National health mission psm
Reading File
Finding Sources
Searching the Web
National Health Mission NHM India PSM components objectives 2024
Reading File
Reading File
Reading File
Here is a comprehensive PSM (Preventive and Social Medicine) overview of the National Health Mission (NHM), drawn from Park's Textbook of PSM and official NHM sources:
National Health Mission (NHM)
Overview
The National Health Mission was approved by the Government of India in May 2013, bringing two sub-missions under one umbrella:
- NRHM - National Rural Health Mission (launched 5 April 2005)
- NUHM - National Urban Health Mission (launched 2013)
Vision: Universal access to equitable, affordable, and quality health care services that are accountable and responsive to people's needs. It also advances Sustainable Development Goal 3 - "Ensure healthy lives and promote well-being for all at all ages."
Main Programmatic Components
- Health System Strengthening (rural and urban)
- RMNCH+A - Reproductive, Maternal, Newborn, Child and Adolescent Health
- Communicable Disease Control
- Non-Communicable Disease Control
Six Financing (Flexipool) Components
- NRHM-RCH Flexipool
- NUHM Flexipool
- Flexible pool for Communicable Diseases
- Flexible pool for Non-Communicable Diseases (including Injury and Trauma)
- Infrastructure Maintenance
- Family Welfare Central Sector component
Historical Milestones (Health Programme Evolution)
| Year | Programme |
|---|---|
| 1992 | Child Survival and Safe Motherhood Programme (CSSM) |
| 1997 | RCH I |
| 2005 | RCH II |
| 2005 | National Rural Health Mission (NRHM) |
| 2013 | RMNCH+A Strategy |
| 2013 | National Health Mission (NHM) |
| 2014 | India Newborn Action Plan (INAP) |
| 2018 | Ayushman Bharat Programme |
Targets of NHM (12th Five Year Plan)
| Target | Goal |
|---|---|
| Maternal Mortality Rate (MMR) | Reduce to 1/1000 live births |
| Infant Mortality Rate (IMR) | Reduce to 25/1000 live births |
| Total Fertility Rate (TFR) | Reduce to 2.1 |
An important achievement of NHM has been a considerable reduction in out-of-pocket expenses from 72% to 60%.
National Rural Health Mission (NRHM)
Launched: 5th April 2005 | Focus: 18 special focus states
Special Focus States (18 total):
- 8 Empowered Action Group (EAG) States: Bihar, Jharkhand, Madhya Pradesh, Chhattisgarh, Uttar Pradesh, Uttarakhand, Odisha, Rajasthan
- 8 North-East States: Assam, Arunachal Pradesh, Manipur, Meghalaya, Mizoram, Nagaland, Sikkim, Tripura
- Himachal Pradesh and Jammu & Kashmir
Main Aim of NRHM
Provide accessible, affordable, accountable, effective, and reliable primary health care and bridge the gap in rural health care through creation of ASHA cadre.
Programmes Integrated under NRHM
- RCH II
- National Vector Borne Disease Control Programme (malaria, filaria, kala-azar, dengue, Japanese encephalitis)
- National Leprosy Eradication Programme (NLEP)
- Revised National TB Control Programme (RNTCP)
- National Programme for Control of Blindness
- Iodine Deficiency Disorder Control Programme
- Integrated Disease Surveillance Project (IDSP)
Plan of Action - Infrastructure Strengthening
- ASHA creation - Accredited Social Health Activist (1 per 1000 population in rural areas)
- Sub-Centres strengthened - Essential drugs (allopathic + AYUSH), untied funds of Rs. 10,000/year
- PHCs strengthened - 24-hour services in at least 50% PHCs, AYUSH practitioners, standard treatment guidelines, 2nd doctor provision
- CHCs upgraded - All CHCs (30-50 beds) as 24-hour First Referral Units (FRUs)
National Urban Health Mission (NUHM)
Coverage: All state capitals, district headquarters, and ~779 cities/towns with population ≥50,000 (Census 2011). Cities below 50,000 population are covered by NRHM.
