Myringoplasty in detail with incision position instruments
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching Images
myringoplasty tympanoplasty surgical technique incision
Reading File
Loading Image
Loading Image
Reading File
I now have sufficient detail from the textbook to compose a comprehensive answer. Let me synthesize everything.
Myringoplasty — Detailed Overview
Myringoplasty is the surgical repair of a tympanic membrane (TM) perforation without manipulation of the middle ear ossicles. When ossicular reconstruction is also performed, the procedure is termed tympanoplasty. Myringoplasty is essentially Type I tympanoplasty (Wullstein classification).
1. Definition & Goals
- Restore an intact, infection-resistant TM
- Improve conductive hearing loss
- Prevent recurrent middle ear disease (cholesteatoma, repeated infections)
- Re-establish the transformer mechanism of the middle ear
2. Indications
- Chronic tympanic membrane perforation (central, not marginal)
- Chronic otitis media (tubotympanic/mucosal type, inactive — dry ear)
- Conductive hearing loss from TM perforation
- Dysventilation syndromes and atelectasis
Prerequisites: Dry ear for ≥3 months, patent Eustachian tube, no active infection, no cholesteatoma.
3. Surgical Approaches — Incision Positions
A. Postauricular (Retroauricular) Approach — Most Common
- A Wilde's incision is made 5–10 mm behind the postauricular sulcus, running from the superior attachment of the auricle to its inferior pole
- The skin and subcutaneous tissue are incised down to the periosteum
- The periosteum is marked and incised; a Lempert elevator elevates the periosteum anteriorly to expose the spine of Henle and the bony canal
- Provides wide exposure, ideal for large perforations, revision cases, and simultaneous mastoidectomy
- Allows generous graft harvesting (temporalis fascia)
B. Endaural (Rosen's) Incision
- Incision placed between the tragus and helix in the incisura terminalis (notch of Rivinus)
- Extended superiorly into the conchal bowl
- Used when more limited exposure is needed; intermediate between transcanal and postauricular approaches
C. Transcanal Approach
- No external skin incision
- Tympanomeatal flap elevated entirely through the ear canal
- A vascular strip incision is made: vertical incisions at 6 o'clock and 12 o'clock connected by a horizontal incision just lateral to the annulus
- Limited to small to moderate central perforations with adequate canal width
- Can be done under microscope or endoscope (endoscopic myringoplasty)
4. Vascular Strip
Lying in the posterosuperior canal between the tympanomastoid and tympanomastoid suture lines, the vascular strip carries the deep auricular branch of the maxillary artery — the main blood supply to the TM. It must be handled carefully to avoid tearing. If suture lines are prominent, a sickle knife or No. 5910 Beaver blade is used to incise fibrous tissue.
5. Graft Material
| Graft | Features |
|---|---|
| Temporalis fascia | Most commonly used; harvested through postauricular incision; excellent |
| Tragal/conchal perichondrium | Easily harvested; good results |
| Cartilage + perichondrium | Used for retraction pockets, atelectasis, revision cases |
| Fat graft (lobule) | For small central perforations; office-based procedures |
| AlloDerm (acellular dermis) | Allogenic option; used in revision cases |
6. Graft Placement Techniques
Underlay (Medial) Technique — Most Common
- Graft placed medial to the fibrous annulus and TM remnant
- Graft rests on the medial surface; supported by Gelfoam packing in the middle ear
- Ideal for posterior and inferior central perforations
- Less technically demanding; avoids risk of lateralization or anterior blunting
- Middle ear is entered by lifting the annulus out of the tympanic sulcus with a pick or hook
Overlay (Lateral) Technique
- Graft placed lateral to the fibrous layer of TM remnant, medial to the malleus handle
- Requires complete removal of squamous epithelium from the TM remnant surface (to prevent iatrogenic cholesteatoma)
- Requires bony canalplasty for anterior visualization
- Useful for large perforations, anterior perforations, revision cases
- Greater vascular ingrowth potential; promotes epithelialization
