Valsalva vs mullers maneuvere
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Now I have rich content from multiple authoritative sources. Let me compile the full comparison.
Valsalva vs. Muller's Maneuver
These two maneuvers are mirror images of each other - both involve a closed glottis but in opposite pressure directions.
The Basics
| Feature | Valsalva Maneuver | Muller's Maneuver |
|---|---|---|
| Action | Forced expiration against closed glottis | Forced inspiration against closed glottis |
| Intrathoracic pressure | Increases (positive pressure) | Decreases (negative pressure) |
| Venous return | Decreased | Increased |
| Memory trick | "V for out-Valve push" | Mirror of Valsalva |
Valsalva Maneuver - In Depth
Mechanism:
- Patient exhales forcefully against a closed glottis (or bears down as if defecating)
- Intrathoracic pressure rises sharply
- Venous return to the right heart decreases (compressed vena cava)
- Cardiac output falls -> preload drops
- As the maneuver is sustained, vagal tone increases -> SA and AV nodal conduction slow
Four Phases:
- Phase I (onset): Brief BP rise from aortic compression
- Phase II (strain): Decreased venous return -> drop in BP and cardiac output; reflex tachycardia
- Phase III (release): Sudden drop in BP as intrathoracic pressure normalizes
- Phase IV (overshoot): Rebound increase in venous return -> BP overshoot -> reflex bradycardia (vagal)
How to perform:
- Patient supine with cardiac monitor
- Take a deep breath, close lips around thumb (or blow into a syringe), and attempt to exhale without expelling air
- Bear down for 10-20 seconds, or passively raise legs simultaneously (modified Valsalva)
Clinical uses:
-
Terminating SVT - the vagal phase (Phase IV) slows AV nodal conduction. Mean success greatest with Valsalva + diving response among vagal maneuvers (Roberts & Hedges' Clinical Procedures in Emergency)
-
Diagnosing heart murmurs - by reducing preload:
- Most murmurs decrease in intensity and duration during Valsalva strain phase
- Two key exceptions that increase with Valsalva:
- HOCM (hypertrophic obstructive cardiomyopathy) - murmur becomes much louder because decreased preload worsens LV outflow tract obstruction
- MVP (mitral valve prolapse) - click and murmur move earlier and often become louder (leaflets prolapse sooner with smaller LV volume)
- After release: right-sided murmurs return to normal earlier than left-sided murmurs (Harrison's Principles of Internal Medicine, 22e, Table 246-1)
-
Equalizing ear pressure (e.g., during flight or diving)
-
Diagnosing hernias and varicoceles - radiologists perform with and without Valsalva to demonstrate small defects (Sleisenger & Fordtran's GI Disease)
-
Provocative test for presyncope / autonomic dysfunction
Natural triggers: Heavy lifting, coughing, vomiting, straining at stool, childbirth (can cause Valsalva retinopathy).
Muller's Maneuver - In Depth
Mechanism:
- Patient inspires forcefully against a closed glottis (mouth and nose closed)
- Intrathoracic pressure becomes strongly negative
- This simulates the negative airway pressure during obstructive sleep apnea
- Pharyngeal walls are sucked inward -> dynamic airway collapse becomes visible
How to perform:
- Mouth closed, nose pinched
- Patient asked to inhale forcefully
- Examiner observes pharyngeal collapse via fiberoptic nasendoscope
Clinical uses:
-
OSA (Obstructive Sleep Apnea) evaluation - primary use. Done with flexible fiberoptic endoscopy (nasopharyngoscopy) in awake patients, both sitting and supine, to identify the level and degree of pharyngeal collapse:
- Retropalatal collapse
- Retrolingual collapse
- Hypopharyngeal collapse Used preoperatively to predict success of UPPP (uvulopalatopharyngoplasty). Sher et al. found that patients with palatal collapse had 73% chance of >=50% reduction in RDI after UPPP (Cummings Otolaryngology, 6e).
-
Respiratory muscle assessment - measuring maximal inspiratory pressure (MIP/PImax) and transdiaphragmatic pressure during maximum static inspiratory effort. Note: activates intercostals, diaphragm, and sternomastoid (Fishman's Pulmonary Diseases).
