Gastrointestinal malformations. Congenital high intestinal obstruction. Congenital pyloric stenosis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Congenital high intestinal obstruction. Congenital pyloric stenosis
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive, well-illustrated answer. Let me compose it.
Congenital High Intestinal Obstruction & Congenital Pyloric Stenosis
Part I — Congenital High Intestinal Obstruction
"High" intestinal obstruction refers to obstruction at or above the proximal jejunum — primarily the duodenum, but also including obstruction at the gastric outlet. The main causes are duodenal atresia/stenosis, annular pancreas, and jejunal atresia.
1. Duodenal Atresia & Stenosis
Embryology & Pathogenesis
During the 5th–6th weeks of development the duodenal lumen is completely occluded by proliferating epithelial cells; normal recanalization follows. Failure of recanalization produces a short segment of complete occlusion (atresia) or incomplete obstruction (stenosis/mucosal web). The blockage most often involves the second portion of the duodenum at or near the hepatopancreatic ampulla; less commonly the horizontal (third) part is affected. Familial cases follow an autosomal recessive inheritance pattern.
— The Developing Human: Clinically Oriented Embryology
Anatomic Variants (spectrum)
| Type | Morphology |
|---|---|
| Stenosis | Narrowed lumen, muscle wall intact |
| Mucosal web ("windsock") | Intact muscle wall; intraluminal diaphragm, sometimes ballooning distally |
| Fibrous cord | Two blind ends connected by a fibrous cord |
| Complete gap atresia | Two blind ends with a mesenteric gap |
In 85% of cases the obstruction is distal to the ampulla of Vater, so vomiting is bilious. Proximal (pre-ampullary) obstruction produces non-bilious vomiting — important: the presence of non-bilious emesis does not exclude duodenal atresia.
— Sabiston Textbook of Surgery, 21e
Associated Conditions
- Down syndrome (trisomy 21) — ~30% of cases
- Prematurity (~20%)
- Annular pancreas
- Maternal polyhydramnios (duodenal obstruction prevents normal absorption of swallowed amniotic fluid)
- Malrotation, preduodenal portal vein, biliary atresia
- Cardiac, renal, and anorectal malformations
— The Developing Human; Sabiston
Clinical Presentation
- Antenatal: polyhydramnios on maternal ultrasound; double-bubble sign may be seen in utero
- Postnatal: bilious vomiting within hours of birth; epigastric distension (distended stomach + proximal duodenum); failure to pass meconium normally
Diagnosis
The pathognomonic radiographic finding is the "double-bubble" sign — two gas-filled, fluid-filled chambers representing the distended stomach and the proximal duodenum, with no gas beyond the obstruction.

- If distal gas is present, an upper GI contrast study should be performed to exclude malrotation with midgut volvulus (a surgical emergency)
- Prenatal ultrasound shows fluid-filled double-bubble in the fetal abdomen
Treatment
- Nasogastric/orogastric decompression; IV fluid resuscitation
- Definitive surgery: bypass of the obstruction — side-to-side or diamond-shaped (proximal transverse-to-distal longitudinal) duodenoduodenostomy
- Laparoscopic approach increasingly performed
- If proximal duodenum is markedly dilated: tapering duodenoplasty to reduce dysmotility
- For mucosal web: web fenestration or excision transduodenally (caution to protect the ampulla)
— Sabiston Textbook of Surgery
2. Jejunoileal Atresia
The most common GI atresia, occurring in 1 in 2000 live births. Unlike duodenal atresia (failure of recanalization), jejunoileal atresia results from an intrauterine mesenteric vascular accident (not a recanalization failure), causing ischemic necrosis of a bowel segment.
