Nephritic syndrome
Reading File
Finding Sources
Finding Sources
Searching PubMed
"nephritic syndrome"[MeSH Terms] AND glomerulonephritis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have excellent material from multiple authoritative textbooks to compose a comprehensive answer. Let me compile everything into a well-structured response.
Nephritic Syndrome
Definition
Nephritic syndrome is defined as the presence of glomerular hematuria (dysmorphic red blood cells or RBC casts), combined with hypertension, edema, reduced GFR (with or without oliguria), and non-nephrotic-range proteinuria - all resulting from glomerular inflammation.
- National Kidneys Foundation Primer on Kidney Diseases, 8e, p. 3046
Pathophysiology
The underlying mechanism is glomerular inflammation causing:
-
Injury to the capillary wall, allowing blood cells to leak into the urinary space (hematuria)
-
Proliferation of glomerular cells + infiltration of inflammatory leukocytes
-
Reduced GFR from severe capillary wall injury → oliguria, fluid retention, azotemia
-
Hypertension from both fluid retention and renin release from ischemic kidneys
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 3064
Clinical Features (The Classic Tetrad)
| Feature | Details |
|---|---|
| Hematuria | RBCs + RBC casts in urine; urine appears brown/smoky (not bright red, no clots) |
| Proteinuria | Subnephrotic range (< 3.5 g/day); serum albumin usually normal |
| Hypertension | From fluid retention + renin release |
| Azotemia | Oliguria, weight gain, edema from reduced GFR |
Nephritic vs. Nephrotic Syndrome
| Feature | Nephrotic | Nephritic |
|---|---|---|
| Onset | Insidious | Abrupt |
| Edema | ++++ (massive) | ++ (mild-moderate) |
| Blood pressure | Normal | Raised |
| JVP | Normal/low | Raised |
| Proteinuria | ++++ (> 3.5 g/day) | ++ (subnephrotic) |
| Hematuria | May/may not occur | +++ |
| RBC casts | Absent | Present |
| Serum albumin | Low | Normal/slightly reduced |
- Comprehensive Clinical Nephrology, 7th Edition, Table 16.4
Causes / Etiologic Classification
Diseases presenting with nephritic syndrome are classified by immunopathologic mechanism:
1. Immune Complex-Mediated
- Postinfectious GN (post-streptococcal) - prototypical; caused by group A beta-hemolytic streptococci types 1, 4, 12; latency of 1-4 weeks after throat/skin infection; subepithelial "humps" on EM
- IgA Nephropathy - most common primary glomerulopathy worldwide; mesangial IgA deposits; triggered by upper respiratory infections (synpharyngitic hematuria)
- Lupus Nephritis (SLE) - proliferative forms (Class III/IV)
- Cryoglobulinemia
- Endocarditis-associated GN
- Membranoproliferative GN (can present as mixed nephritic/nephrotic)
2. Pauci-Immune / ANCA-Associated
- Granulomatosis with Polyangiitis (GPA) (c-ANCA/PR3)
- Microscopic Polyangiitis (p-ANCA/MPO)
- Eosinophilic Granulomatosis with Polyangiitis (EGPA)
- Absent or sparse immune deposits on IF
3. Anti-GBM Antibody-Mediated
- Goodpasture Syndrome - antibodies to the NC1 domain of the alpha-3 chain of type IV collagen; linear IgG on IF; two age peaks (3rd decade males; >60 females); pulmonary hemorrhage + nephritis
4. Complement-Mediated
-
C3 Glomerulopathy (C3 GN, dense deposit disease)
-
National Kidneys Foundation Primer on Kidney Diseases, 8e, p. 3046; Goldman-Cecil Medicine, p. 2684
Serum Complement Levels - Key Diagnostic Clue
| Complement Status | Diseases |
|---|---|
| Reduced C3/C4 | Post-streptococcal GN, SLE, Cryoglobulinemia, C3 glomerulopathies, Endocarditis, Shunt infections |
| Normal complement | IgA nephropathy / HSP, Anti-GBM disease, Pauci-immune RPGN (ANCA-associated) |
- Goldman-Cecil Medicine, Table 107-4
Rapidly Progressive GN (RPGN) - The Emergency Form
RPGN (crescentic GN) is a clinicopathologic syndrome defined by rapid loss of kidney function over days to weeks in the context of nephritic syndrome - a uremic emergency.
Histology: Extensive crescent formation in Bowman's space (proliferation of parietal epithelial cells + monocytes/macrophages), compressing the glomerular tuft.
