Multiple inflammed lymph nodes after pharyngitis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive overview of multiple inflamed lymph nodes following pharyngitis, synthesized from emergency medicine, internal medicine, and infectious disease textbooks.
Multiple Inflamed Lymph Nodes After Pharyngitis (Cervical Lymphadenitis)
Anatomy of Drainage
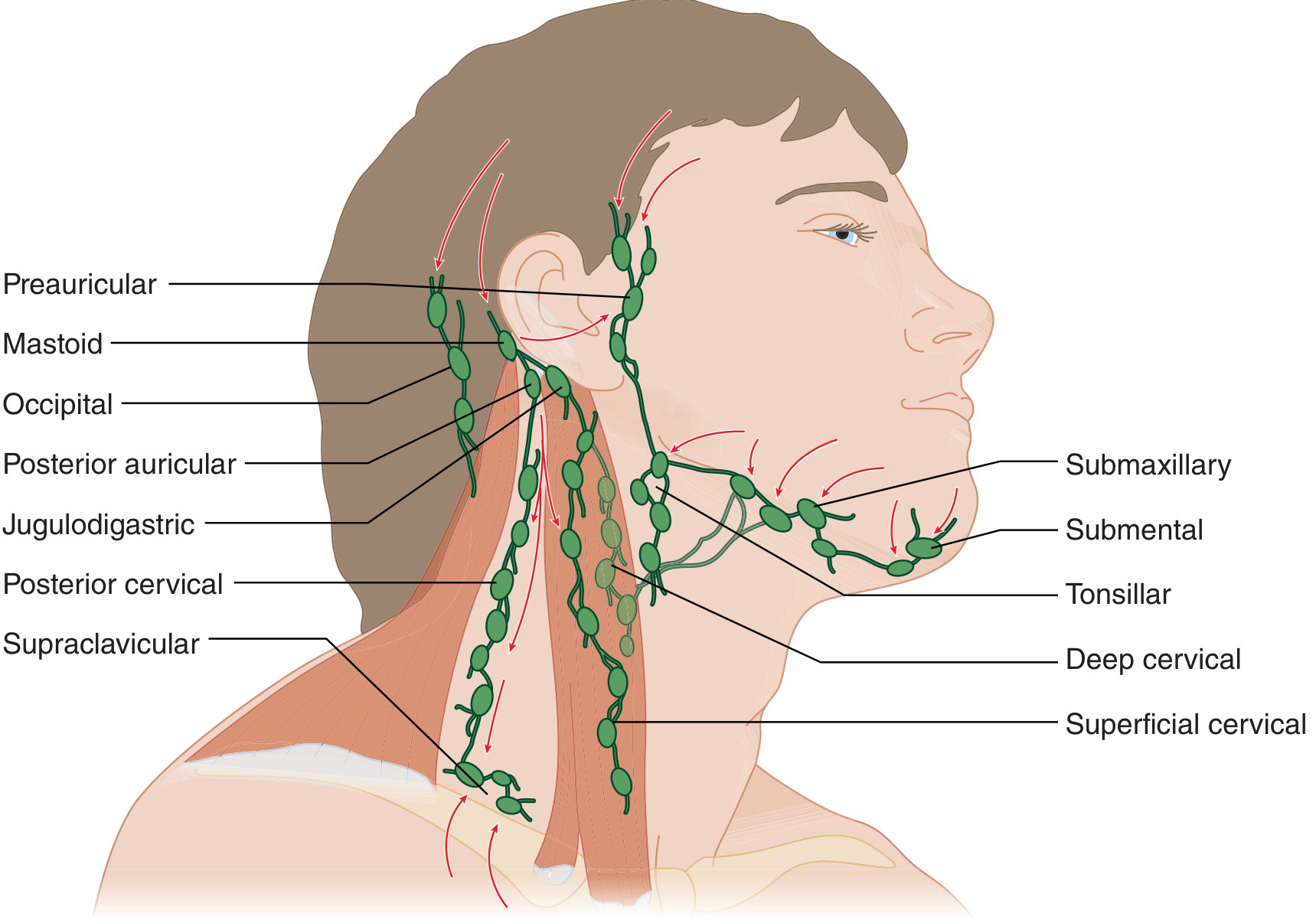
The pharynx drains primarily to the tonsillar, jugulodigastric, deep cervical, and posterior cervical nodes. Bilateral involvement after pharyngitis is expected because lymphatic drainage from the pharynx is bilateral. — Tintinalli's Emergency Medicine, p. 826
Acute Bilateral Lymphadenopathy — Most Common Scenario
Bilateral inflamed nodes after pharyngitis are most often due to viral infection and are self-limited.