Classification (Grosfeld Types)
| Type | Description |
|---|---|
| I | Mucosal web/diaphragm; intact muscle and mesentery |
| II | Atretic cord between blind ends; intact mesentery |
| IIIa | Complete separation; V-shaped mesenteric gap |
| IIIb | "Apple-peel" / "Christmas tree" — large mesenteric gap; surviving bowel spirals around marginal artery |
| IV | Multiple atresias ("string of sausages") |
Clinical Features
- Bilious vomiting, abdominal distension, failure to pass meconium
- Proximal atresias: prominent bilious emesis
- Distal atresias: abdominal distension with multiple dilated loops
- Contrast enema shows microcolon (unused, small caliber colon)
- Multiple atresias occur in 10–15% — distal bowel must be checked intraoperatively (saline injection via catheter)
- Associated with cystic fibrosis (~10%) — the only significant systemic association
Treatment
Surgical resection and primary anastomosis; always inspect entire bowel for additional atretic segments.
— Sabiston Textbook of Surgery, 21e
3. Annular Pancreas (as a cause of high obstruction)
A ring of pancreatic tissue encircles the second portion of the duodenum, causing extrinsic obstruction. Associated with duodenal atresia. Management: duodenoduodenostomy or duodenojejunostomy — the pancreatic ring is never divided (risk of pancreatitis and fistula).
Part II — Congenital Pyloric Stenosis (Infantile Hypertrophic Pyloric Stenosis)
Definition & Incidence
Infantile hypertrophic pyloric stenosis (HPS) is hypertrophy and hyperplasia of the pyloric muscularis propria (predominantly the circular muscle), producing progressive gastric outlet obstruction.
- Incidence: 1 in 300–900 live births (~0.2% of the general population)
- Male predominance: 4–5:1 (males affected more); first-born males at highest risk
- Typical presentation age: 2–8 weeks (range 3–12 weeks); rare after 12 weeks
- Siblings of affected patients: incidence rises to ~6%
— Schwartz's Principles of Surgery, 11e; Robbins Pathologic Basis of Disease
Pathology
Hyperplasia of the pyloric muscularis propria causes outward bulging and narrowing of the pyloric channel; mucosal and submucosal edema and inflammation may worsen the obstruction. The circular muscle is predominantly affected, with lesser involvement of the longitudinal muscle. Deficiency of nitric oxide synthase in pyloric tissue has been implicated in pathogenesis (loss of relaxation).
— Sabiston; Robbins
Etiology & Genetics
- Exact cause remains unknown