-
Mueller-Hillis maneuver (obstetrics variant) - used to predict dystocia in the second stage of labor.
Limitations:
- Poor inter- and intra-rater reliability for OSA assessment
- Low correlation with intraoperative findings
- Low positive-predictive value for surgical outcomes
- Findings in awake patients differ from sleep (hence drug-induced sleep endoscopy [DISE] is gaining favor)
Key Comparison Summary
| Valsalva | Muller's | |
|---|---|---|
| Pressure direction | +ve intrathoracic | -ve intrathoracic |
| Venous return | Decreased | Increased |
| LV preload | Decreased | Increased |
| HOCM murmur | Louder (obstruction worsens) | Softer |
| MVP click/murmur | Earlier + louder | Later (more volume) |
| Main cardiac use | SVT termination; murmur differentiation | Not used for cardiac murmurs |
| Main airway use | Ear pressure equalization | OSA level-of-obstruction mapping |
| Analogy | Blowing out | Sucking in |
Pneumonic to remember the exceptions for Valsalva and heart murmurs:
"HOCM and MVP go UP with Valsalva" - everything else goes down because preload falls; but HOCM worsens with less blood (cavity collapses), and MVP's leaflets prolapse earlier with a smaller ventricle.
Sources: Harrison's Principles of Internal Medicine 22e | Roberts & Hedges' Clinical Procedures in Emergency Medicine | Cummings Otolaryngology Head & Neck Surgery | K.J. Lee's Essential Otolaryngology | Fishman's Pulmonary Diseases and Disorders | Miller's Anesthesia 10e
How do you differentiate MVP vs HOCM using auscultation maneuvers?
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - both diagrams retrieved. Here is the full answer:
Differentiating MVP vs. HOCM by Auscultation Maneuvers
The core principle is simple: both murmurs respond to the same direction of preload change, but MVP has an additional unique feature - a mid-systolic click that moves in time.
The Underlying Logic
HOCM murmur is caused by dynamic LVOT obstruction. Less blood in the LV = the walls come closer together = more obstruction = louder murmur. More blood = less obstruction = softer murmur.
MVP murmur is caused by mitral leaflet prolapse into the LA once the LV shrinks enough that the chordae go slack. Less blood in the LV = leaflets prolapse earlier in systole = click moves toward S1, murmur starts earlier and is longer. More blood = leaflets stay supported longer = click moves toward S2, murmur is shorter.
Maneuver-by-Maneuver Breakdown
| Maneuver | Effect on Preload | HOCM Murmur | MVP Click | MVP Murmur |
|---|---|---|---|---|
| Valsalva (strain) | Decreases | Louder | Moves toward S1 (earlier) | Louder + longer |
| Standing | Decreases | Louder | Moves toward S1 (earlier) | Louder + longer |
| Squatting | Increases | Softer | Moves toward S2 (later) | Softer + shorter |
| Passive leg raise | Increases | Softer | Moves toward S2 (later) | Softer + shorter |
| Handgrip (isometric) | Increases afterload | Softer | Moves toward S1 (earlier) | Louder |
(Source: Tintinalli's Emergency Medicine, Table 55-5)
The Critical Differentiator: Handgrip
This is the key bedside test to distinguish the two:
- Handgrip increases systemic vascular resistance (afterload). This increases LV volume (the LV empties less completely against greater resistance) AND increases aortic pressure.
- In HOCM: increased LV volume relieves outflow obstruction → murmur decreases
- In MVP: increased LV volume delays prolapse → click moves toward S2 and murmur shortens → but the murmur intensity is often increased due to greater MR from elevated LV-LA pressure gradient
In short: handgrip softens HOCM but tends to increase or maintain MVP murmur - this is the one maneuver where they diverge.