Focus Groups
- Urban poor in listed and unlisted slums
- Vulnerable groups - homeless, rag-pickers, street children, rickshaw pullers, construction/kiln workers, sex workers, temporary migrants
- Public health - sanitation, clean drinking water, vector control
- Strengthening urban local bodies' health capacity
7 Metropolitan Cities (Special Treatment)
Mumbai, New Delhi, Chennai, Kolkata, Hyderabad, Bengaluru, Ahmedabad - managed through Municipal Corporations directly.
Urban Community Structures
- ASHA/Link Worker (LW): 1 per 1000-2500 urban poor (200-500 households)
- Mahila Arogya Samiti (MAS): Per 50-100 households; receives annual grant of Rs. 5,000
- Rogi Kalyan Samitis
Key NHM Interventions to Reduce IMR and MMR
| Intervention | Details |
|---|---|
| Janani Suraksha Yojana (JSY) | Cash incentive to BPL pregnant women for institutional delivery |
| Janani Shishu Suraksha Karyakram (JSSK) | Free delivery (including C-section), free drugs, diagnostics, blood, diet, and transport in public facilities |
| RMNCH+A Strategy | Focus on 184 high-priority districts |
| SNCUs/NBSUs | Special Newborn Care Units and Newborn Stabilization Units |
| Name-based tracking | Web-enabled tracking of pregnant women for ANC/PNC |
| Free Drugs & Free Diagnostic Service | Reduces out-of-pocket expenditure |
| Village Health and Nutrition Days | Outreach for maternal and child health services |
| Iron and Folic Acid Supplementation | For pregnant and lactating women |
| District Hospital & Knowledge Centers (DHKC) | Multi-specialty care including dialysis, cardiac, cancer, mental health, and telemedicine |
| National Iron+ Initiative | Addressing anaemia across life stages |
ASHA (Accredited Social Health Activist) - Key Figure of NRHM
- Rural: 1 ASHA per 1000 population
- Urban: 1 ASHA per 1000-2500 urban poor population
- Acts as a link between community and health system
- Promotes good health practices, RCH services, contraception, gender equality, maternal and child care
Recent Initiatives Under NHM (2024-2026)
- Ayushman Bharat - PM-JAY (health insurance component)
- National Sickle Cell Anaemia Elimination Mission
- National TB Elimination Programme (NTEP)
- PM-ABHIM (Pradhan Mantri Ayushman Bharat Health Infrastructure Mission)
- Revised Mobile Medical Units (MMU) Guidelines 2026
- Revised CEmONC Curriculum 2024
Source: Park's Textbook of Preventive and Social Medicine; NHM Official Website
National health mission. Parks reference in structerd and point wise and flow chart form
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Now I have all the data from Park's. Here is the complete, structured, point-wise answer with a text-based flowchart:
NATIONAL HEALTH MISSION (NHM)
Park's Textbook of PSM - Structured Notes
1. INTRODUCTION
- Ministry of Health & Family Welfare launched NHM by merging all health programmes under one umbrella
- Approved: May 2013
- Two Sub-Missions:
- National Rural Health Mission (NRHM)
- National Urban Health Mission (NUHM)
- Key Achievement: Reduction in out-of-pocket expenses from 72% → 60%
2. HISTORICAL MILESTONES (Parks)
1992 → Child Survival and Safe Motherhood Programme (CSSM)
↓
1997 → RCH I
↓
2005 → RCH II + NRHM (launched 5 April 2005)
↓
2013 → RMNCH+A Strategy + NHM (approved May 2013)
↓
2014 → India Newborn Action Plan (INAP)
↓
2018 → Ayushman Bharat Programme
3. NHM - OVERALL STRUCTURE (FLOWCHART)
┌─────────────────────────────┐
│ NATIONAL HEALTH MISSION │
│ (Approved May 2013) │
└─────────────┬───────────────┘
│
┌───────────────────┴────────────────┐
↓ ↓
┌───────────────────────┐ ┌─────────────────────────┐
│ NRHM │ │ NUHM │
│ National Rural │ │ National Urban │
│ Health Mission │ │ Health Mission │
│ (Launched 5 Apr 2005)│ │ (Launched 2013) │
└───────────────────────┘ └─────────────────────────┘
4. PROGRAMMATIC COMPONENTS (3 Main)
NHM COMPONENTS
│
├─── 1. Health System Strengthening (Rural + Urban)
│
├─── 2. RMNCH+A
│ (Reproductive - Maternal - Newborn - Child - Adolescent Health)
│
└─── 3. Disease Control
├── Communicable Diseases
└── Non-Communicable Diseases
5. SIX FINANCING (FLEXIPOOL) COMPONENTS
| # | Flexipool Component |
|---|---|
| i | NRHM-RCH Flexipool |
| ii | NUHM Flexipool |
| iii | Flexible pool for Communicable Diseases |
| iv | Flexible pool for NCDs (including Injury and Trauma) |
| v | Infrastructure Maintenance |
| vi | Family Welfare Central Sector component |
6. NHM TARGETS (12th Five Year Plan)
| Indicator | Target | Achievement |
|---|---|---|
| IMR | Reduce to 25/1000 live births | Reduced (33 in 2019) |
| MMR | Reduce to 1/1000 live births | Reduced (103/100,000) |
| TFR | Reduce to 2.1 | ~2.0 achieved |
| Sex Ratio at Birth | 950/1000 | Improving |
7. NATIONAL RURAL HEALTH MISSION (NRHM) - DETAILED
A. Basic Facts
- Launched: 5th April 2005 (for 7 years; extended to 2017)
- Operational: Whole country with special focus on 18 states
B. 18 Special Focus States
18 Special Focus States
│
├── 8 EAG (Empowered Action Group) States
│ Bihar, Jharkhand, MP, Chhattisgarh,
│ UP, Uttarakhand, Odisha, Rajasthan
│
├── 8 North-East States
│ Assam, Arunachal Pradesh, Manipur, Meghalaya,
│ Mizoram, Nagaland, Sikkim, Tripura
│
└── 2 Others: Himachal Pradesh + Jammu & Kashmir
C. Main Aim (5 A's - Park's)
Provide Accessible, Affordable, Accountable, Effective and Reliable primary health care