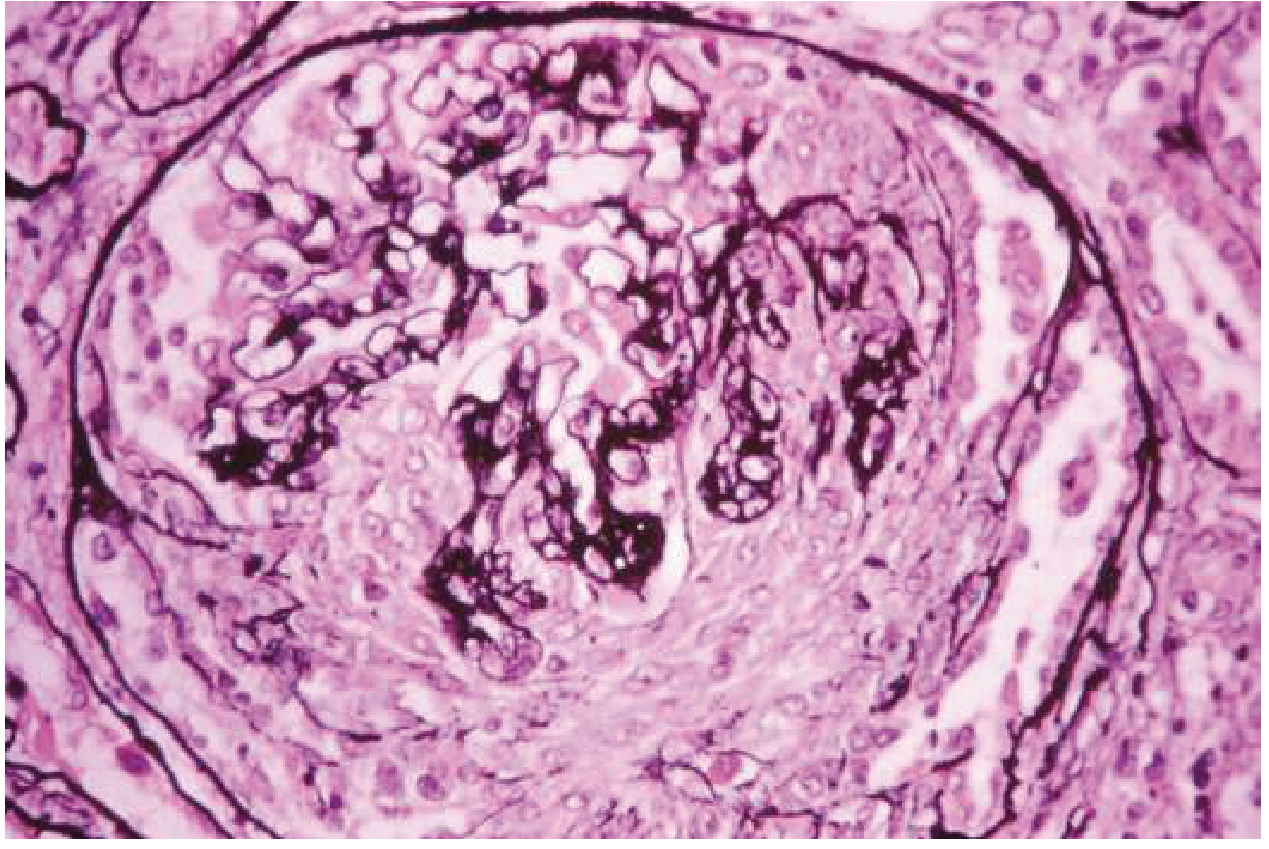
Crescentic GN: Proliferation of cells in Bowman's space forming a crescent, compressing the glomerular tuft. (Goldman-Cecil Medicine, Fig. 107-10)
Three pathogenic types of RPGN:
| Type | Mechanism | IF Pattern | Serology |
|---|---|---|---|
| Type I | Anti-GBM antibodies | Linear IgG + C3 | Anti-GBM Ab positive |
| Type II | Immune complex-mediated | Granular IgG/IgA + C3 | Low complement; various serologies (ANA, ASLO, etc.) |
| Type III | Pauci-immune / ANCA | No/minimal deposits | c-ANCA or p-ANCA positive |
- Goldman-Cecil Medicine, p. 2987; Robbins, Cotran & Kumar, p. 3199
Pathology Summary of Key Nephritic Diseases
| Disease | Light Microscopy | Immunofluorescence | Electron Microscopy |
|---|---|---|---|
| Post-infectious GN | Diffuse endocapillary proliferation + neutrophils | Granular IgG + C3 (GBM + mesangium) | Subepithelial "humps"; subendothelial deposits early |
| Crescentic GN (anti-GBM) | Crescents; fibrinoid necrosis | Linear IgG + C3 | No deposits |
| Crescentic GN (ANCA) | Crescents; necrosis; pauci-immune | No/minimal deposits | No deposits |
| Crescentic GN (immune complex) | Crescents; necrosis | Granular IgG; various | Immune complexes at various locations |
| IgA Nephropathy | Mesangial proliferation (MEST-C) | Mesangial IgA | Mesangial electron-dense deposits |
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Table 20.5
Post-Streptococcal GN - Prototypical Case
- Who: Children 6-10 years most commonly; 1-4 weeks after strep pharyngitis or impetigo
- Organism: Group A beta-hemolytic strep; nephritogenic strains (M types 1, 4, 12); principal antigen = streptococcal pyogenic exotoxin B (SpeB)
- Labs: Low serum complement (C3), elevated ASO titer (for pharyngitis) or anti-DNase B (for skin infections)
- UA: Brown urine, RBCs, RBC casts, subnephrotic proteinuria
- Course: Most children recover; prognosis worse in adults
- EM Hallmark: Subepithelial "hump-like" immune complex deposits
IgA Nephropathy - Most Common Primary GN Worldwide
- Pathogenesis: Deposition of galactose-deficient IgA1 immune complexes in the mesangium
- Presentation: Episodic macroscopic hematuria coinciding with URI (synpharyngitic, within 1-2 days - much shorter latency than post-streptococcal)
- MEST-C score on biopsy: Mesangial proliferation (M), Endocapillary proliferation (E), Segmental sclerosis (S), Tubulo-interstitial fibrosis (T), Crescents (C)
