Bells palsy
Reading File
Finding Sources
Searching PubMed
"Bell palsy"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is a detailed overview of Bell's Palsy:
Bell's Palsy
Definition & Epidemiology
Bell's palsy is the most common cause of acute unilateral facial paralysis, affecting the peripheral facial nerve (cranial nerve VII) on an idiopathic basis. The diagnosis is one of exclusion.
- Incidence: ~23-25 per 100,000 persons annually (~1 in 60 persons over a lifetime)
- Affects men and women roughly equally, at all ages
- Risk factors: diabetes mellitus, pregnancy (especially the third trimester and first 2 weeks postpartum - up to 3x increased risk), hypertension
Pathophysiology
The facial nerve (CN VII) controls:
- Motor innervation to all muscles of facial expression and the scalp
- The stapedius muscle
- Taste to the anterior two-thirds of the tongue (via chorda tympani)
Viral reactivation is the leading mechanism:
- HSV type 1 (herpes simplex) DNA has been detected in endoneurial fluid surrounding the facial nerve in the majority of cases - it is thought to reactivate in the geniculate ganglion
- Varicella-zoster virus (VZV) accounts for up to one-third of cases and is the second most common cause
- Other implicated viruses: SARS-CoV-2, HIV (at seroconversion), EBV
Histologically, there is mononuclear cell inflammation of the facial nerve, consistent with an infectious or immune-mediated cause. Swelling of the nerve within the tight bony facial canal leads to compression and ischemia.
Clinical Features
| Feature | Details |
|---|---|
| Onset | Acute; maximal weakness in 48 hours (practically all within 3-4 days) |
| Prodrome | Retroauricular (behind-the-ear) pain 1-2 days before paralysis |
| Motor | Complete or partial unilateral facial palsy - includes forehead (distinguishes LMN from UMN lesion) |
| Taste | Impaired taste (anterior 2/3 tongue) - usually resolves within 2 weeks |
| Hearing | Hyperacusis (due to stapedius paralysis) |
| Sensory | Mild facial numbness/hypoesthesia in some patients |
| CSF | Mild lymphocytosis in a small number of cases |
Key distinguishing point: In Bell's palsy (lower motor neuron), both the upper face (forehead) AND lower face are affected. In upper motor neuron lesions (e.g. stroke), the forehead is spared because upper facial muscles receive bilateral cortical input.
MRI Findings
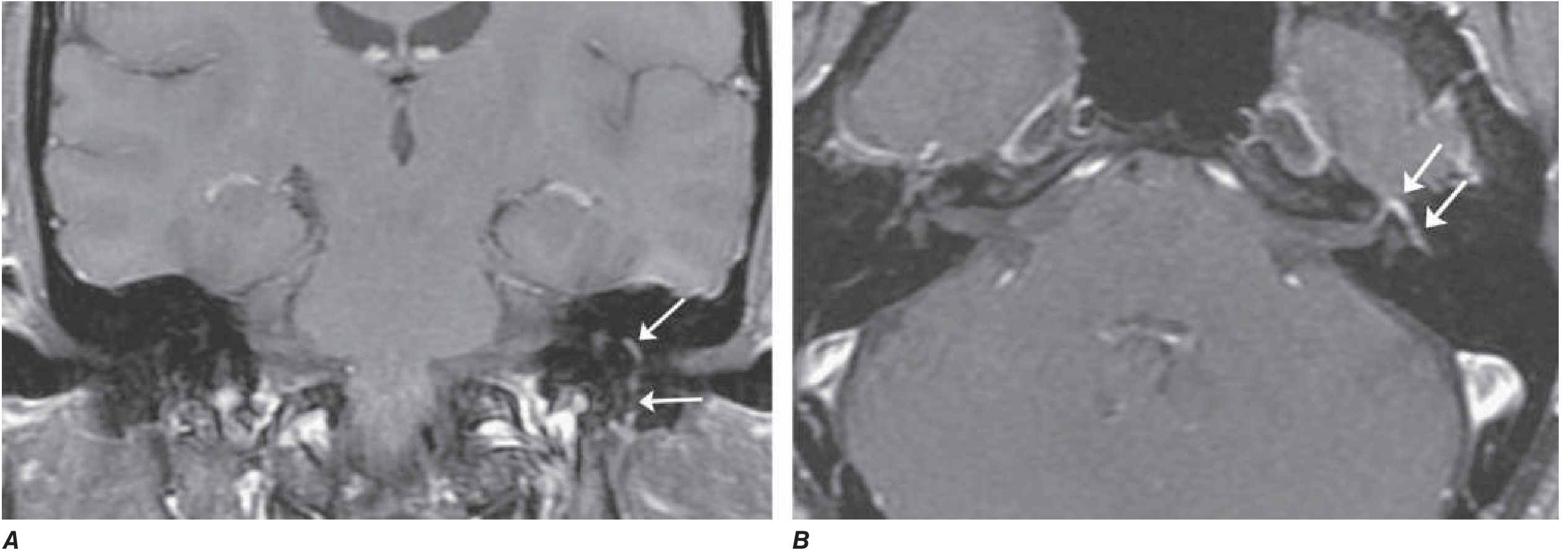
Axial and coronal T1-weighted images with gadolinium + fat suppression showing diffuse smooth linear enhancement of the left facial nerve within the temporal bone (arrows). Note: similar findings can occur with Lyme disease, sarcoidosis, and perineural malignant spread. - Harrison's Principles of Internal Medicine, 22E
Differential Diagnosis
Bell's palsy is a diagnosis of exclusion. Other causes of peripheral facial palsy to consider:
| Cause | Key Clues |
|---|---|
| Ramsay Hunt syndrome (VZV) | Vesicular rash in external auditory canal, ear pain, CN VIII involvement (vertigo, deafness) |
| Lyme disease | Endemic area exposure, may cause bilateral palsy, erythema migrans history |
| Sarcoidosis | Often bilateral; elevated ACE, hilar adenopathy |
| Guillain-Barré syndrome | Often bilateral, ascending paralysis, CSF albuminocytologic dissociation |
| HIV | At seroconversion; associated CSF pleocytosis |
| Malignancy / parotid tumor | Slow onset, progressive, no recovery |
| Leprosy | Endemic areas, skin lesions, sensory loss |
