Sinus rythm with First degree av block predominently with 2:1 av block
Reading File
Finding Sources
Finding Sources
Searching Images
first degree AV block 2:1 AV block ECG rhythm strip
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of Sinus Rhythm with First-Degree AV Block and 2:1 AV Block, drawn from authoritative cardiology textbooks.
Sinus Rhythm with First-Degree AV Block + 2:1 AV Block
This ECG description implies a variable AV conduction pattern: at baseline, there is first-degree AV block (prolonged PR interval, all beats conducted), but predominantly there is a 2:1 AV conduction ratio (every other P wave is blocked, halving the ventricular rate).
First-Degree AV Block
Definition: A prolonged PR interval >200 ms, with every atrial impulse successfully conducted to the ventricles. Despite the name, nothing is "blocked" — it is a conduction delay, almost always within the AV node itself.
ECG features:
- PR interval > 200 ms (constant)
- Every P wave followed by a QRS complex
- QRS is typically narrow unless intraventricular conduction disease coexists
Clinical significance: Generally benign. Can be seen in:
- Normal healthy individuals, well-trained athletes (vagal tone)
- Inferior MI (AV nodal ischemia)
- Drug effects (beta-blockers, calcium channel blockers, digoxin, amiodarone)
- Inflammatory/infiltrative disease (myocarditis, sarcoidosis, Lyme disease)
"First-degree AV block is a misnomer because nothing is actually blocked; rather, there is delay, usually in the AV node, manifest by a prolonged PR interval." — Goldman-Cecil Medicine
2:1 AV Block
Definition: Every other P wave is non-conducted — 2 P waves for every 1 QRS complex. This is technically a form of second-degree AV block, but because there are never two consecutively conducted beats, it is impossible to distinguish Mobitz Type I (Wenckebach) from Mobitz Type II on ECG alone.
The critical clinical challenge with 2:1 AV block is determining the level of block:
| Feature | Nodal (proximal) — likely Wenckebach | Infranodal (distal) — likely Mobitz II |
|---|---|---|