D. Programmes Integrated under NRHM
- RCH II
- National Vector Borne Disease Control Programme (malaria, filaria, kala-azar, dengue, Japanese encephalitis)
- National Leprosy Eradication Programme (NLEP)
- Revised National TB Control Programme (RNTCP)
- National Programme for Control of Blindness
- Iodine Deficiency Disorder Control Programme
- Integrated Disease Surveillance Project (IDSP)
E. Synergic Approach (Park's)
- AYUSH integrated into mainstream healthcare
- Health related to determinants: nutrition, sanitation, hygiene, safe drinking water
8. NRHM INFRASTRUCTURE (Pyramid - Park's Fig. 11)
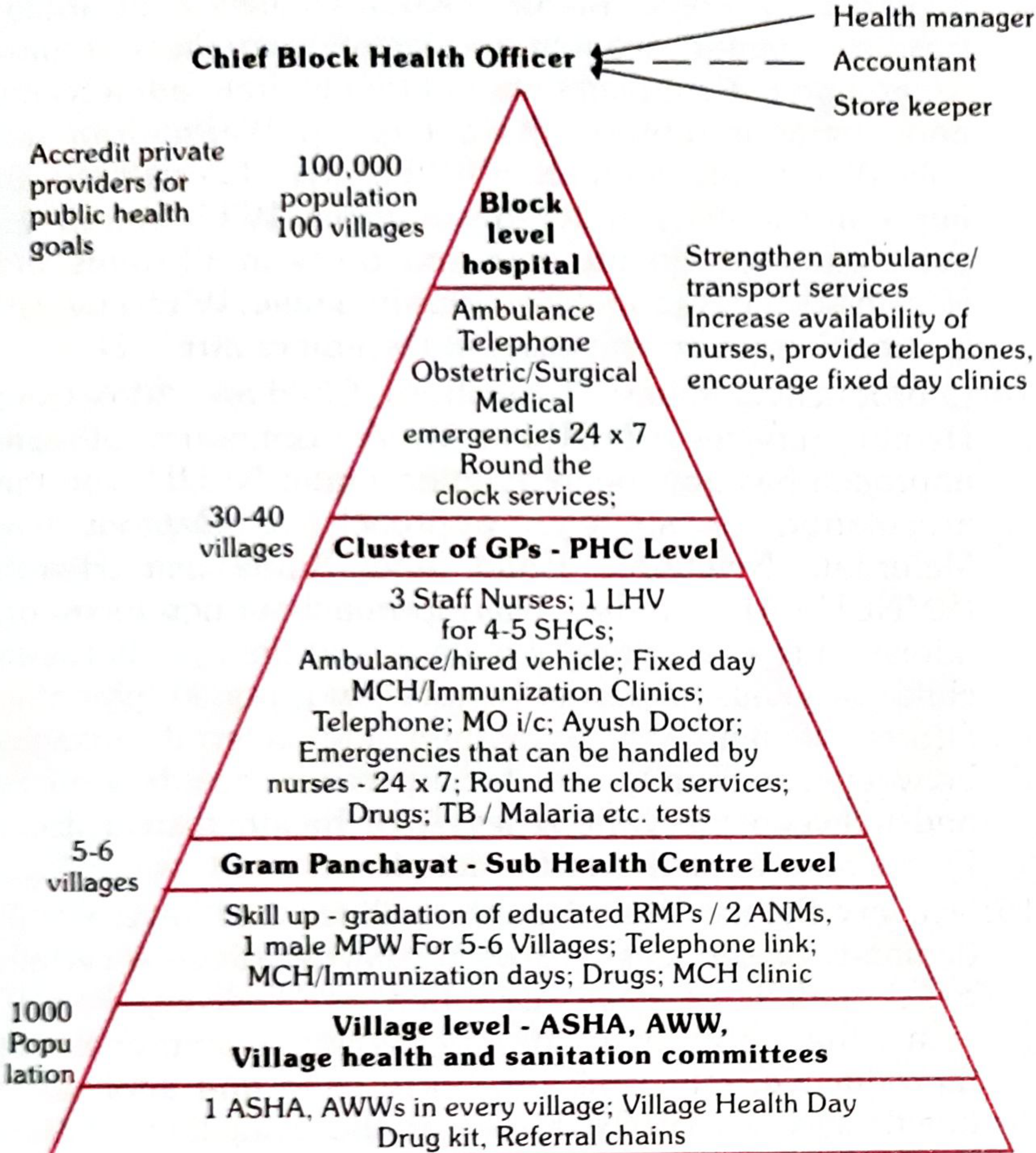
LEVEL POPULATION FACILITY KEY PERSONNEL/SERVICES
─────────────────────────────────────────────────────────────────────────────
Block Level 1,00,000 Block Level Chief Block Health Officer
100 villages Hospital (CHC) + Health Manager + Accountant
(24×7 FRU) Ambulance, OBS/Surgical/Medical
Emergencies Round the Clock
PHC Level 30-40 Cluster of GPs - 3 Staff Nurses, 1 LHV,
villages PHC MO-i/c, AYUSH Doctor,
24×7 Emergency care,
MCH/Immunization Clinics
Sub-Centre Level 5-6 Gram Panchayat - 2 ANMs + 1 Male MPW,
villages Sub Health Centre MCH/Immunization Days,
Drugs, MCH Clinic
Village Level 1,000 Village ASHA + AWW + VHSNC
population (ASHA, AWW, Drug Kit, Referral Chain,
VHSNC) Village Health Day
─────────────────────────────────────────────────────────────────────────────
- District = Core unit of planning, budgeting, and implementation
- All vertical programmes merged into District Health Mission (district level) and State Health Mission (state level)
- Mobile Medical Unit at district level for outreach
9. PLAN OF ACTION - INFRASTRUCTURE STRENGTHENING (Park's)
1. ASHA Creation
↓
2. Sub-Centre Strengthening
- Essential drugs (Allopathic + AYUSH)
- Untied funds: Rs. 10,000/year (18 states)
- Additional ANMs / MPW
↓
3. PHC Strengthening
- 24-hr service in ≥50% PHCs
- AYUSH practitioner included
- Standard Treatment Guidelines
- 2nd doctor (1M + 1F)
↓
4. CHC Strengthening (First Referral Care)
- All CHCs (30-50 beds) as 24-hr FRUs
- Anaesthetist posting
- Indian Public Health Standards (IPHS)
- Rogi Kalyan Samiti (RKS)
- Standards of services and costs
10. MAJOR INITIATIVES UNDER NRHM
A. ASHA (Accredited Social Health Activist)
- Selection: Woman (married/widow/divorced), age 25-45 years, education ≥ Class 8
- Norm: 1 ASHA per 1000 population (relaxed to 1 per habitation in tribal/hilly/desert areas)
- Acts as link between community and health system
B. Rogi Kalyan Samiti (RKS) - Patient Welfare Committee
- Registered society; members act as trustees