| Melkersson-Rosenthal syndrome | Recurrent facial palsy + facial edema + fissured tongue |
| Diabetes mellitus | Can cause facial neuropathy independently |
Investigations
The diagnosis is clinical in typical cases. The following are NOT routinely required but indicated in atypical presentations:
- EMG/nerve conduction: performed after 10 days; evidence of denervation = axonal degeneration = poor prognosis (expect 3+ months to recovery)
- MRI with gadolinium: shows facial nerve enhancement and swelling; useful to exclude mass lesion
- Lyme serology, HIV test, ACE level + chest imaging (for sarcoidosis), ESR/CRP, fasting glucose
- Lumbar puncture: if Guillain-Barré is suspected
Prognosis
- ~70-80% of patients recover completely within 1-2 months
- ~85% achieve near-normal function
- About 10% have little to no recovery
- Favorable signs: incomplete paralysis in the first week; early return of some motor function in days 5-7; early return of taste (within first week)
- Unfavorable signs: EMG denervation after 10 days (indicates axonal degeneration; long regeneration timeline of ~3 months)
- Recurrence in ~7-8% of cases, on average ~10 years between episodes
- Complications of aberrant regeneration: synkinesis (jaw-winking - eye closes when jaw moves), "crocodile tears" (tearing with salivation)
Treatment
1. Supportive / Eye Protection (Essential in all patients)
- Tape the upper eyelid shut during sleep to prevent corneal drying/exposure keratopathy
- Artificial tears (lubricating eye drops) during the day
- Massage of weakened muscles
2. Glucocorticoids (First-line, start ASAP)
- Prednisone 60-80 mg/day for 5 days, then taper over the next 5 days (Harrison's) OR
- Prednisolone 25 mg twice daily for 10 days (Goldman-Cecil)
- Increases return of full facial function from ~63% to ~83% at 3 months
- Thought to reduce nerve swelling within the tight facial canal
- Most benefit when started within 72 hours of onset
3. Antiviral Agents
- Valacyclovir 1000 mg/day for 5-7 days OR Acyclovir 400 mg five times daily for 7-10 days
- Most RCT evidence does NOT support antivirals alone or in combination with steroids for routine Bell's palsy
- Use if: vesicular lesions present in the palate/ear canal (suggesting VZV/Ramsay Hunt), or if complete facial palsy (one study by Hato et al. showed additive benefit of valacyclovir + prednisolone in complete palsy)
- For confirmed Ramsay Hunt syndrome, use higher dose antivirals (double the Bell's palsy dose)
4. Surgical Decompression
- Not recommended - no evidence of benefit, and may be harmful
5. For Permanent Paralysis
- Cosmetic/reconstructive surgical procedures to restore facial symmetry
- Botulinum toxin injections for synkinesis
Recent Evidence (2023-2026)
Recent systematic reviews have explored adjunct therapies:
- Physical therapy meta-analysis (2024, PMID 37149416) examined exercise-based rehabilitation for peripheral facial palsy
- Laser therapy meta-analysis (2024, PMID 39546047) found some benefit of photobiomodulation/laser therapy as adjunct to standard care
- A meta-analysis on COVID-19 vaccines (2024, PMID 37433426) found a small but measurable increased incidence of Bell's palsy post-COVID vaccination, though the absolute risk remains very low
Sources: Harrison's Principles of Internal Medicine 22E (2025); Adams and Victor's Principles of Neurology, 12th Ed.; Goldman-Cecil Medicine; Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.