- High concordance in monozygotic twins; risk increased in dizygotic twins and siblings → strong familial/genetic component
- GWAS identified a locus at chromosome 11q23.3 (linked to cholesterol regulation)
- Turner syndrome and trisomy 18 confer increased risk
- Erythromycin or azithromycin exposure in the first 2 weeks of life (oral or via breast milk) is associated — macrolides are motilin receptor agonists, promoting excessive antral contractions
— Robbins; Schwartz's
Clinical Presentation
| Feature | Detail |
|---|---|
| Age at onset | 3–6 weeks (can be 2–12 weeks) |
| Vomiting | Progressive, forceful, projectile, non-bilious (obstruction is proximal to ampulla) |
| Feeding behavior | Infant vomits, then is immediately hungry again ("hungry vomiter") |
| Gastric peristalsis | Visible wave L→R across upper abdomen before vomiting (left upper quadrant to epigastrium) |
| Abdominal mass | Palpable "olive" — firm, ovoid, 1–2 cm mass in epigastrium / right upper quadrant; present in up to 90%; pathognomonic when felt |
| Dehydration | Progressive — decreased wet diapers, lethargy |
| Jaundice | Indirect hyperbilirubinemia (indirect) in some infants — mechanism unclear |
Metabolic Consequences
Repeated vomiting of gastric HCl causes:
Hypochloremic, hypokalemic metabolic alkalosis
- Loss of H⁺ and Cl⁻ → metabolic alkalosis + hypochloremia
- Kidneys initially excrete alkaline urine (high pH)
- As hypochloremia worsens, H⁺ is preferentially exchanged for Na⁺ in the distal tubule → paradoxical aciduria (urine becomes acidic despite systemic alkalosis)
- Low CO₂ from respiratory compensation: if anaesthesia is induced before correction, postoperative apnoea can occur due to absent CO₂ respiratory drive
Pre-operative targets before surgery:
- Serum bicarbonate < 30 mEq/L
- Serum chloride > 95 mEq/L
- Adequate urine output > 2 mL/kg/hr
— Schwartz's Principles of Surgery; Sabiston
Diagnosis
Ultrasound — first-line investigation (diagnostic accuracy ~95%):
- Pyloric muscle thickness > 3–4 mm
- Pyloric channel length > 15–18 mm
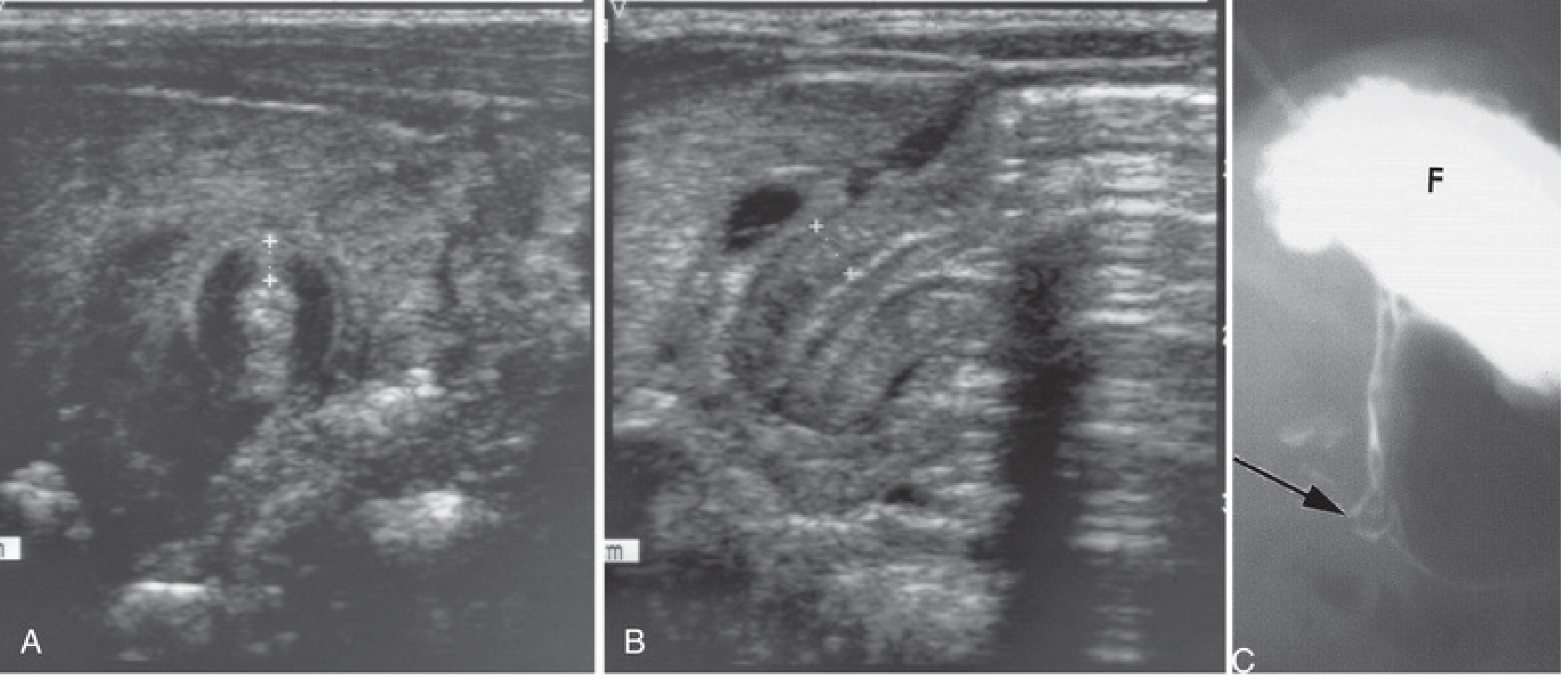
- If the "olive" is confidently palpated, no imaging is required
- Upper GI contrast study (used with caution — aspiration risk): delayed/absent passage of contrast through the pylorus; "string sign" or "beak sign" of the elongated, narrowed pyloric channel; used when ultrasound is equivocal or to exclude malrotation
Plain AXR: enlarged gastric gas bubble (gastric distension).