7. Instruments Used
General Set
| Instrument | Use |
|---|---|
| Wilde's retractor / self-retaining retractor | Maintain postauricular wound exposure |
| Lempert periosteal elevator | Elevate periosteum from mastoid cortex and canal |
| Sickle knife (No. 1 knife) | Tympanomeatal flap incision; vascular strip incisions |
| No. 5910 Beaver blade | Fine incisions in tympanomastoid suture lines |
| Rosen needle (pick) | Elevate annulus from tympanic sulcus |
| Drum elevator (Duckbill elevator) | Elevate tympanomeatal flap |
| Curette (small House curette) | Remove granulation tissue; freshen perforation edges |
| Alligator forceps / cup forceps | Grasp and position graft; remove tissue |
| Suction (Rosen/Baron suction tips) | Delicate suction in external canal and middle ear |
| Gelfoam (absorbable gelatin sponge) | Medial packing to support graft under TM |
| Ear speculum (various sizes) | Maintain canal visualization (transcanal approach) |
| Microscope / endoscope (0°, 30°, 45°) | Magnification and illumination |
| Bipolar cautery | Hemostasis in soft tissues |
| Fascia press | Thin the harvested temporalis fascia to desired thickness |
| Irrigation syringe | Gentle canal cleaning |
8. Step-by-Step Operative Technique (Postauricular Underlay)
- Positioning: Supine, head turned contralateral; operating microscope positioned
- Infiltration: Local anaesthetic with adrenaline (1:100,000) in canal and postauricular area
- Incision: Wilde's postauricular incision, 5–10 mm behind sulcus
- Graft harvest: Temporalis fascia harvested, thinned with fascia press, allowed to dry
- Periosteal elevation: Lempert elevator exposes bony canal; self-retaining retractor placed
- Vascular strip incisions: Sickle knife at 12 and 6 o'clock, connected horizontally just lateral to annulus
- Tympanomeatal flap elevation: Flap elevated from lateral to medial using drum elevator; annulus freed from sulcus with Rosen needle
- Middle ear entry: Posterior half of drum lifted; chorda tympani identified and preserved
- Perforation edge freshening: Margins of perforation denuded of epithelium with small curette or pick to create a raw edge for graft adherence
- Gelfoam packing: Absorbable gelatin foam placed in middle ear for graft support
- Graft placement: Dry fascia slid medial to TM remnant and annulus; positioned over Gelfoam
- Flap repositioning: Tympanomeatal flap laid back over graft
- Canal packing: Gelfoam strips or ribbon gauze placed lateral to graft in canal
- Wound closure: Postauricular wound closed in layers (periosteum, subcutaneous, skin)
- Dressing: Mastoid dressing applied
9. Postoperative Care
- Ear kept dry for 4–6 weeks
- Antibiotic eardrops after canal pack removal (1–2 weeks)
- Avoid nose blowing; Valsalva manoeuvre contraindicated
- Audiogram at 6–8 weeks to assess hearing improvement
- Success rates for Type I tympanoplasty: 80–95% (graft uptake); no single technique or approach has been shown superior in meta-analyses
10. Complications
| Complication | Notes |
|---|---|
| Graft failure/re-perforation | Most common; higher in smokers, revision cases, poor Eustachian tube function |
| Iatrogenic cholesteatoma | Risk with overlay technique if squamous epithelium not completely removed |
| Anterior blunting | Angle between anterior canal wall and TM lost; more common with overlay |
| Conductive hearing loss (residual) | May persist if ossicular pathology unaddressed |
| Sensorineural hearing loss | Rare; from manipulation near oval/round window |
| Chorda tympani injury | Taste disturbance; occurs during middle ear entry |
| Tinnitus, vertigo | Uncommon; from inner ear disturbance |
Surgical Images
Postauricular Wilde's incision and tympanomeatal flap elevation:
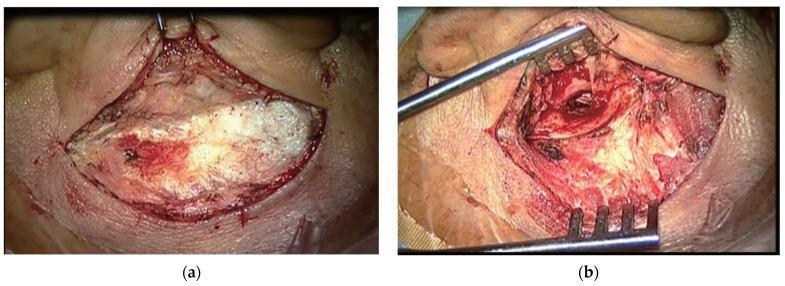
(a) Postauricular Wilde's incision with mastoid cortex exposed. (b) Tympanomeatal flap elevated, external auditory canal visible as dark circular opening.
Large subtotal perforation (A) and underlay temporalis fascia graft placement (B):
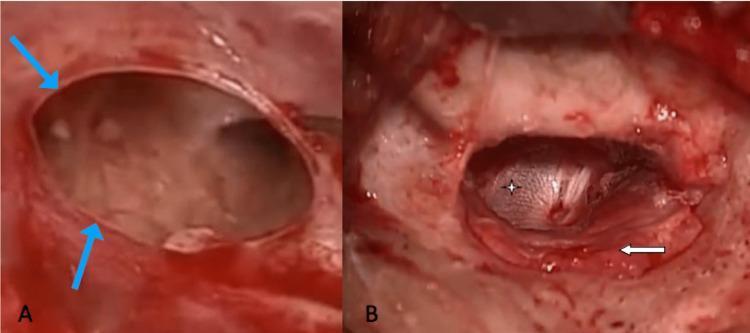
(A) Large subtotal perforation with edges marked by blue arrows. (B) Temporalis fascia graft (star) placed by underlay technique; tympanomeatal flap (arrow) repositioned over graft posterior margin.
