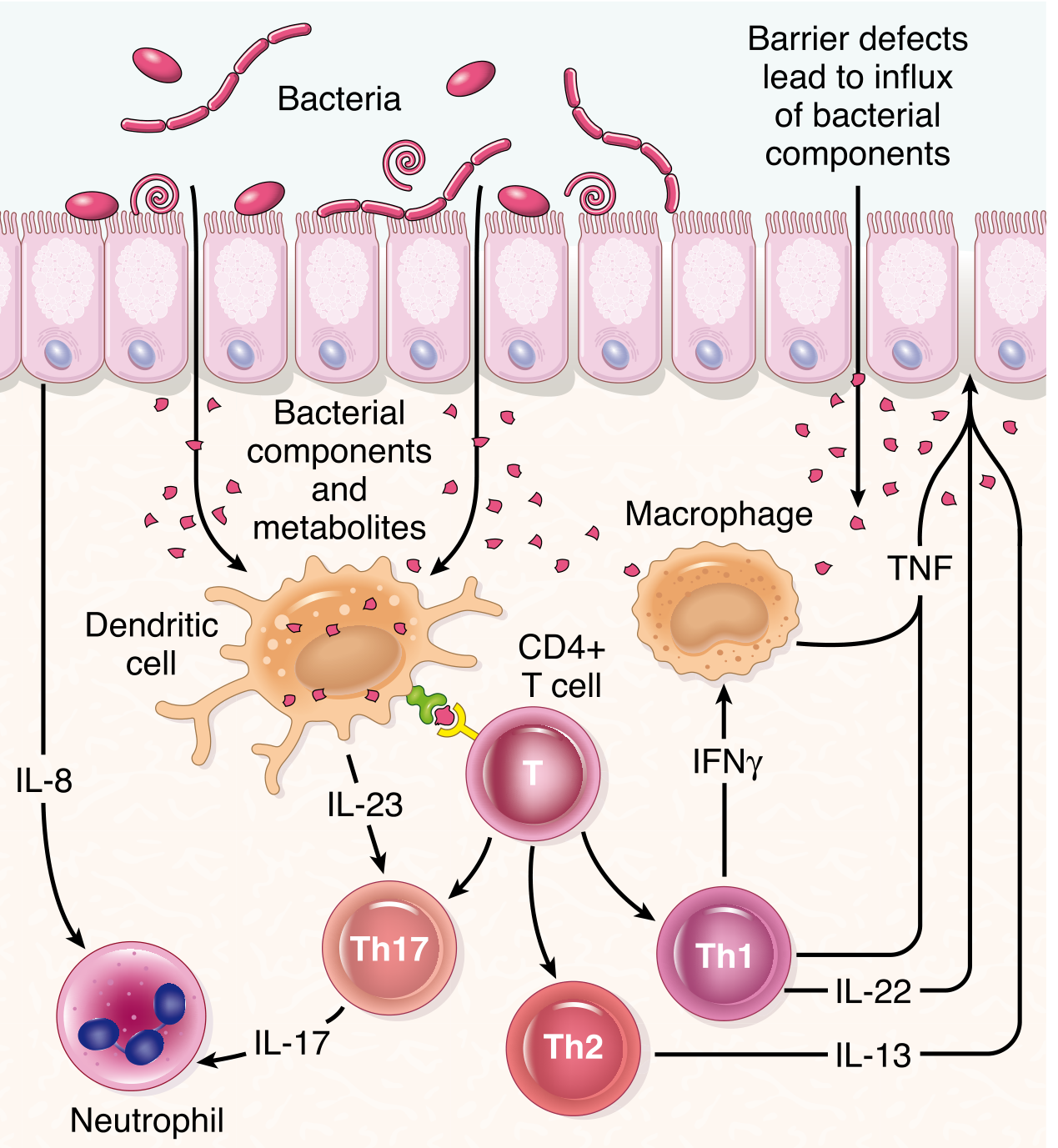
- Epithelial barrier dysfunction - barrier defects allow influx of bacterial components into the lamina propria
- Aberrant immune responses - dendritic cells present bacterial antigens to CD4+ T cells, driving Th1 and Th17 polarization with release of TNF, IFN-γ, IL-17, IL-23, and other cytokines that sustain chronic inflammation
Transmural inflammation leads to:
- Fibrosis and stricture formation
- Fistula and abscess formation (penetrating disease)
- Adhesions to adjacent bowel or organs
- "Fat wrapping" - mesenteric fat encroachment onto the bowel serosa, virtually pathognomonic of CD - Schwartz's Principles of Surgery
Distribution
- Small bowel involved in 80% of cases; colon alone in 20%
- Majority of small bowel disease = ileocecal disease
- Isolated perianal/anorectal disease: 5-10%
- Uncommon sites: esophagus, stomach (usually with concurrent intestinal disease), duodenum
- Skip lesions: discontinuous inflamed segments separated by normal-appearing intestine - Schwartz's Principles of Surgery
Pathology - Key Features
| Feature | Crohn's Disease | Ulcerative Colitis |
|---|---|---|
| Inflammation depth | Transmural | Mucosal only |
| Distribution | Skip lesions, anywhere mouth-to-anus | Continuous, always involves rectum |
| Granulomas | Non-caseating, present | Absent |
| Fistulas | Common | Rare |
| Rectum spared | Often | Never |
| Small bowel | Commonly involved | Backwash ileitis only |
- Robbins & Kumar Basic Pathology; ROSEN's Emergency Medicine
Clinical Presentation
The classic triad is abdominal pain, diarrhea, and weight loss. Disease behavior falls into three overlapping patterns:
- Fibrostenotic - obstructive symptoms from strictures
- Fistulizing / penetrating - internal fistulas, abscesses
- Aggressive inflammatory - active mucosal inflammation
Onset is typically insidious with a waxing-and-waning course. Children may present with growth retardation. Up to one-quarter of patients develop extraintestinal manifestations. - Schwartz's Principles of Surgery
Extraintestinal manifestations include:
- Arthritis / arthralgia
- Skin: erythema nodosum, pyoderma gangrenosum
- Eyes: iritis, uveitis
- Oral: aphthous stomatitis
- Perianal disease (fissures, fistulas, abscesses)
Diagnosis & Disease Activity
Disease activity is classified as mild, moderate, or severe based on response to therapy, systemic toxicity, abdominal tenderness, mass/obstruction, and degree of malnutrition.