The Click: MVP's Unique Signature
MVP is the only murmur with a mid-systolic non-ejection click (C). This click is absent in HOCM. Tracking its movement is diagnostic:

- Standing (small LV): click moves closer to S1 - murmur longer
- Squatting (large LV): click moves closer to S2 - murmur shorter
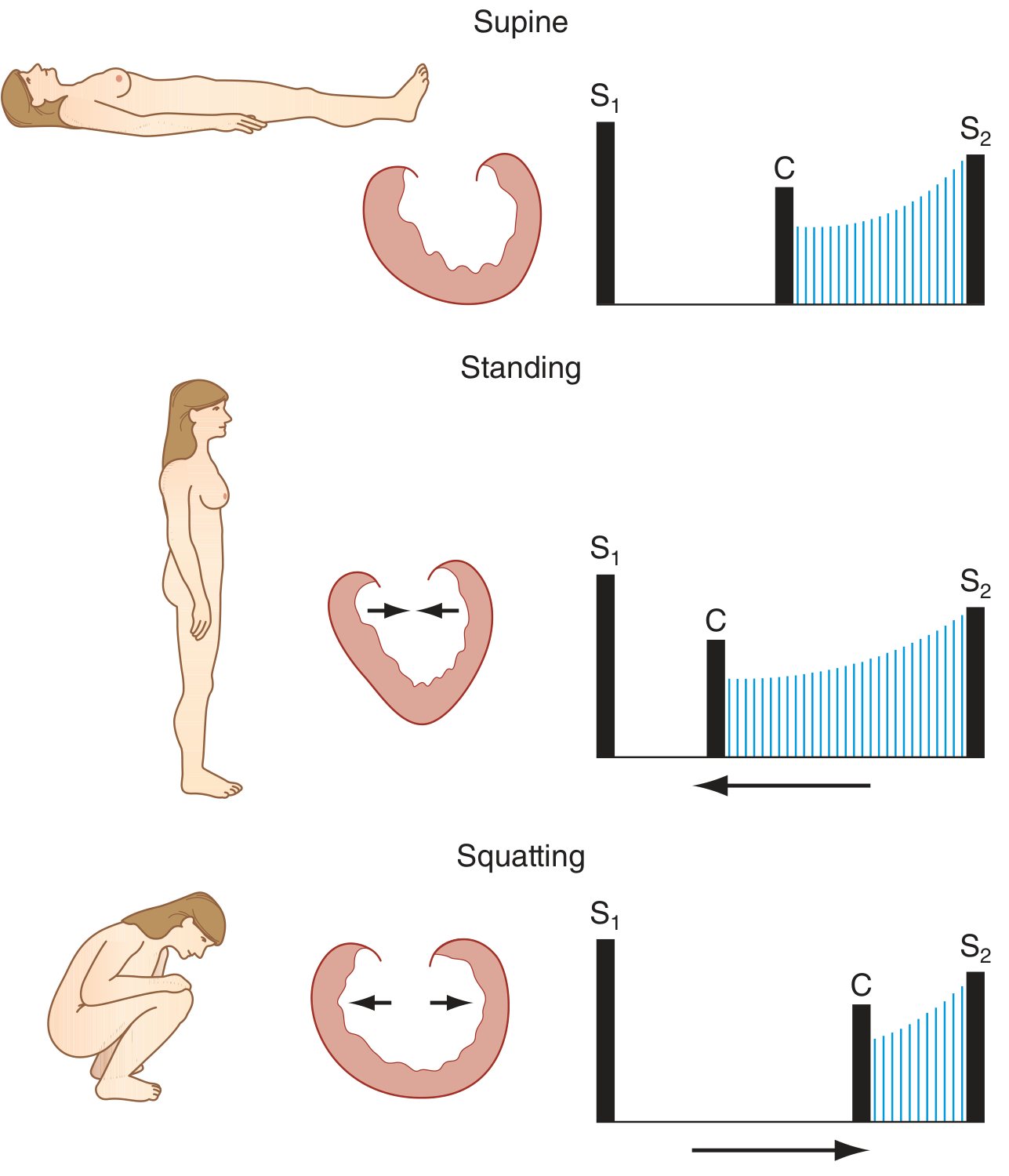
(Harrison's Principles of Internal Medicine 22e, Figure 44-3)
The systolic murmur of HOCM behaves similarly to MVP on standing/squatting - but HOCM has no click. The click is the distinguishing feature.