— Cummings Otolaryngology Head and Neck Surgery, Chapter 142 (Tympanoplasty and Ossiculoplasty)
— K.J. Lee's Essential Otolaryngology
Complication of csom tubo tympanic
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content to compile a thorough answer. Let me synthesize it.
Complications of CSOM — Tubotympanic (Mucosal/Safe) Type
CSOM tubotympanic disease is called "safe" because it carries a lower risk of serious complications compared to the atticoantral (cholesteatoma) type — but complications do still occur, typically when infection spreads beyond the mucosal confines of the middle ear cleft.
Complications are classified into Extracranial (Intratemporal) and Intracranial groups.
Classification (Box 141.1 — Cummings Otolaryngology)
Extracranial (Intratemporal)
- Acute mastoiditis
- Coalescent mastoiditis
- Chronic mastoiditis
- Masked mastoiditis
- Postauricular (subperiosteal) abscess
- Bezold abscess
- Temporal abscess
- Petrous apicitis (Gradenigo syndrome)
- Labyrinthine fistula
- Facial nerve paralysis
- Acute suppurative labyrinthitis
- Encephalocele and CSF leakage
Intracranial
- Meningitis
- Brain abscess
- Subdural empyema
- Epidural abscess
- Lateral (sigmoid) sinus thrombosis
- Otitic hydrocephalus
Routes of Spread
| Route | Mechanism |
|---|---|
| Direct extension | Bone erosion by granulation tissue; spread through pre-formed pathways (sutures, air cell tracts) |
| Haematogenous | Via emissary veins and diploic veins |
| Preformed pathways | Petrosquamous suture, Hyrtl fissure, round window membrane, congenital dehiscences |
Extracranial Complications in Detail
1. Acute Mastoiditis
- Most common extracranial complication
- Occurs when AOM/COM fails to resolve → mucosal edema blocks aditus ad antrum → pus accumulates in mastoid air cells
- Features: Fever, post-auricular pain, tenderness, erythema, auricle displaced anteroinferiorly
- Pathogens: S. pneumoniae, S. pyogenes, S. aureus, H. influenzae
- Coalescent mastoiditis: Bony septa between air cells dissolve → empyema cavity forms
- Managed with IV antibiotics ± myringotomy ± cortical mastoidectomy
2. Subperiosteal (Postauricular) Abscess
- Pus erodes through the lateral cortex of the mastoid → collects between periosteum and bone
- Pinna pushed anteriorly and laterally; post-auricular sulcus obliterated
- Requires incision and drainage + mastoidectomy
3. Bezold Abscess
- Pus perforates the medial/inner cortex of the mastoid tip → tracks along sternocleidomastoid (SCM) muscle sheath into the neck
- Presents as a deep neck swelling along the anterior border of SCM
- Can track to mediastinum → descending necrotising mediastinitis (rare, life-threatening)
4. Temporal (Zygomatic) Abscess
- Pus extends anteriorly through zygomatic air cells → subcutaneous abscess over the zygoma/temple
5. Petrous Apicitis (Gradenigo Syndrome)
- Infection spreads through the petrous apex air cells
- Classic Gradenigo's triad:
- Ipsilateral CN VI palsy (abducens — lateral rectus palsy → diplopia)
- Deep retro-orbital/facial pain (CN V — Meckel's cave irritation)
- Otorrhoea (purulent discharge)
- Managed with IV antibiotics; surgical drainage if no improvement
6. Labyrinthine Fistula
- More common with cholesteatoma, but can occur in tubotympanic CSOM with granulation tissue
- Usually involves the lateral semicircular canal (most exposed)
- Presents with sensorineural hearing loss, vertigo, positive fistula test (pressure-induced nystagmus)
- Managed surgically — fistula sealed with fascia graft
7. Facial Nerve Paralysis
- Bacteria reach the facial nerve via congenital dehiscences of the fallopian canal or erosion by granulation tissue
- In CSOM without cholesteatoma: affects the horizontal (tympanic) segment near the stapes
- Onset is usually gradual (unlike cholesteatoma, where it can be acute)
- Progression from partial to complete palsy
- Managed by mastoidectomy + facial nerve decompression; best outcomes if decompressed within 1 week of onset
- If nerve undergoes complete degeneration before surgery, prognosis is poor
8. Acute Suppurative Labyrinthitis
- Bacterial invasion of the labyrinth → immediate, total, irreversible loss of auditory and vestibular function
