Computer navigation in Orthopedics with all the literature available and advances till date from the beginning gather me all information
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Searching Images
computer navigation orthopedic surgery total knee arthroplasty robotic system
Reading File
Loading Image
Now I have comprehensive material from multiple authoritative textbooks. Let me compile the complete, well-structured answer.
Computer Navigation in Orthopaedics — A Comprehensive Review
1. Historical Background
The concept of computer-assisted orthopaedic surgery (CAOS) emerged from broader developments in minimally invasive and robot-assisted surgery. The first computer-assisted robot in orthopaedics was designed specifically to drill femoral shaft bone for accurate, wobble-free placement of hip prostheses. While the concept was theoretically sound, this early robot proved no better than a skilled orthopaedic surgeon and operated considerably more slowly — a pattern that would recur with early generations of the technology. Despite initial setbacks, incremental advances in imaging, computing power, and sensor technology progressively transformed navigation from a research curiosity into a clinical tool.
— Schwartz's Principles of Surgery, 11th Ed.
2. Definition and Core Concept
Computer-navigated joint arthroplasty uses intraoperative feedback to guide the surgeon with real-time information regarding:
- Component position
- Planned bone cuts
- Limb alignment
The goal is more accurate and consistent placement of arthroplasty components than what is achievable by conventional mechanical instrumentation alone.
— Schwartz's Principles of Surgery, 11th Ed.
3. Classification of Navigation Systems
Navigation systems in orthopaedics can be broadly categorized:
| System Type | Description |
|---|---|
| Image-based (CT-based) | Preoperative CT used to create 3D digital anatomical model; registration links the virtual model to the actual patient intraoperatively |
| Imageless | Anatomical landmark registration performed intraoperatively without preoperative imaging; reduces radiation and cost |
| Fluoroscopy-based | Intraoperative fluoroscopic images used for reference and registration |
| Robotic-assisted (semi-active) | Robot constrains the cutting instrument within preset bone resection boundaries; surgeon guides the tool |
| Autonomous robotic | Robot performs bone cuts independently based on preoperative plan (less common) |
4. How Computer Navigation Works — Technical Workflow
Step 1 — Preoperative Planning
In CT-based systems, high-resolution volumetric CT scans of the operative joint are obtained preoperatively. The imaging data are imported into navigation software (e.g., Stryker OrthoMap Express, MAKO Stryker) to generate a 3D digital model of anatomical landmarks.
Step 2 — Intraoperative Registration
Optical tracking arrays (passive reflective spheres) or active infrared-emitting diodes are rigidly fixed to the bone via Schanz pins or tracker brackets. A camera system tracks the position of these arrays in real-time 3D space. The software registers the virtual model to the actual patient by identifying matching anatomical landmarks.
Step 3 — Real-Time Feedback
As the surgeon operates, the navigation system continuously updates the screen with the position, orientation, and alignment of instruments and bone cuts relative to the planned resection. In semiactive robotic systems, the robot automatically stops the saw when bone resection exceeds predetermined parameters — preventing inadvertent over-resection.
Step 4 — Intraoperative Adjustment
Navigation allows dynamic adjustment of component sizing, depth, and alignment before bone cuts are made — a critical advantage over conventional mechanical jigs.
— Miller's Anesthesia, 10th Ed.
5. Computer Navigation in Total Knee Arthroplasty (TKA)
TKA is the most extensively studied application of computer navigation in orthopaedics.
What Navigation Achieves in TKA
- More accurate restoration of the mechanical axis of the lower limb
- Improved implant balance (mediolateral and flexion-extension gap balancing)
- Reduced number of alignment outliers (components placed outside the accepted 3° variance)
- Intraoperative kinematics assessment with trial components
Robotic-Assisted Knee Surgery (RAKS)
RAKS provides:
- Predetermined parameters set in preoperative planning
- The semiactive robotic arm stops cutting when resection exceeds planned boundaries
- CT-based 3D image guides intraoperative adjustments using systems such as Stryker MAKO (Rio platform)
Clinical evidence: Multiple studies confirm RAKS restores the mechanical axis more accurately and improves implant balance and positioning compared to conventional TKA. However, like all robotic/computer-navigated procedures, it increases operative time (partly a learning curve effect) and cost. There is insufficient data to confirm improved long-term outcomes over conventional TKA.
— Miller's Anesthesia, 10th Ed.; Schwartz's Principles of Surgery, 11th Ed.