- Complement: Normal
- Prognosis: ~60% benign course; ~40% progress to kidney failure over 10-20 years
- Can manifest systemically as IgA vasculitis (Henoch-Schonlein Purpura) with skin, joint, and intestinal involvement
Anti-GBM Disease (Goodpasture Syndrome)
- Antibodies against NC1 domain of alpha-3 chain of type IV collagen
- IF: Linear IgG + C3 along GBM (pathognomonic)
- When pulmonary capillary basement membranes are also involved: pulmonary hemorrhage + nephritis = Goodpasture syndrome
- Rapidly progresses to dialysis-requiring renal failure within days to weeks
- Complement: Normal
Diagnosis Workup
Urinalysis: Dysmorphic RBCs, RBC casts (hallmark), subnephrotic proteinuria
Serologic panel:
- ASO titer / anti-DNase B (post-streptococcal)
- ANA, anti-dsDNA, complement C3/C4 (SLE)
- ANCA (c-ANCA/PR3, p-ANCA/MPO) for pauci-immune RPGN
- Anti-GBM antibodies
- Cryoglobulins, hepatitis B/C serology
- Serum complement (C3, C4, CH50)
Kidney biopsy - often required for definitive diagnosis and classification
- Comprehensive Clinical Nephrology, 7th Edition, Table 16.5
Treatment Principles
| Disease | First-Line Treatment |
|---|---|
| Post-streptococcal GN | Supportive (antibiotics for active infection, antihypertensives, diuretics); most self-limited |
| IgA Nephropathy | ACEi/ARB (first line); SGLT-2 inhibitors (emerging); immunosuppression in high-risk cases |
| ANCA-associated RPGN | High-dose corticosteroids + cyclophosphamide or rituximab; plasma exchange in severe cases |
| Anti-GBM disease | Urgent plasma exchange + corticosteroids + cyclophosphamide |
| Lupus nephritis (proliferative) | Corticosteroids + mycophenolate mofetil or cyclophosphamide |
Key Points to Remember
- Hallmark: RBC casts in urine (pathognomonic of glomerulonephritis)
- Mechanism: Glomerular inflammation - distinct from nephrotic syndrome's barrier permeability defect
- Complement low: Post-streptococcal, SLE, cryoglobulinemia, C3 GN
- Complement normal: IgA nephropathy, anti-GBM, pauci-immune (ANCA)
- RPGN = emergency: Crescents on biopsy; treat urgently to preserve kidney function
- Post-streptococcal vs. IgA: Latency distinguishes them - weeks after strep vs. days during URI
- Goodpasture: Linear IF + pulmonary hemorrhage = anti-GBM disease
This is a shared conversation. Sign in to Orris to start your own chat.