- Manages hospital affairs, patient welfare
- Receives untied funds
- 32,005 RKS set up in DH, SDH, CHC, PHC (as of March 2015)
C. Untied Grants to Sub-Centres
- Sub-centres equipped with BP instruments, Hb testing kits
- Untied funds for local health needs
D. Village Health & Sanitation Committee → renamed VHSNC (Village Health, Sanitation & Nutrition Committee)
E. Indian Public Health Standards (IPHS)
- Norms for infrastructure, staff, equipment, management at all levels
F. National Ambulance Services
- Dial 108 - Emergency Response (critical care, trauma, accidents)
- Dial 102 - Basic patient transport (focus: pregnant women and children; JSSK entitlements)
- Dial 104 - Mobile health services
- 8680 (Dial-108) + 8718 (Dial-102) + 603 (Dial-104) vehicles operational
G. Web-enabled Mother and Child Tracking System (MCTS)
- Name-based tracking of every pregnant woman and child up to 3 years
- Tracks: ANC, institutional delivery, PNC, immunization
- Linked with AADHAR for subsidy tracking
H. Public-Private Partnership (PPP)
- 75% health services provided by private sector; PPP ensures RCH services reach community
11. NEW INITIATIVES UNDER NRHM (from 2011 onwards)
| # | Initiative | Key Detail |
|---|---|---|
| 1 | Home Delivery of Contraceptives | By ASHA (condoms, OCP, ECP) |
| 2 | DLHS-4 | District Level Household Survey in 26 states/UTs |
| 3 | Menstrual Hygiene Scheme | 152 districts, 1.5 crore adolescent girls, 20 states |
| 4 | Differential Financial Approach | Funds based on case load and services |
| 5 | ASHA in Home Based Newborn Care | ASHA visits newborns at home |
| 6 | VHSNC | Village Health, Sanitation and Nutrition Committee |
| 7 | AYUSH Mainstreaming | AYUSH hospitals/dispensaries under NRHM |
| 8 | RBSK | Rashtriya Bal Swasthya Karyakram - launched Feb 2013 - 4Ds screening |
| 9 | RKSK | Rashtriya Kishor Swasthya Karyakram - launched Jan 2014 - adolescent health |
| 10 | MCH Wings | 100/50/30-bed MCH Wings; >32,000 additional beds in 550 facilities |
| 11 | Free Drugs & Free Diagnostic Service | Reduce out-of-pocket expenditure |
| 12 | National Iron+ Initiative (2013) | IFA for children, adolescents, women; WIFS for 10-19 yrs; 32 states/UTs |
| 13 | RMNCH+A | Continuum of care; 184 high-priority districts |
| 14 | Delivery Points (DPs) | ~25,000 facilities identified for focused RMNCH+A support |
| 15 | UHC | NHM = primary vehicle for Universal Health Coverage |
| 16 | Kilkari | IVR-based audio messages on pregnancy/child health to mobile phones |
12. KEY SCHEMES UNDER NHM (Flowchart)
NHM KEY SCHEMES
│
├── JSY (Janani Suraksha Yojana)