6. Computer Navigation in Total Hip Arthroplasty (THA)
MAKO Robotic-Assisted Hip Surgery (RAHS)
- Preoperative planning uses CT-based 3D digital imaging of the hip
- Optimizes acetabular cup implantation — position, angle, and depth
- Semi-active robotic arm controls the depth and size of acetabular reaming, preventing over-penetration
- Theoretically prevents malposition — the leading cause of dislocation, impingement, and early revision
Clinical Evidence
Evidence on RAHS vs. conventional THA has produced mixed short-term and long-term outcomes for functional status and disability. The primary rationale remains accurate positioning to prevent malfunction and reduce revision rates. Blood loss may be similar to or greater than conventional THA (especially in females). Extended operative time is expected during the learning curve.
— Miller's Anesthesia, 10th Ed.
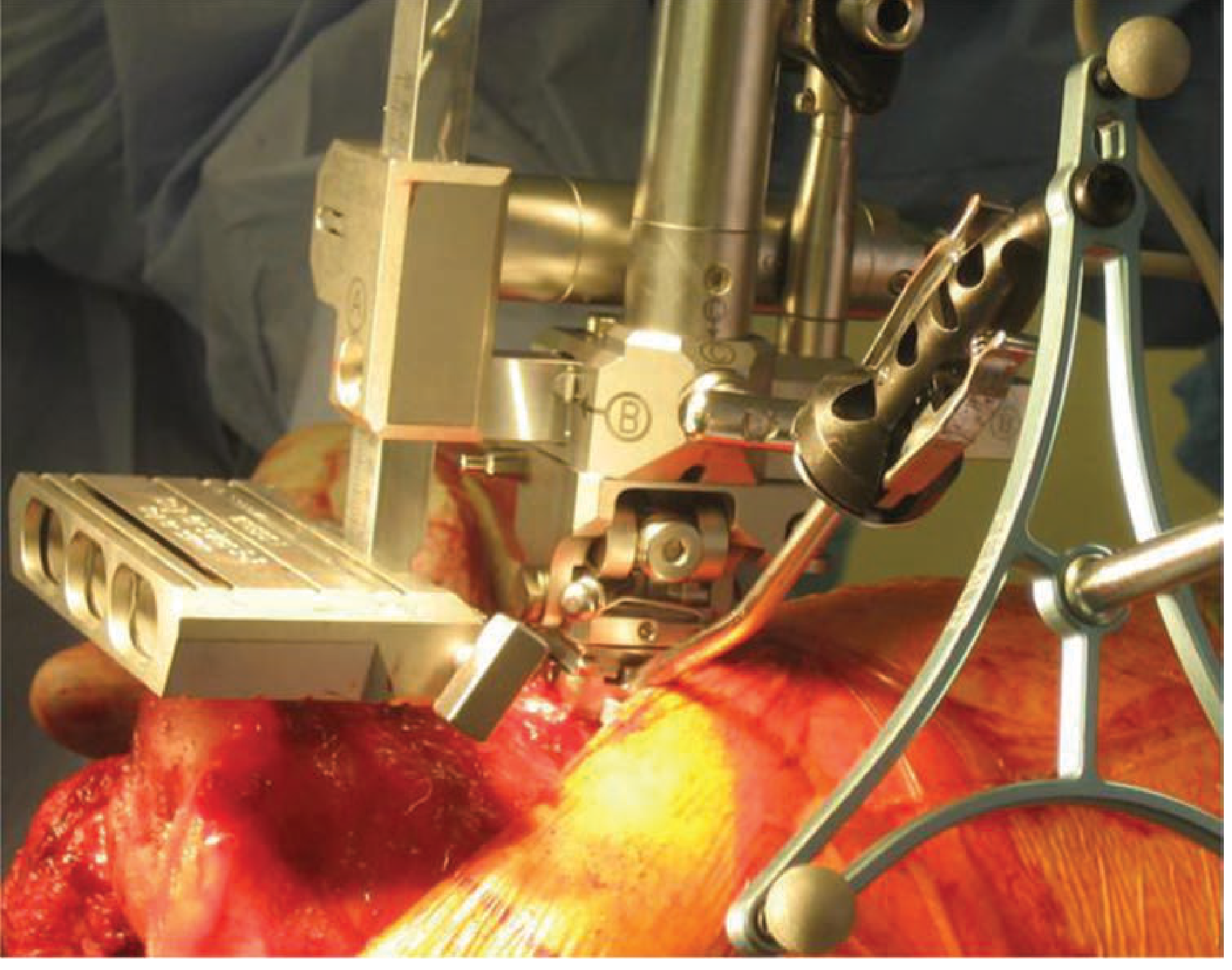
7. Key Clinical Images
Computer-assisted robotic targeting arm for total knee replacement:
Stryker MAKO Robotic System — Knee and Hip:
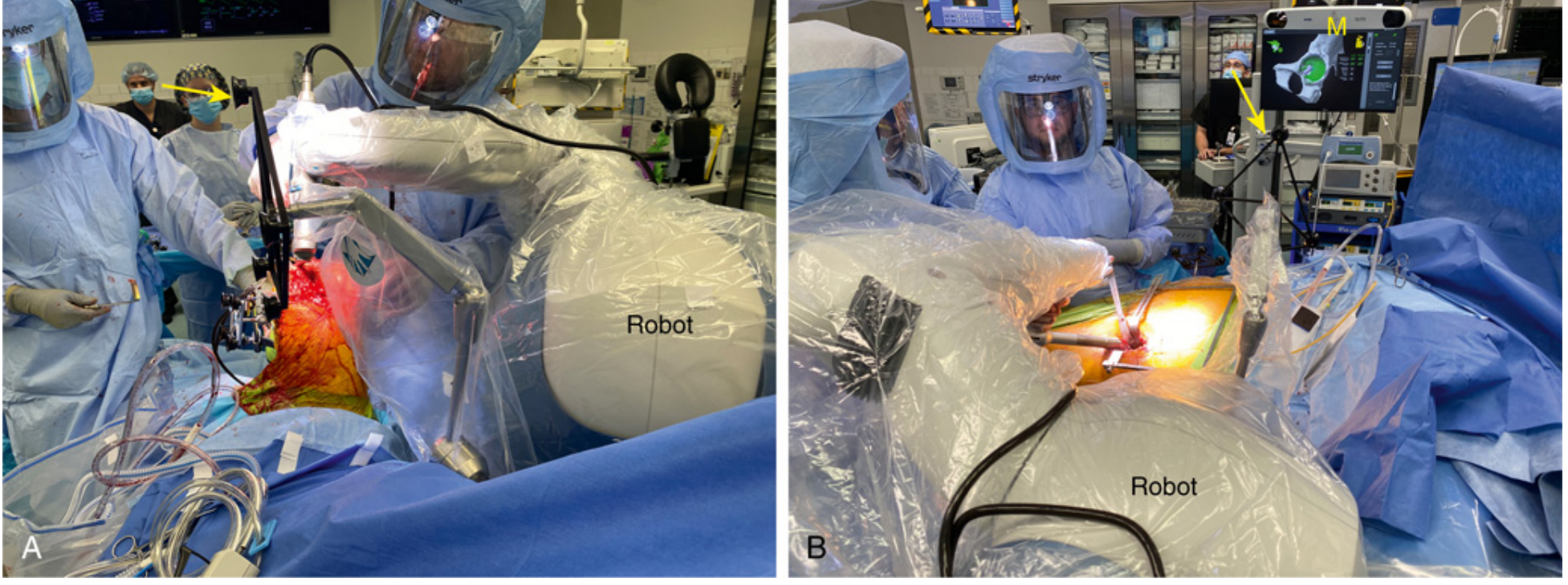
(A) MAKO robotic-assisted TKA — the robotic arm approaches from the contralateral side. The yellow arrow indicates the navigation system displaying real-time alignment.
(B) MAKO robotic-assisted THA — the monitor (M, yellow arrow) shows the 3D acetabular interface for cup positioning.