- Extension usually via weakened oval window membrane or round window
- Presents with sudden profound SNHL + severe vertigo + nausea/vomiting
- Treated with high-dose IV antibiotics; hearing loss is permanent
- Can progress to meningitis via the cochlear aqueduct or IAC
Intracranial Complications in Detail
1. Meningitis
- Most common intracranial complication overall
- Spread via: labyrinth → cochlear aqueduct → subarachnoid space; or direct dural erosion
- Features: high fever, severe headache, neck stiffness, photophobia, Kernig's/Brudzinski's signs
- CSF: turbid, raised protein, low glucose, polymorphs, organisms on gram stain
- Managed with IV antibiotics (penicillin/cephalosporin/chloramphenicol) + mastoidectomy after stabilisation
2. Brain Abscess
- Second most common intracranial complication in COM
- Temporal lobe abscess (via tegmen erosion) and cerebellar abscess (via sigmoid sinus or posterior fossa erosion)
- Stages: encephalitis → central softening → abscess capsule formation
- Features: headache, fever (may be low grade or absent), focal neurological deficits, seizures, papilloedema
- CT/MRI: ring-enhancing lesion
- Managed: neurosurgical drainage (aspiration/excision) + IV antibiotics + mastoidectomy
3. Epidural Abscess
- Pus accumulates between the dura and inner cortex of temporal bone
- Often asymptomatic or mild headache; discovered incidentally on CT
- Dura acts as a barrier → less serious unless it progresses
- Treated by mastoidectomy with evacuation of abscess
4. Subdural Empyema
- Pus between dura and arachnoid
- Spreads rapidly over the cerebral surface → very serious
- Features: fever, headache, meningism, focal deficits, altered consciousness, seizures
- Neurosurgical craniotomy/drainage is priority; then mastoidectomy
5. Lateral (Sigmoid) Sinus Thrombosis
- Infection from mastoid air cells → perisinus abscess → thrombophlebitis → sigmoid sinus thrombosis
- Features:
- Picket-fence (hectic) fever — characteristic spiking fever with rigors
- Griesinger's sign: oedema and tenderness over mastoid emissary vein (posterior to mastoid)
- Tobey-Ayer test: compression of ipsilateral internal jugular vein → no rise in CSF pressure (thrombosis blocks venous return)
- Can embolise → septic pulmonary emboli, septicaemia
- Managed with mastoidectomy, removal of infected thrombus, IV antibiotics; anticoagulation controversial
6. Otitic Hydrocephalus
- Raised intracranial pressure without evidence of abscess, meningitis, or thrombosis
- Mechanism: lateral sinus thrombosis → impaired CSF absorption at arachnoid granulations → raised ICP
- Features: severe headache, papilloedema, diplopia (CN VI palsy), visual changes; CSF is normal in composition
- Treated with acetazolamide, serial lumbar punctures, or CSF shunting; mastoidectomy for underlying disease
Key Points: Why Tubotympanic is "Safer" But Not Safe
| Feature | Tubotympanic (Mucosal) | Atticoantral (Cholesteatoma) |
|---|---|---|
| Perforation | Central | Marginal / attic |
| Discharge | Profuse, mucoid | Scanty, foul-smelling |
| Bone erosion | Absent | Present (enzymatic) |
| Complication risk | Lower | Higher |
| Complications seen | Mainly mastoiditis, labyrinthitis, meningitis | All of above + more frequent facial palsy, fistula |
Investigations for Suspected Complications
- CT temporal bone — bony erosion, mastoid opacification, sinus plate erosion
- MRI brain with contrast — intracranial extension, abscess ring enhancement, sinus thrombosis
- CBC — leukocytosis
- Blood cultures — septicaemia
- Lumbar puncture — CSF analysis for meningitis (contraindicated if raised ICP with brain abscess/subdural empyema)
Management Principles
- IV broad-spectrum antibiotics covering aerobes and anaerobes (e.g., ceftriaxone + metronidazole)
- Mastoidectomy — to eradicate the primary source
- Neurosurgical intervention (aspiration/drainage) for intracranial collections
- Sequential or concurrent treatment of the ear and intracranial complication
- Post-treatment follow-up CT/MRI to confirm resolution — new complications can emerge
— Cummings Otolaryngology Head and Neck Surgery, Chapter 141 (Complications of Temporal Bone Infections)
This is a shared conversation. Sign in to Orris to start your own chat.