| Cause | Key Features |
|---|---|
| Infectious mononucleosis (EBV) | Exudative pharyngitis + significant bilateral lymphadenopathy + splenomegaly; lymphadenopathy in 95% of cases, pharyngitis in 82% |
| Group A Streptococcus | Bacterial pharyngitis with tender anterior cervical nodes; may have exudate, palatal petechiae, scarlatiniform rash |
| Rhinovirus / adenovirus / parainfluenza | Mild viral URI; bilateral, self-limited |
| Herpes simplex (gingivostomatitis) | Oral lesions + bilateral nodes |
| Coxsackievirus (herpangina) | Oral vesicles + bilateral nodes |
| Measles | Koplik spots, conjunctivitis, descending rash |
| Rubella | Forchheimer spots, rash, polyarthritis |
| Primary HIV | Pharyngitis + mucosal erosions + diffuse lymphadenopathy |
| Mumps | Bilateral jaw swelling (parotid), may mimic cervical lymphadenopathy; associated orchitis |
— Tintinalli's Emergency Medicine, p. 826
Infectious Mononucleosis — The Classic Presentation
EBV (Epstein-Barr virus) is the most important cause to identify when bilateral lymphadenopathy follows pharyngitis.
- Incubation: 4–6 weeks
- Prodrome: Fatigue, malaise, myalgia for 1–2 weeks
- Triad: Fever + exudative pharyngitis/tonsillitis + lymphadenopathy
- Lymphadenopathy: Posterior cervical nodes most affected, but may be generalized; nodes are tender, symmetric, non-fixed
- Splenomegaly develops in the 2nd–3rd week (51% of patients)
- Lab: Leukocytosis (10,000–20,000/μL), >10% atypical lymphocytes, elevated LFTs (>90%)
- Diagnosis: Heterophile antibodies (Monospot) or EBV-specific IgM
- Treatment: Symptomatic; avoid amoxicillin/ampicillin (causes maculopapular rash)
- Avoid contact sports due to splenic rupture risk
— Harrison's Principles of Internal Medicine 22E, pp. 1143–1145
Acute Unilateral Lymphadenitis
If only one side is inflamed and the node shows classic signs (erythema, warmth, tenderness ± fluctuance), think bacterial lymphadenitis:
- Organisms: S. aureus (most common) and Group A Streptococcus
- GAS often originates from the pharynx; S. aureus from skin breaks
- Size-based management:
- < 1 cm: no treatment needed
- 1–3 cm: antibiotics (10–14 days)
-
3 cm: raises malignancy concern; if acute/inflammatory, antibiotics + close observation
- Antibiotics: First-generation cephalosporins or amoxicillin-clavulanate; clindamycin if local MRSA prevalence is high
- Reassess at 48 hours: If no improvement, broaden coverage (add MRSA coverage)
- Fluctuance → suggests abscess; often responds to antibiotics alone; needle aspiration or I&D if not resolving after 2 weeks
— Tintinalli's Emergency Medicine, pp. 826–827
When Lymphadenopathy Becomes Subacute/Chronic
Nodes persisting >6 weeks without resolution require workup for:
| Category | Causes |
|---|---|
| Mycobacterial | TB (scrofula) — painless, firm, may form cold abscess with violaceous skin; nontuberculous mycobacteria |
| Bartonella (Cat-scratch disease) | Kitten scratch/bite → regional node swelling 1–3 weeks later; usually self-limited; azithromycin may hasten resolution |
| Neoplastic | Lymphoma, metastatic carcinoma |
| Other infections | Toxoplasmosis, fungal, sarcoidosis |
TB lymphadenitis (scrofula) is the most common form of extrapulmonary TB — tender/firm node in anterior or posterior cervical chain or supraclavicular fossa; diagnose by FNA. — ROSEN's Emergency Medicine, p. 3263
Red Flags Requiring Urgent Workup
- Node > 3 cm, hard, non-tender, or fixed
- Supraclavicular location (high malignancy risk)
- Associated weight loss, night sweats, fever (B symptoms → lymphoma)
- Torticollis or trismus → deep space neck infection (retropharyngeal/parapharyngeal abscess)
- No improvement after 2–4 weeks of antibiotics
- Generalized lymphadenopathy in an immunocompromised patient
Summary Approach
- Bilateral + pharyngitis → most likely viral; test for EBV (Monospot), strep (rapid antigen/throat culture)
- Unilateral + inflammatory signs → bacterial lymphadenitis; start antibiotics targeting GAS/S. aureus
- Persistent >6 weeks → refer to otolaryngology; consider FNA, TB testing, CBC with differential, LDH
- Systemic symptoms or supraclavicular nodes → urgent hematology/oncology referral
This is a shared conversation. Sign in to Orris to start your own chat.