| QRS morphology | Narrow | Wide (BBB pattern) |
| PR interval (conducted) | Prolonged | Normal or minimally prolonged |
| Response to atropine | Improves conduction | May worsen |
| Level on His bundle recording | AH interval prolonged | HV interval prolonged or H-V block |
| Clinical risk | Lower | Higher — risk of complete heart block |
"When 2:1 AV block is caused by a block distal to the bundle of His (type II), it has a more serious prognosis than if it is caused by a block proximal to the bundle of His." — Braunwald's Heart Disease
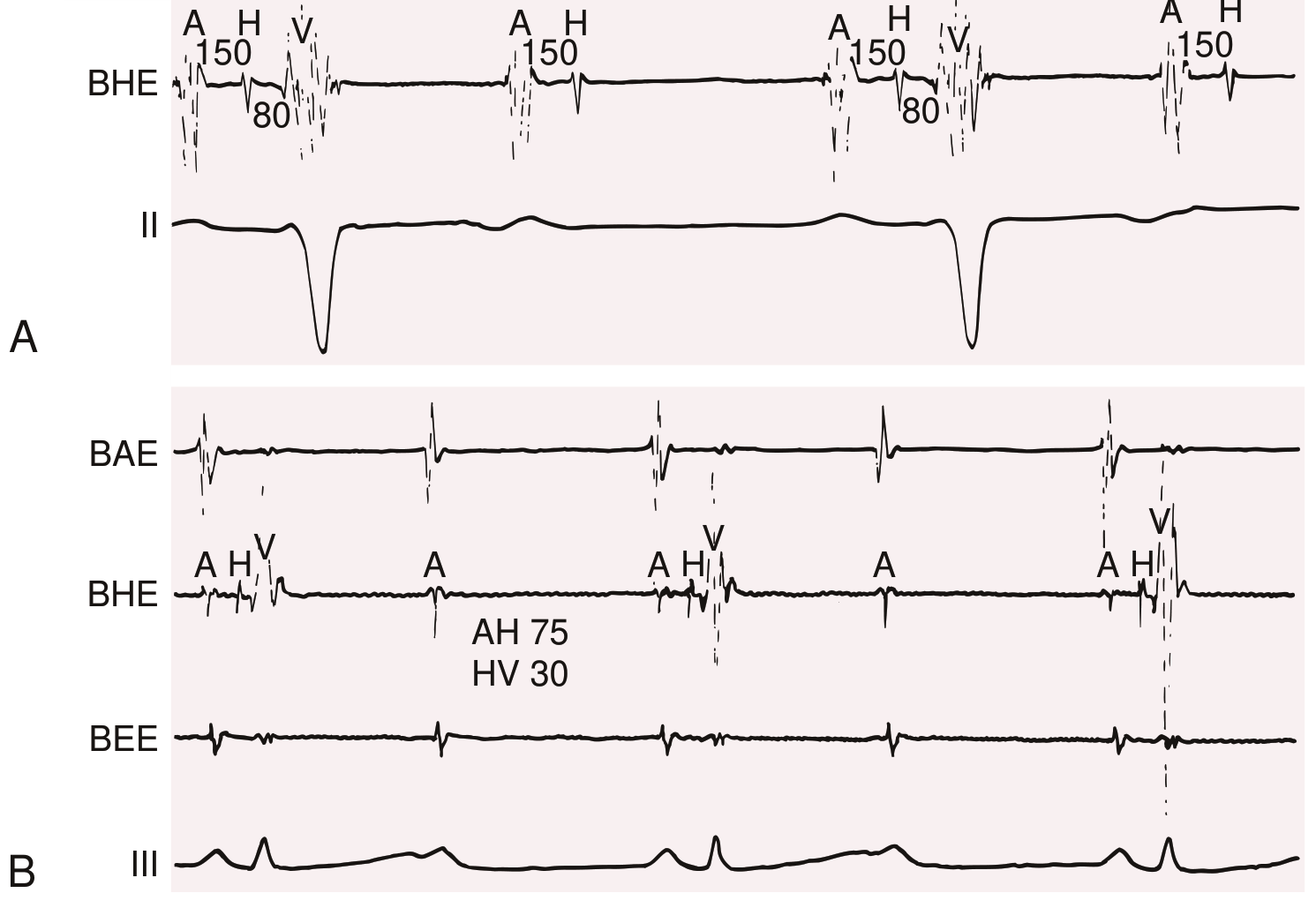
Fig: 2:1 AV block proximal vs. distal to the His bundle (Braunwald's Heart Disease). Panel A = infranodal 2:1 block with RBBB. Panel B = proximal/nodal 2:1 block with normal QRS.
Clinical Significance of the Combined Pattern
When first-degree AV block is present alongside 2:1 AV block, the conducted PR being prolonged is actually a clue: it favors the block being at the AV node level (Mobitz I / Wenckebach behavior), rather than infranodal (Mobitz II). Mobitz II tends to have a normal PR interval in the conducted beats.
However, the combination can also represent alternating conduction ratios or a transitioning conduction disorder, which warrants careful monitoring.
Etiologies to consider:
- Acute inferior MI (RCA supplies AV node in ~90% of people)
- Degenerative conduction system disease (Lev's or Lenègre's disease)
- Drug toxicity (digoxin, beta-blockers, CCBs)
- Hyperkalemia
- Inflammatory: myocarditis, Lyme carditis, sarcoidosis, rheumatic fever
- Post-cardiac surgery
ECG Recognition Tips

For 2:1 AV block on rhythm strip:
- Count 2 P waves per QRS — one conducted, one blocked
- Measure the PR interval of the conducted beat — prolonged = likely nodal; normal = likely infranodal
- Check QRS width — narrow = nodal; wide = infranodal until proven otherwise
- Compare with longer rhythm strips or Holter — catching 3:2 Wenckebach sequences would confirm Mobitz I
Management
First-degree AV block alone: No treatment required. Monitor and address reversible causes (drugs, electrolytes, ischemia).