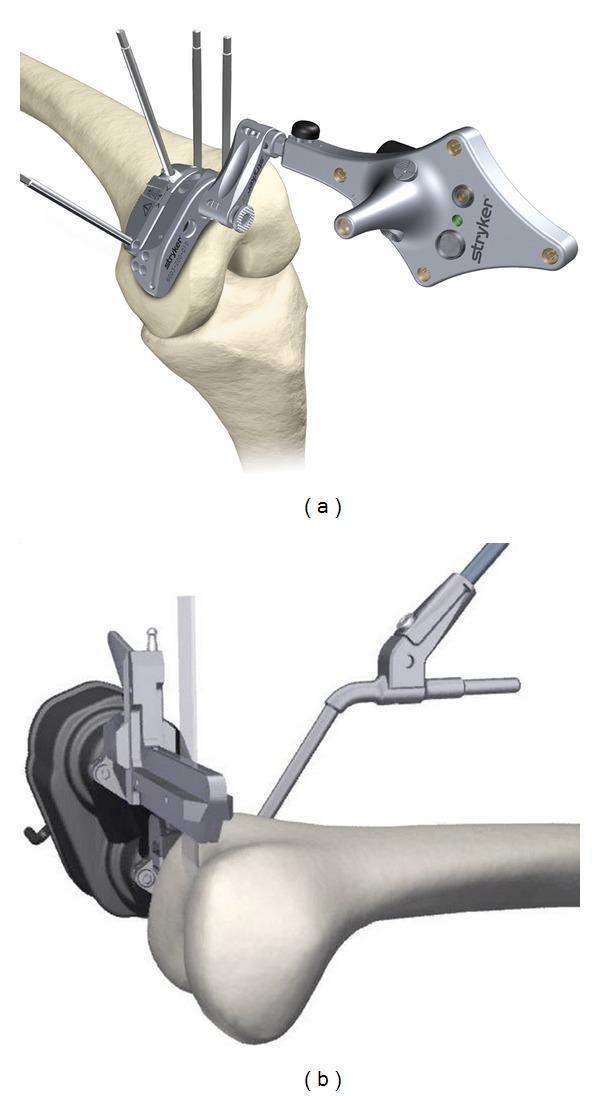
CAN vs. RAN system comparison for distal femoral osteotomy:
8. Advantages of Computer Navigation
| Advantage | Detail |
|---|---|
| Alignment accuracy | Minimizes outliers in coronal, sagittal, and rotational component placement |
| Real-time feedback | Surgeon can assess alignment and soft tissue balance before final bone cuts |
| Reduced outliers | Fewer cases with >3° deviation from ideal mechanical alignment |
| Intraoperative adjustability | Component size and position can be modified in virtual space before any irreversible step |
| Traceable data | Navigation creates a permanent digital record of intraoperative measurements |
| Reduced reliance on fluoroscopy | Imageless and CT-based systems reduce intraoperative radiation exposure |
9. Disadvantages and Limitations
| Disadvantage | Detail |
|---|---|
| Increased cost | Navigation hardware, software, and maintenance add significant capital and per-case cost |
| Prolonged operative time | Registration, array placement, and intraoperative checks extend surgery |
| Pin site complications | Schanz pins and tracking array fixation screws carry risk of pin site fracture and infection |
| Learning curve | Surgeons require dedicated training; early cases take substantially longer |
| Unproven long-term benefit | No survival or functional benefit from computer navigation has been definitively demonstrated in long-term RCTs |
| Technical failures | Registration errors, tracker movement, and software issues can mislead the surgeon |
"Computer navigation in total joint arthroplasty has been shown to minimize outliers in alignment, but there has been no proven benefit in survival or function secondary to computer-navigated or robotic-assisted joint replacement." — Schwartz's Principles of Surgery, 11th Ed., p. 1937
10. Application in Fracture Surgery
Computer navigation has been applied in periprosthetic fracture fixation, particularly for percutaneous screw fixation of periprosthetic acetabular fractures. Navigation allows accurate screw trajectory planning without excessive soft tissue dissection.
A systematic review documented periprosthetic fractures through tracking pin sites following computer-navigated and robotic TKA and unicompartmental knee arthroplasty (UKA) — a recognized but uncommon complication that must be considered in postoperative assessment.
— Rockwood and Green's Fractures in Adults, 10th Ed.
11. Specific Navigation Systems and Platforms
| Platform | Manufacturer | Primary Use |
|---|---|---|
| MAKO (Rio/TKA/THA) | Stryker | TKA, THA, UKA — CT-based, semiactive haptic robotic arm |
| OrthoMap Express Knee | Stryker | Imageless CAN for TKA |
| Praxim RAN | Praxim/Brainlab | Femoral and tibial cuts — robotic automated cutting guide |
| Zimmer Biomet ROSA | Zimmer Biomet | TKA (PERSONA system), neurosurgery (ROSA Brain) |
| ROPA TKA | — | CT-based navigation with resection surface overlay and gap balancing interface |
| Navio (Smith+Nephew) | Smith+Nephew | Imageless handheld robotic for UKA and TKA |
12. Navigation in Other Orthopaedic Applications
Beyond arthroplasty, computer navigation has been investigated or applied in:
- Unicompartmental Knee Arthroplasty (UKA): Accurate component positioning in single-compartment disease
- Osteotomies: High tibial osteotomy (HTO) with navigation-guided correction of mechanical axis
- Pedicle screw placement in spine surgery: Navigation significantly improves screw accuracy and reduces neurovascular injury
- Shoulder arthroplasty: Navigation for glenoid component positioning to minimize malpositioning and notching
- Trauma: Percutaneous screw fixation (e.g., sacroiliac, acetabular, long bone)
- Foot and ankle surgery: Early-stage evidence only; insufficient data to recommend routinely
"Robotic technology has been applied in orthopedic trauma, shoulder surgeries, and foot and ankle surgery, with insufficient or conflicting evidence to recommend for or against using robots for the abovementioned surgeries." — Miller's Anesthesia, 10th Ed.