The Crohn's Disease Activity Index (CDAI) is the standard research tool:
- Remission: CDAI < 150
- Response to therapy: decrease in CDAI ≥ 100 points
Key variables: stool count, abdominal pain, general well-being, extraintestinal features, opiate use, abdominal mass, hematocrit, and body weight.
Biomarkers:
- CRP - useful for tracking activity; elevated CRP correlates with active disease and risk of infectious complications
- Fecal calprotectin - pooled sensitivity 88%, specificity 67% for active CD vs. endoscopy. Also correlates with relapse risk and biologic therapy response
- Fecal lactoferrin - sensitive marker of intestinal inflammation
Symptoms do not always correlate with objective disease activity - mucosal healing (endoscopic + biomarker-based) has emerged as the therapeutic target beyond symptom control. - Sleisenger and Fordtran's GI and Liver Disease
Imaging: MR enterography with gadolinium shows mural hyperenhancement, mural thickening, and the "comb sign" (engorged peri-enteric vasculature resembling comb teeth) in the terminal ileum.
Complications
- Small bowel obstruction (SBO): CD is the primary cause in ~5% of SBO cases. May result from active inflammation or chronic fibrosis/strictures. Up to 75% of patients undergo at least one abdominal surgery in their lifetime.
- Intra-abdominal abscess and fistulas
- Colorectal cancer: Risk increased after >8-10 years of colonic IBD
- Short bowel syndrome (from repeated resections)
Management
Medical Therapy
Step-up approach based on disease severity:
| Class | Agents | Use |
|---|---|---|
| Aminosalicylates | Mesalamine | Mild-moderate disease |
| Corticosteroids | Prednisone, budesonide | Induction of remission |
| Immunomodulators | Azathioprine, 6-mercaptopurine, methotrexate | Maintenance; steroid-sparing |
| Biologic - anti-TNF-α | Infliximab, adalimumab | Moderate-severe disease, fistulizing CD |
| Biologic - anti-integrin | Vedolizumab | Gut-selective; moderate-severe CD |
| JAK inhibitors / IL-12/23 blockers | Ustekinumab, upadacitinib | Refractory disease |
- Anti-TNF therapies are effective by inhibiting the pro-inflammatory cascade, but up to 50% of patients ultimately become unresponsive to their first anti-TNF biologic. Some respond to a second anti-TNF agent. - Robbins, Cotran & Kumar
- For gastric/duodenal CD: PPIs are first-line; controlled trial data on immunosuppressants and biologics is lacking, though infliximab has been used successfully. - Sleisenger and Fordtran's
- Despite biologic availability, up to 40% of CD patients still require long-term corticosteroids, which significantly increase surgical morbidity (infection, anastomotic leak). - Fischer's Mastery of Surgery
Surgical Therapy
Surgery is integral in CD management. Key principles:
- Preserve intestinal length - wide margins do not reduce recurrence but increase short bowel syndrome risk
- Indications: intra-abdominal abscess, medically intractable fistula, fibrotic stricture with obstruction, toxic megacolon, malignancy, failure of optimal medical therapy, steroid dependence, growth failure in children
- Most common operation: ileocecal resection with primary anastomosis, increasingly done laparoscopically
- The LIR:C trial showed no QOL difference at 12 months between laparoscopic ileocecal resection and infliximab in limited ileal CD (<40 cm) - suggesting primary resection is an acceptable alternative to biologic therapy in select patients
- Strictureplasty is preferred over resection for isolated fibrotic/scattered strictures (bowel-sparing)
- IPAA (ileal pouch-anal anastomosis) is generally avoided in established CD due to high pouch failure rates
- Risk of second surgery: ~30% at 5 years; ~33% of those needing a second surgery will need a third. - Sleisenger and Fordtran's
Surveillance
Colonoscopic surveillance for dysplasia/adenocarcinoma is recommended after 8-10 years of colonic IBD involvement.
Recent evidence (2024-2026):
- A 2025 meta-analysis in J Crohn's Colitis found partial enteral nutrition (PEN) has a role in CD management, particularly in pediatric populations (PMID 39565924)
- A 2025 Lancet Gastroenterology & Hepatology systematic review proposed novel diagnostic criteria and management advice specifically for isolated perianal Crohn's disease (PMID 40315877)
- A 2024 meta-analysis in United European Gastroenterol J reviewed probiotics in IBD - modest benefit but not yet standard of care (PMID 39106167)
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology; Schwartz's Principles of Surgery 11e; ROSEN's Emergency Medicine; Fischer's Mastery of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.