2:1 AV block:
- Asymptomatic + likely nodal: Monitor, treat underlying cause, avoid AV-blocking drugs
- Symptomatic (syncope, presyncope, hemodynamic compromise): Urgent evaluation; atropine (if nodal), temporary pacing if needed
- Infranodal 2:1 block: High risk of progression to complete heart block → permanent pacemaker indicated (Class I indication per guidelines)
- Acute inferior MI: Usually transient, resolves with reperfusion; temporary pacing if symptomatic
- Acute anterior MI with 2:1 block: More ominous — often infranodal, high risk of CHB
"When 2:1 AV block is associated with a bundle branch block, the block is more likely to be distal to the bundle of His, and a permanent pacemaker is often indicated." — Braunwald's Heart Disease
Bottom line: The coexistence of first-degree AV block and predominantly 2:1 AV block suggests significant AV conduction disease. The key decision point is localizing the block (nodal vs. infranodal) via QRS width and PR interval analysis — and in many cases, electrophysiology study. Symptomatic patients or those with evidence of infranodal block need pacemaker evaluation.
— Braunwald's Heart Disease (9780323722193), pp. 574–582; Goldman-Cecil Medicine (9780323930345); Fuster and Hurst's The Heart, 15th Ed.
Approach and treatment strategy
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a structured approach and treatment strategy for sinus rhythm with first-degree AV block and predominant 2:1 AV block.
Approach & Treatment Strategy
Step 1 — Immediate Clinical Assessment
Assess hemodynamic stability first:
- Is the patient symptomatic? (syncope, presyncope, dizziness, fatigue, dyspnea, chest pain)
- What is the ventricular rate? (2:1 block halves the effective rate — if sinus rate is 80 bpm, ventricular rate is ~40 bpm → likely symptomatic)
- Blood pressure, perfusion, mental status
"Persistent 2:1 AV block can produce symptoms of chronic bradycardia. Complete AV block can be accompanied by signs and symptoms of reduced cardiac output, syncope or presyncope, angina, or palpitations." — Braunwald's Heart Disease
Step 2 — Localize the Level of Block (Critical Decision Point)
This determines urgency, prognosis, and whether a pacemaker is needed.
| ECG Clue | Favors Nodal (AV node) | Favors Infranodal (His-Purkinje) |
|---|---|---|
| PR interval (conducted beat) | Markedly prolonged (>300 ms) | Normal or mildly prolonged |
| QRS duration | Narrow (<120 ms) | Wide (BBB morphology) |
| Response to atropine | Improves conduction ratio | May worsen (increases sinus rate, more P waves blocked) |
| Response to exercise | Improves | Worsens |
| Coexisting first-degree AV block | Supports nodal level | Less typical of pure infranodal |
In this patient, the coexistence of first-degree AV block (prolonged PR on conducted beats) favors a nodal location, but this cannot be assumed if QRS is wide.
Step 3 — Identify and Treat Reversible Causes
Always look for and remove precipitants before deciding on pacing:
| Category | Examples |
|---|---|
| Drugs | Beta-blockers, CCBs (diltiazem/verapamil), digoxin, amiodarone, ivabradine |
| Electrolyte | Hyperkalemia |
| Ischemia | Acute inferior MI (RCA → AV node), anterior MI (infranodal) |
| Inflammatory | Lyme carditis, myocarditis, sarcoidosis, rheumatic fever |
| Infiltrative | Amyloidosis, hemochromatosis |
| Degenerative | Lev's or Lenègre's disease (fibrosis of conduction system) |
| Post-surgical | After cardiac or valve surgery |
| Vagal/autonomic | Athletes, sleep, vasovagal |
"The treatment of AV blocks consists of first removing any medications that may precipitate dysfunction. Although some patients will recover normal conduction, the susceptibility to medications usually indicates an underlying conduction abnormality that may worsen over time." — Goldman-Cecil Medicine
Special case — Lyme carditis: Most AV block resolves within 1 week of IV antibiotics (ceftriaxone). Temporary pacing may bridge the acute phase. This is the one exception where permanent pacing is usually not needed.
