Captopril
Reading File
Finding Sources
Searching PubMed
captopril ACE inhibitor clinical pharmacology
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a thorough answer. Here is the complete summary:
Captopril
Overview
Captopril is the first orally active ACE (angiotensin-converting enzyme) inhibitor. It was developed in the 1970s by Ondetti, Cushman, and colleagues after studying the inhibitory action of teprotide - a nonapeptide from the venom of the Brazilian pit viper (Bothrops jararaca). It belongs to the sulfhydryl-containing class of ACE inhibitors and remains the prototype of the entire drug class.
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, p. 615
- Lippincott Illustrated Reviews: Pharmacology, p. 302
Mechanism of Action
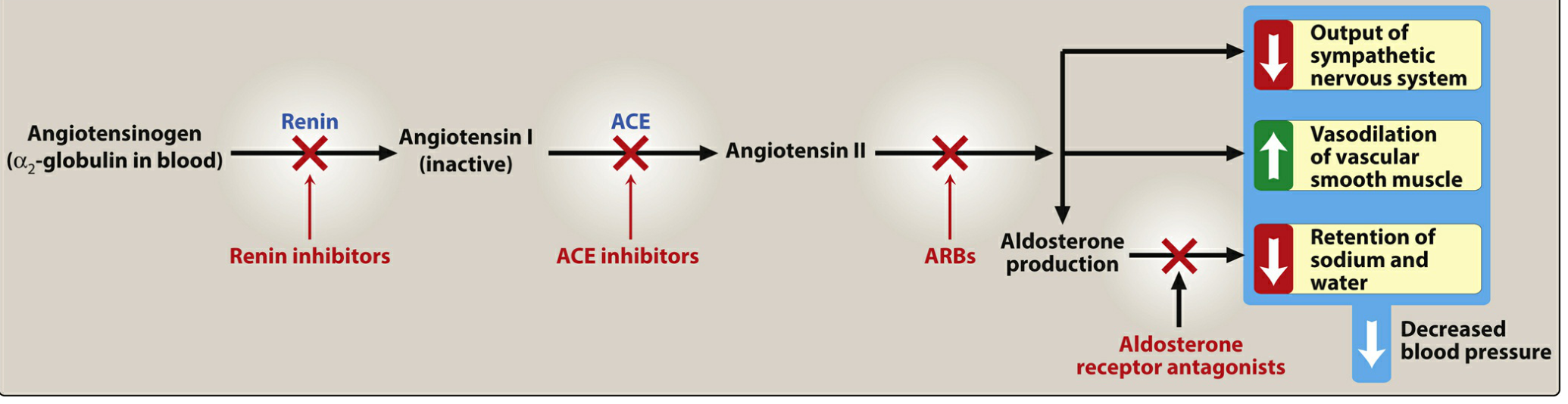
Captopril blocks ACE, which is a zinc-containing dipeptidyl carboxypeptidase (also known as kinase II). This has several consequences:
- Blocks AngI → AngII conversion - reduces circulating angiotensin II, decreasing vasoconstriction, aldosterone secretion, and sympathetic activation
- Inhibits bradykinin breakdown - ACE is the same enzyme that degrades bradykinin; its inhibition raises bradykinin levels, enhancing production of nitric oxide and prostacyclin (both vasodilators)
- Increases Ac-SDKP - a stem cell regulator with cardioprotective effects
- Increases renin and AngI - through disruption of negative feedback; excess AngI is shunted to vasodilator peptides such as Ang(1-7)
Net effect: vasodilation of both arterioles and veins, reduced preload and afterload, decreased Na+/water retention.
- Goodman & Gilman's, p. 616
- Lippincott Pharmacology, p. 302
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Class | Sulfhydryl-containing ACEI (not a prodrug - active as administered) |
| Bioavailability | ~75%, but reduced by 25-30% with food - should be taken on an empty stomach |
| Ki | 1.7 nM (highly potent) |
| Peak plasma level | ~1 hour after oral dose |
| Protein binding | ~30% |
| Half-life | ~2 hours (but prolonged in renal failure) |
| Elimination | Renal: 40-50% as unchanged captopril; remainder as captopril disulfide dimers and captopril-cysteine disulfide |
| Dose | 6.25 to 150 mg, 2-3 times daily |
| Prodrug? | No - captopril and lisinopril are the only ACEIs that do NOT require hepatic conversion; preferred in hepatic impairment |
- Goodman & Gilman's, p. 618
- Lippincott Pharmacology, p. 303
Therapeutic Uses
| Indication | Notes |
|---|---|
| Hypertension | First-line; reduces peripheral vascular resistance |
| Heart failure (HFrEF) | Reduces preload and afterload; first-line along with beta blockers |
| Post-MI | Improves ventricular remodeling; reduces mortality |
| Diabetic nephropathy | Slows progression, reduces albuminuria; efferent arteriolar dilation lowers intraglomerular pressure |
| Chronic kidney disease | First-line in hypertensive CKD patients |
| Left ventricular hypertrophy | Causes regression with chronic use |
| Cystinuria | Captopril's sulfhydryl group forms a captopril-cysteine disulfide, increasing cystine solubility ~200-fold |
| Primary aldosteronism diagnosis | Captopril suppression test: 25-50 mg orally; PAC measured afterward |