Treatment
Pyloric stenosis is NEVER a surgical emergency.
Correct the metabolic derangement first:
- IV fluids: 20 mL/kg NS bolus; then D5 ½ NS + 20 mEq/L KCl at 1.5× maintenance until urine output established
- Nasogastric tube decompression
- Correct hypochloraemic alkalosis to safe targets before GA
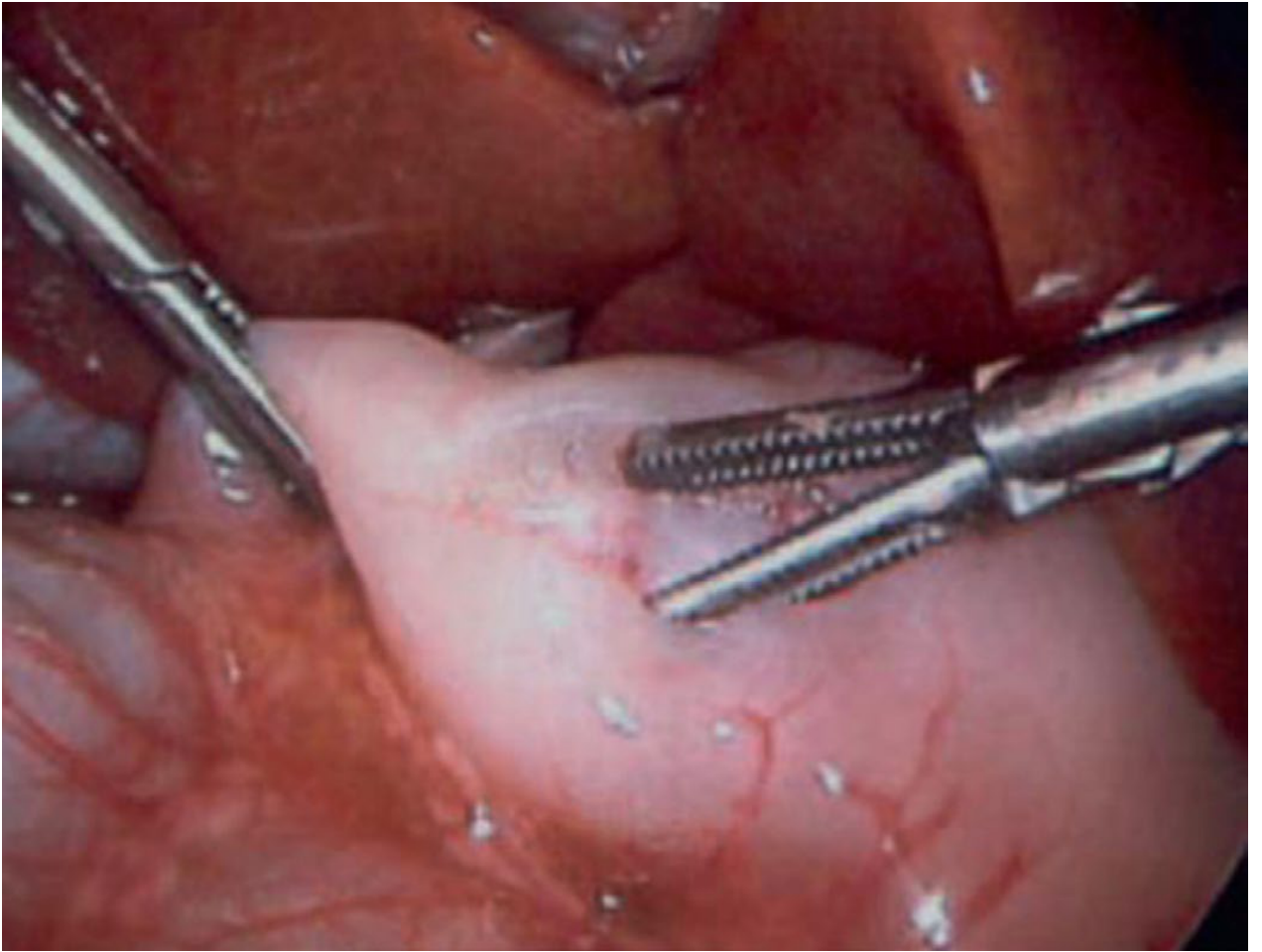
Definitive surgery — Fredet-Ramstedt Pyloromyotomy:
- Longitudinal incision through the hypertrophied pyloric muscle (serosa down to submucosa) — does not enter the mucosa
- Key endpoint: bulging mucosa throughout the length of the incision + independent wall motion of the two muscle edges
- Mucosal perforation must be excluded by injecting air via nasogastric tube
- Approaches: laparoscopic (preferred — shorter stay, lower wound infection rate) or open (umbilical or right upper quadrant transverse incision)
Postoperatively, infants are started on an oral feeding protocol and typically discharged within 24–48 hours. Surgical splitting of the hypertrophied muscularis is generally curative.