Other Differentiating Features (Non-Maneuver)
| Feature | HOCM | MVP |
|---|---|---|
| Mid-systolic click | Absent | Present (pathognomonic) |
| Murmur location | Lower left sternal border / apex | Apex, radiates to axilla |
| Carotid pulse | Rapid upstroke, bisferiens (bifid) | Normal |
| Apical impulse | Sustained, hyperdynamic; presystolic lift | Usually normal |
| S4 | Common (stiff, hypertrophied LV) | Absent |
| LVH on ECG | Present | Absent |
| Family history | Autosomal dominant (sarcomere gene) | Connective tissue (Marfan, etc.) |
| Demographics | Young athlete, family history of SCD | Young women, thin build |
Quick Memory Rule
"Both go UP with Valsalva and standing - but only MVP has a CLICK, and only HOCM has an S4 + LVH."Handgrip = the separator: HOCM down, MVP click goes toward S2 (shorter murmur).
Sources: Harrison's Principles of Internal Medicine 22e (Fig. 44-3, Table 246-1) | Tintinalli's Emergency Medicine (Table 55-5) | Fuster & Hurst's The Heart 15e (Fig. 2-27) | Miller's Anesthesia 10e
What ECG findings distinguish HOCM from MVP?
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
I have all the key data. Here's the full answer:
ECG Findings: HOCM vs. MVP
HOCM - ECG is Almost Always Abnormal
The resting ECG is abnormal in the vast majority of HOCM patients and is one of the most important clues to the diagnosis. Key findings:
1. Left Ventricular Hypertrophy (LVH)
The most common finding. Seen as:
- Increased QRS voltage (large R in lateral leads, deep S in V1-V3)
- Left axis deviation
- ST depression and T-wave inversion in lateral leads (the classic "strain pattern")
2. Septal Q Waves ("Pseudoinfarction Pattern")
- Deep, narrow Q waves (>0.3 mV) in anterior, lateral, or inferior leads (I, aVL, V4-V6, or II, III, aVF)
- These are caused by hypertrophied septal depolarization, not scar
- They can mimic Q waves of prior MI - but the T-wave polarity is the key differentiator:
- HOCM: T waves are upright in the same leads that have the septal Q waves (QS or QR complexes with upright T)
- Myocardial infarction: T waves are inverted in leads with Q waves
This is the classic "pseudoinfarction" pattern of HOCM.
Real HOCM ECG:
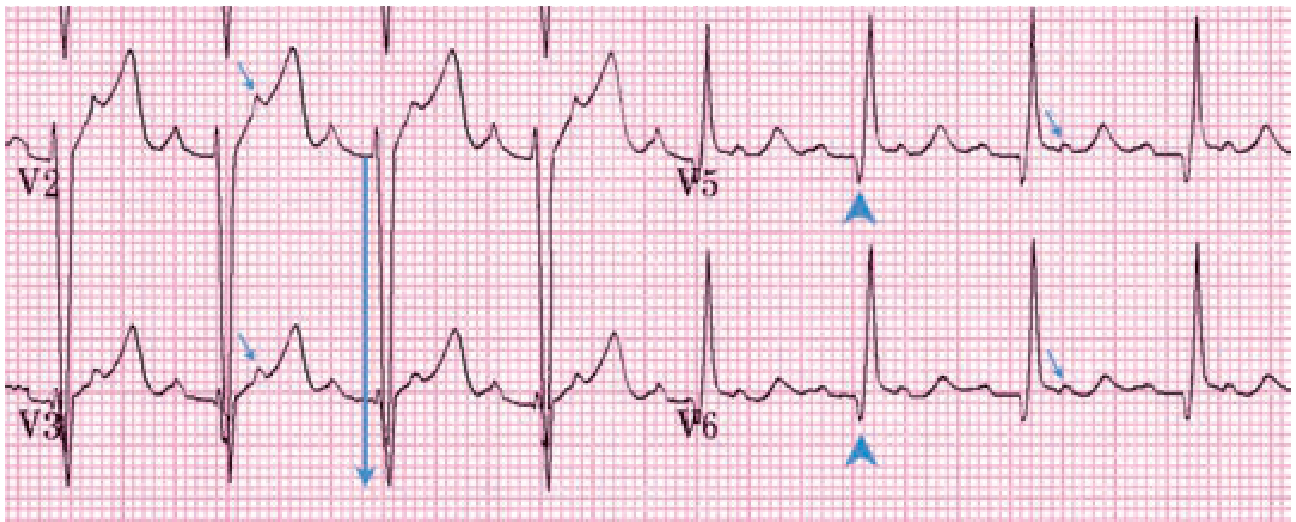
V2-V3: Deep S-wave voltage (28 mm in V3) = LVH. V5-V6: Narrow septal Q waves (arrowheads) with upright T waves - typical HOCM pseudoinfarction pattern. Small arrows show flutter P waves hiding in ST segments (this patient had atrial flutter with 2:1 block).