│ └─ Cash incentive for institutional delivery (BPL women)
│
├── JSSK (Janani Shishu Suraksha Karyakram)
│ └─ FREE: Delivery + C-section + Drugs + Diagnostics
│ + Blood + Diet + Transport (home → facility → home)
│ + Same for sick infants
│
├── ASHA Home Delivery of Contraceptives
│
├── RBSK (4 Ds: Defects, Diseases, Deficiencies, Developmental delays)
│
├── RKSK (Adolescent health)
│
├── National Iron+ Initiative (WIFS)
│
├── MCTS (Mother & Child Tracking System)
│
├── Dial 108 / 102 / 104 (Ambulance Services)
│
└── Kilkari (IVR mobile health messages)
13. NATIONAL URBAN HEALTH MISSION (NUHM)
Coverage
- All state capitals + district HQs + ~779 cities/towns with population ≥ 50,000 (Census 2011)
- Cities < 50,000 covered under NRHM
Focus Groups
- Urban poor in listed and unlisted slums
- Vulnerable groups - homeless, rag-pickers, street children, rickshaw pullers, construction/kiln workers, sex workers, temporary migrants
- Sanitation, clean water, vector control
- Urban Local Bodies capacity building
7 Metro Cities (Special Treatment via Municipal Corporations)
Mumbai | New Delhi | Chennai | Kolkata | Hyderabad | Bengaluru | Ahmedabad
Community Structures under NUHM
NUHM Community Structures
│
├── ASHA / Link Worker (LW)
│ └─ 1 per 1,000-2,500 urban poor (200-500 households)
│
├── Mahila Arogya Samiti (MAS)
│ └─ 1 per 50-100 households
│ Annual grant: Rs. 5,000/-
│ (States can route ASHA incentives to MAS)
│
└── Rogi Kalyan Samiti
Service Delivery under NUHM
- Urban PHCs + Urban CHCs → Universal services
- Outreach → Targeted to slum dwellers/vulnerable groups
- Female Health Workers (FHWs/ANMs) - placed at Urban PHCs with 3-6 months induction training
14. NHM GOVERNANCE STRUCTURE
National Level
Ministry of Health & Family Welfare
Mission Steering Group
↓
State Level
State Health Mission
State Health Society
↓
District Level (Core Unit)
District Health Mission
District Health Society
(All vertical programmes merged here)
↓
Block Level
Block Health Unit / CHC
↓
Village Level
ASHA + AWW + VHSNC
QUICK MEMORY AIDS
| Mnemonic | Meaning |
|---|---|
| 5 A's of NRHM | Accessible, Affordable, Accountable, Effective, Reliable |
| RMNCH+A | Reproductive, Maternal, Newborn, Child, Adolescent Health |
| 4 Ds (RBSK) | Defects at birth, Diseases, Deficiencies, Developmental delays |
| ASHA | Woman, 25-45 yrs, Class 8 educated, 1/1000 population |
| 108/102/104 | Emergency/Maternal transport/Mobile health services |
| 18 special focus states | 8 EAG + 8 NE + HP + J&K |
Source: Park's Textbook of Preventive and Social Medicine, Chapter 10 (Health Care of the Community)
This is a shared conversation. Sign in to Orris to start your own chat.