13. Anesthetic Considerations for Navigation-Assisted Orthopaedic Surgery
Anaesthetic management for robotic and computer-navigated TKA/THA is essentially the same as for conventional arthroplasty, with important modifications:
- Multimodal analgesia is the standard approach — periarticular infiltration (ropivacaine 0.2% + morphine + ketorolac + epinephrine) at posterior capsule, medial/lateral capsular flaps, subcutaneous tissue, pin sites, and drain sites
- Regional anaesthesia: Adductor canal block for TKA (preferred over femoral nerve block to preserve quadriceps strength)
- Patient positioning: The arm on the contralateral side to the robotic approach is flexed and rotated over the thorax to create space for the robotic arm
- Extended operative time must be factored into fluid management, tourniquet time, and DVT prophylaxis planning
- Blood loss may be similar or greater than conventional THA with robotic systems
— Miller's Anesthesia, 10th Ed.
14. Current Status and Future Directions
Where Navigation Stands Today
- Navigation reliably and reproducibly reduces alignment outliers in TKA — the strongest and most consistent finding across the literature
- No randomized controlled trial has yet demonstrated a definitive benefit in implant survival or patient-reported outcomes over optimally performed conventional arthroplasty
- Adoption continues to grow driven by precision surgery principles, surgeon preference, and commercial promotion
Advances and Emerging Technologies
- Augmented reality (AR) navigation: Overlaying digital anatomical information onto the surgeon's real-time field of view via headsets
- Patient-specific instrumentation (PSI): Preoperatively manufactured jigs based on CT/MRI data — a lower-cost alternative to active navigation
- Machine learning integration: AI-driven preoperative planning and intraoperative guidance refinement
- Miniaturized handheld robotics (e.g., Navio): No large robotic arm required — surgeon holds a handheld robotic-guided burr; imageless; lower cost
- Soft tissue balancing modules: Real-time quantitative data on joint line tension and gap symmetry integrated into navigation displays
- Connectivity and data analytics: Cloud-linked systems enabling pooled outcome data for quality improvement and implant surveillance
Summary Table
| Parameter | Computer-Assisted Navigation | Conventional Instrumentation |
|---|---|---|
| Alignment accuracy | Higher (fewer outliers) | Variable |
| Operative time | Longer | Shorter |
| Cost | Higher | Lower |
| Learning curve | Required | Minimal |
| Implant survival | Not proven superior | Reference standard |
| Functional outcomes | Not consistently superior | Reference standard |
| Pin site risk | Present | None |
| Radiation (imageless) | Reduced | Standard fluoroscopy |
Key References (from the literature)
- Schwartz's Principles of Surgery, 11th Ed., p. 1936–1937 — Computer Navigation, Robotics, and Joint Arthroplasty
- Miller's Anesthesia, 10th Ed., Chapter 67 — Robotic-Assisted Knee Surgeries (RAKS) and Robotic-Assisted Hip Surgeries (RAHS)
- Rockwood and Green's Fractures in Adults, 10th Ed., 2025 — Periprosthetic fractures via tracking pin sites (systematic review)
- Kayani B, Konan S, Huq SS, et al. Robotic-arm assisted total knee arthroplasty. J Arthroplasty. 2018
- Pearle AD, Kendoff D, Stueber V, et al. Perioperative management of UKA using MAKO robotic arm system (MAKOplasty). Am J Orthop
Bottom line: Computer navigation in orthopaedics — from passive intraoperative guidance to semiactive robotic systems like MAKO — represents a genuine technological advance that consistently reduces component malalignment and alignment outliers in total joint arthroplasty. Its greatest current limitation is the absence of demonstrated superiority in implant survival or patient functional outcomes over technically precise conventional surgery. The field is evolving rapidly with AR navigation, AI planning, and handheld robotics poised to address current cost and workflow barriers.
This is a shared conversation. Sign in to Orris to start your own chat.