(Tintinalli's Emergency Medicine, Figure 55-1)
3. Left Atrial Enlargement
- Broad, notched P waves in lead II (P mitrale) or biphasic P in V1
- Reflects the stiff, non-compliant LV requiring high filling pressures
4. Arrhythmias
- Atrial fibrillation - seen in up to 20-25% of HOCM patients; can be catastrophic (loss of atrial kick dramatically worsens obstruction)
- Ventricular arrhythmias - non-sustained VT on Holter; a major risk factor for sudden cardiac death
- WPW pattern (delta waves + short PR) - seen in some HOCM patients, especially those with PRKAG2 mutations (glycogen storage type)
5. Giant Negative T Waves
- A specific variant: Apical HOCM (Yamaguchi syndrome) - predominantly affects the LV apex rather than septum
- Hallmark ECG: giant symmetric T-wave inversions in precordial leads V3-V5, often >10 mm deep
- This variant is more common in Japanese patients and is typically non-obstructive
MVP - ECG Usually Normal
The ECG in MVP is usually normal, which is a key distinguishing feature from HOCM.
"The ECG is usually normal. If suspecting mitral valve prolapse, refer the patient for outpatient echocardiography to confirm the diagnosis." (Tintinalli's Emergency Medicine)
When abnormalities are present:
1. T-Wave Inversions in Inferior Leads (II, III, aVF)
- The most characteristic MVP-associated ECG finding
- Flat or inverted T waves in inferior leads
- Can mimic inferior ischemia
- Clinically important: T-wave abnormalities in inferior leads have been associated with malignant arrhythmias in MVP patients - these patients have a higher risk of sudden death (Fuster & Hurst's The Heart, 15e)
2. Biphasic/Inverted T Waves in V5-V6
- Less common, nonspecific
- May suggest significant mitral regurgitation if present alongside LA enlargement
3. QTc Prolongation (mild)
- Can occur in some MVP patients, contributing to arrhythmia risk
4. Arrhythmias
- PVCs - frequent and complex PVCs are associated with the "malignant arrhythmic phenotype" of MVP
- Atrial fibrillation - less common than in HOCM unless significant MR has caused LA enlargement
- PSVT/SVT - due to accessory pathways more common with connective tissue predisposition
Side-by-Side ECG Summary
| Feature | HOCM | MVP |
|---|---|---|
| Overall ECG | Abnormal in majority | Usually normal |
| LVH | Present (most cases) | Absent (unless severe MR) |
| Q waves | Deep narrow septal Q waves (ant/lat/inf) | Absent |
| T-wave polarity with Q waves | Upright (pseudoinfarction clue) | N/A |
| T-wave inversions | Lateral strain pattern (I, aVL, V5-V6) | Inferior leads (II, III, aVF) |
| Giant T-wave inversions | V3-V5 (apical variant/Yamaguchi) | Absent |
| Left atrial enlargement | Common | Only with significant MR |
| Atrial fibrillation | Common (20-25%) | Less common |
| WPW pattern | Rare (PRKAG2 variant) | Not associated |
| PVCs | Present, risk marker | Present; inferior T-wave inversions + PVCs = high-risk phenotype |
The One-Line Differentiator
HOCM: LVH + narrow septal Q waves + upright T waves in those Q-wave leads = pseudoinfarction pattern. ECG almost never normal.MVP: ECG usually clean. If abnormal, look for T-wave inversions isolated to inferior leads - and take them seriously as a marker of arrhythmic risk.
Sources: Tintinalli's Emergency Medicine (Table 55-5, Figure 55-1) | Fuster & Hurst's The Heart 15e | Harrison's Principles of Internal Medicine 22e | Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.