| Renovascular hypertension screening | Captopril-enhanced renography (80-95% sensitivity) |
- Lippincott Pharmacology, p. 302-303
- Brenner & Rector's The Kidney
- Campbell Walsh Wein Urology
Adverse Effects
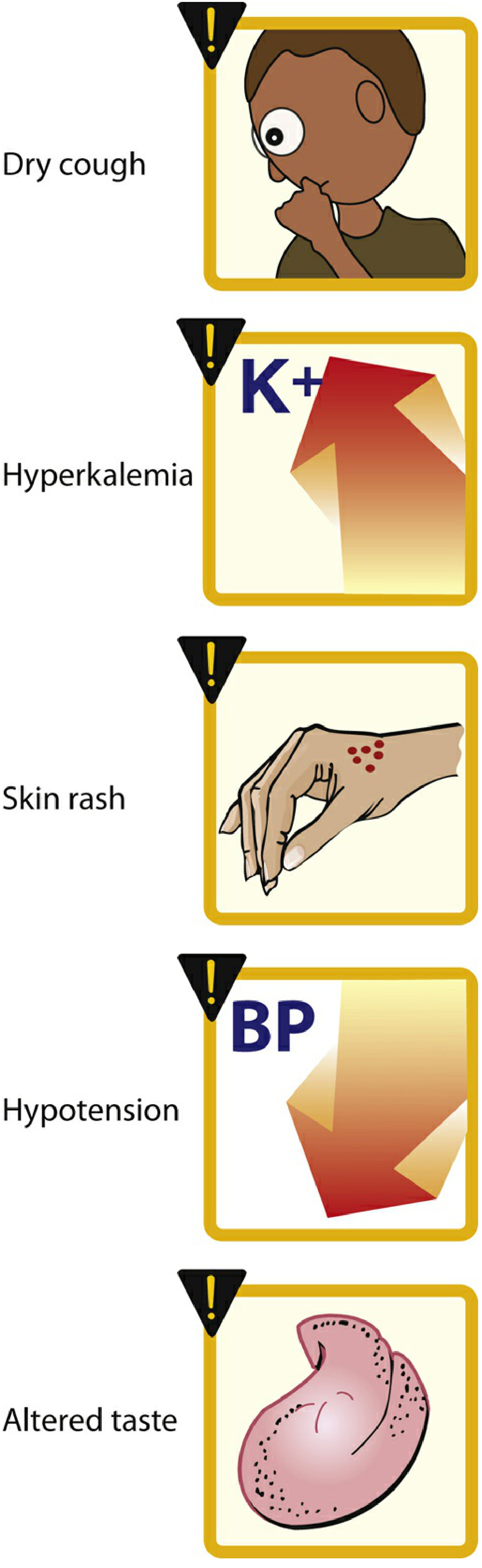
| Adverse Effect | Mechanism / Notes |
|---|---|
| Dry cough | Up to 10% of patients; from bradykinin and substance P accumulation in the pulmonary tree; more common in women; resolves within days of stopping |
| Angioedema | Rare but life-threatening; swelling of lips, oral mucosa, throat; bradykinin-mediated; more common in ACE inhibitors than ARBs |
| Hyperkalemia | Reduced aldosterone → reduced K+ excretion; avoid K+ supplements and K+-sparing diuretics |
| Hypotension | Especially "first-dose hypotension" - worse if volume-depleted or on diuretics |
| Altered taste (dysgeusia) | More specific to captopril than other ACEIs - attributed to the sulfhydryl group |
| Skin rash | Also relatively specific to captopril (sulfhydryl group) |
| Rise in serum creatinine | Up to 30% rise above baseline is acceptable; monitor renal function |
| Leukopenia | Rare |
| Teratogenicity | Fetal malformations (renal dysgenesis, skull ossification defects) - contraindicated in pregnancy |
- Lippincott Pharmacology, p. 303-304
- Washington Manual of Medical Therapeutics
Captopril-specific adverse effects (more than other ACEIs): taste disturbances and skin rash due to the sulfhydryl moiety. It is also less commonly used today because it requires 2-3 times daily dosing and causes more side effects than later-generation ACEIs. - Barash Clinical Anesthesia, p. 3255
Contraindications
- Pregnancy (all trimesters - teratogenic and fetotoxic)
- Bilateral renal artery stenosis (can cause acute renal failure by removing efferent tone)
- History of angioedema with any ACEI
- Concurrent use with aliskiren in diabetic patients
- Concurrent use with ARBs (increased adverse effects without added benefit for hypertension)
Drug Interactions
- Potassium supplements / K+-sparing diuretics (spironolactone, amiloride) - risk of hyperkalemia
- NSAIDs - blunt antihypertensive effect; worsen renal function
- Diuretics - potentiate hypotension (especially first-dose)
- Lithium - ACEIs reduce lithium excretion, raising lithium toxicity risk
Key Distinguishing Features vs. Other ACEIs
| Feature | Captopril | Others (e.g., enalapril, ramipril) |
|---|---|---|
| Active drug (not prodrug) | Yes | Most are prodrugs |
| Dosing frequency | 2-3x daily | Once daily (most) |
| IV form available | No | Enalaprilat only |
| Hepatic conversion needed | No | Yes (most) |
| Sulfhydryl group | Yes | No (dicarboxyl or phosphorus) |
| Taste/rash more common | Yes | Less so |
Summary Mnemonic - "CAPTOPRIL"
- C - Cough (dry, bradykinin-mediated)
- A - Angioedema
- P - Potassium rises (hyperkalemia)
- T - Teratogen (contraindicated in pregnancy)
- O - Output (cardiac) improved in HF
- P - Proteinuria reduced (diabetic nephropathy)
- R - Renal artery stenosis: use with caution
- I - Inhibits ACE (AngI → AngII blocked)
- L - Lowers BP (vasodilation, ↓ aldosterone)
This is a shared conversation. Sign in to Orris to start your own chat.