— Schwartz's Principles of Surgery, 11e; Sabiston Textbook of Surgery, 21e; Robbins Pathologic Basis of Disease
Summary Comparison
| Feature | Pyloric Stenosis | Duodenal Atresia | Jejunoileal Atresia |
|---|---|---|---|
| Obstruction level | Gastric outlet (pylorus) | 2nd duodenum (post-ampullary 85%) | Jejunum/ileum |
| Vomiting | Non-bilious, projectile | Bilious (usually) | Bilious |
| Onset | 3–6 weeks of life | Hours after birth | Hours after birth |
| Pathogenesis | Muscular hypertrophy | Failed recanalization | Intrauterine vascular accident |
| Key association | First-born males; macrolide exposure | Down syndrome (30%) | Cystic fibrosis (~10%) |
| Imaging sign | Pyloric "olive"; US thick muscle | "Double-bubble" | Microcolon on contrast enema |
| Metabolic effect | Hypochloraemic hypokalaemic alkalosis | Dehydration/alkalosis | Dehydration |
| Surgery | Pyloromyotomy (Fredet-Ramstedt) | Duodenoduodenostomy | Resection + anastomosis |
Esophageal atresia,Congenital high intestinal obstruction. Congenital pyloric stenosis , diaphragmatic hernia Need everything for pediatric surgery
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
The complete pediatric surgery reference is above. Here's what's covered for each condition:
What's Included
1. Esophageal Atresia / TEF
- Embryology (4th week foregut division failure)
- Full Gross-Vogt classification with incidence diagram (Type C = 86%)
- VACTERL associations
- Clinical presentation + diagnostic algorithm
- Waterston classification
- Pre-operative management (Replogle tube, positioning, avoid PPV)
- Surgical repair (primary anastomosis, long-gap strategies, thoracoscopy)
- All complications (stricture, recurrent TEF, GOR, tracheomalacia)
2. Congenital High Intestinal Obstruction
- Duodenal atresia: failed recanalization, double-bubble sign (X-ray shown), Down syndrome association, diamond duodenoduodenostomy
- Jejunoileal atresia: vascular accident pathogenesis, Grosfeld types I–IV including apple-peel (Type IIIb), cystic fibrosis association, microcolon
- Annular pancreas: never divide the ring
3. Congenital Pyloric Stenosis
- Pathology, risk factors, macrolide association
- "Hungry vomiter" clinical picture, palpable olive
- Hypochloraemic hypokalaemic metabolic alkalosis + paradoxical aciduria
- US criteria (muscle >3–4 mm, length >15–18 mm)
- Pre-op resuscitation targets + Fredet-Ramstedt pyloromyotomy (image shown)
4. Congenital Diaphragmatic Hernia (CDH)
- Bochdalek vs Morgagni; embryology
- Pulmonary hypoplasia + PPHN pathophysiology
- LHR / O/E LHR prognostic markers; FETO fetal intervention
- "Gentle ventilation" strategy, iNO, ECMO criteria
- Delayed surgery principle; patch vs primary repair; long-term outcomes
This is a shared conversation. Sign in to Orris to start your own chat.