Step 4 — Acute / Emergency Management
For hemodynamically unstable or symptomatic patients:
-
IV Atropine 0.5–1 mg (repeat to max 3 mg)
- Effective for nodal block (increases AV node conduction)
- May paradoxically worsen infranodal block (accelerates sinus rate → more P waves blocked)
-
IV Isoproterenol (1–2 μg/min infusion)
- Increases conduction at any level
- Use with extreme caution in acute MI (pro-arrhythmic)
-
Transcutaneous pacing — immediate bridge when drugs fail or infranodal block suspected
-
Temporary transvenous pacing — definitive bridge while awaiting permanent pacemaker or resolving reversible cause
Step 5 — Investigations
| Investigation | Purpose |
|---|---|
| 12-lead ECG + long rhythm strip | QRS width, PR interval, P:QRS ratio |
| Holter / prolonged monitoring | Catch 3:2 Wenckebach sequences (confirms Mobitz I), document progression |
| Electrolytes (K+, Mg++) | Reversible causes |
| Drug levels (digoxin) | Toxicity |
| Troponin / ECG for STEMI | Acute ischemia |
| Lyme serology | In endemic areas |
| ANA, ACE level | Autoimmune / sarcoidosis |
| Electrophysiology study (EPS) | If uncertain — measures HV interval directly; HV ≥100 ms → high risk infranodal block |
| Echocardiogram | Structural disease, LV function (impacts pacemaker type selection) |
"In patients with presyncope or syncope, one should suspect intermittent infrahisian block in those with BBB or an intraventricular conduction defect. An EPS to evaluate AV conduction thoroughly may be warranted." — Braunwald's Heart Disease
Step 6 — Permanent Pacemaker Decision
Class I Indications (Pacemaker IS indicated):
- Symptomatic second-degree AV block at any level (syncope, presyncope, heart failure, bradycardia symptoms)
- Asymptomatic infranodal (His or below) 2:1 block
- Second-degree/advanced AV block with associated BBB (infranodal presumed)
- Second-degree AV block in the setting of neuromuscular disease (myotonic dystrophy, Kearns-Sayre)
- Post-operative AV block not expected to resolve
- Post-MI: persistent symptomatic block, or transient infranodal block with BBB
Class IIa Indications (Pacemaker is Reasonable):
- Asymptomatic Mobitz II with narrow QRS
- Asymptomatic infranodal second-degree AV block
- First- or second-degree AV block with symptoms resembling pacemaker syndrome (fatigue, dyspnea from loss of AV synchrony)
Pacemaker Mode Selection:
| Situation | Preferred Mode |
|---|---|
| AV block with intact sinus node (as in this patient) | DDD (dual-chamber — tracks P waves, maintains AV synchrony) |
| Permanent AF + AV block | VVI or leadless RV pacemaker |
| AV block + LV dysfunction (EF <35–40%) | Biventricular (CRT) or His/left bundle branch pacing to prevent RV pacing-induced cardiomyopathy |
"There is growing evidence that some patients with AV block, especially those with preexisting LV dysfunction, may benefit from biventricular pacing rather than right ventricle-only pacing to prevent development or progression of heart failure." — Braunwald's Heart Disease
Summary Algorithm
Sinus rhythm + 1° AVB + predominant 2:1 AV block
↓
Hemodynamically unstable?
YES → Atropine → Transcutaneous pacing → Transvenous pacing
NO ↓
Remove reversible causes (drugs, electrolytes, ischemia, infection)
↓
Localize block: QRS width + PR of conducted beat
↙ Narrow QRS / long PR ↘ Wide QRS / normal PR
Likely nodal (Mobitz I) Likely infranodal (Mobitz II)
Monitor; treat cause → EPS or proceed to PPM
↓
Persistent block + symptoms → PERMANENT PACEMAKER (DDD)
Asymptomatic infranodal block → PERMANENT PACEMAKER (Class I)
Asymptomatic nodal block, reversible cause resolved → Monitor
Key principle: Sinus rhythm is preserved in this patient, making a DDD pacemaker ideal — it will sense atrial activity and pace the ventricle after the appropriate AV delay, restoring physiologic AV synchrony. His-bundle or left bundle branch pacing is increasingly preferred over right ventricular apical pacing to maintain ventricular synchrony.
— Braunwald's Heart Disease (9780323722193), pp. 580–588; Goldman-Cecil Medicine (9780323930345), pp. 563–566; Goldman-Cecil Medicine Table 54-1 & 54-2 Pacemaker Indications
This is a shared conversation. Sign in to Orris to start your own chat.