What is Crohn’s Disease
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from the authoritative GI textbook. Here is a thorough overview of Crohn's Disease:
Crohn's Disease
Definition & Overview
Crohn's disease (CD) is a chronic, relapsing inflammatory bowel disease (IBD) characterized by transmural (full-thickness), focal, and discontinuous inflammation that can affect any part of the GI tract from the mouth to the anus. It most commonly involves the terminal ileum and colon.
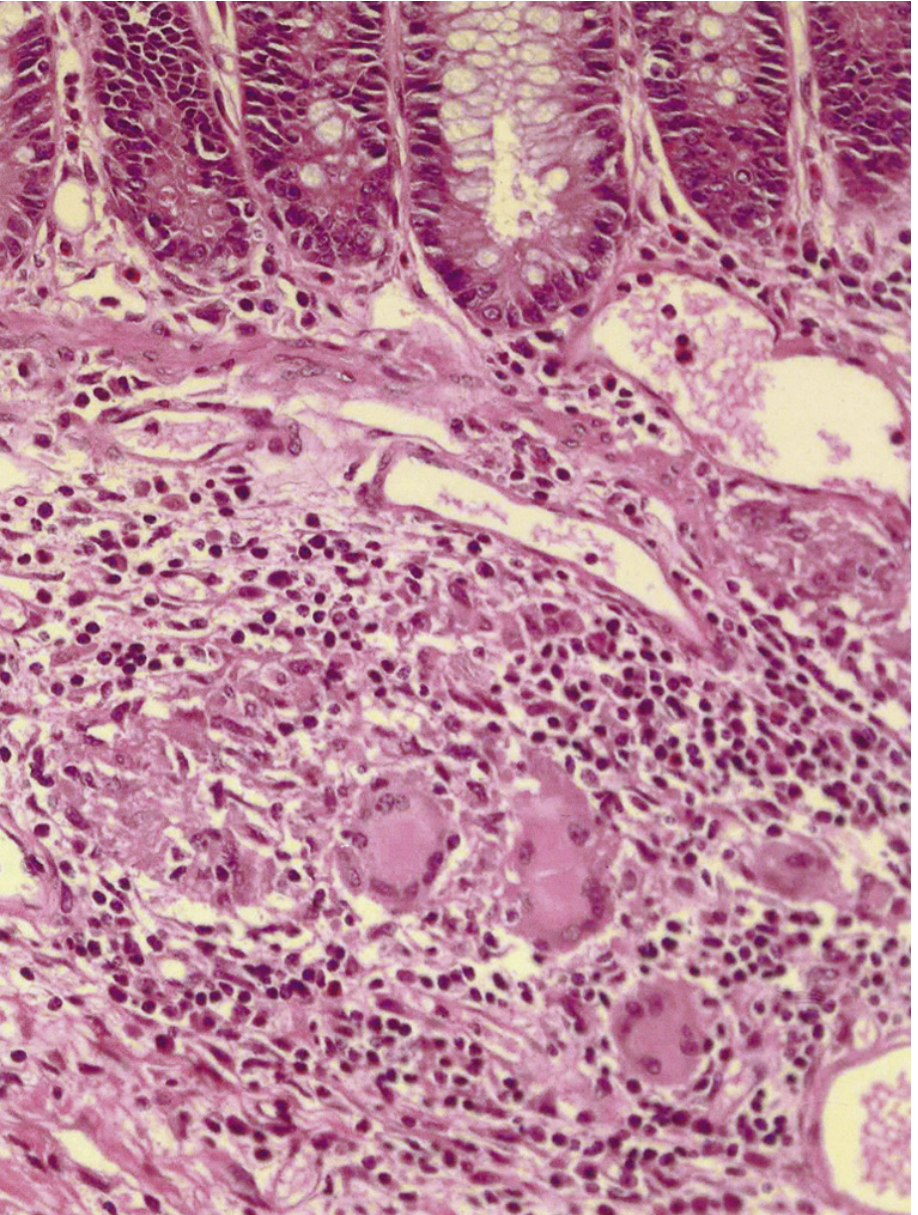
Pathology
Focal inflammation is the hallmark. Unlike ulcerative colitis, CD characteristically skips segments — inflamed bowel is interspersed with normal bowel. Even within a single biopsy, there is pronounced variability in inflammation.
Key pathological features:
-
Aphthous erosions — The earliest lesions; minute superficial mucosal breaks (up to 3 mm) surrounded by a halo of erythema, arising over lymphoid aggregates. They occur in normal-appearing mucosa and heal when the bowel is excluded from the fecal stream, strongly implicating luminal factors in pathogenesis.
-
Granulomas — Sarcoid-like, non-caseating collections of epithelioid histiocytes, lymphocytes, and eosinophils. Highly characteristic of CD (though not universal — found in 9–66% of cases depending on sampling). Unlike tuberculosis, there is no central necrosis and acid-fast stains are negative. Granulomas may be found in any layer of the intestine, mesenteric lymph nodes, and even extraintestinal sites (skin, eye, liver).
-
Transmural inflammation — Inflammation extends through all layers of the bowel wall, predisposing to fistulas, abscesses, and strictures.
Clinical Presentation
Symptoms depend on disease location and severity, but commonly include:
- Abdominal pain (especially right lower quadrant)
- Diarrhea (may be >10 bowel movements/day in severe flares)
- Weight loss and malnutrition
- Bloating
- Fever in active or complicated disease
Disease Activity Classification
Activity is classified as mild, moderate, or severe based on:
- Response to therapy
- Presence of systemic toxicity
- Abdominal tenderness, mass, or obstruction
- Degree of malnutrition, weight loss, and anemia
The Crohn's Disease Activity Index (CDAI) integrates subjective symptoms and objective findings. Remission = CDAI < 150; a response to therapy = decrease in CDAI ≥100 points.
Biomarkers & Monitoring
- CRP (C-reactive protein) — correlates with clinical and endoscopic disease activity; elevated levels indicate active disease or infectious complication
- Fecal calprotectin — sensitive marker of intestinal inflammation; pooled sensitivity 88%, specificity 67% for CD (vs. endoscopically active disease). Also correlates with relapse and response to biologic therapy.
- Fecal lactoferrin — similarly useful
- ESR — useful but less specific
Symptoms do not always correlate with objective disease activity. Mucosal healing (assessed by endoscopy and biomarkers) has emerged as a therapeutic target beyond pure symptom control.
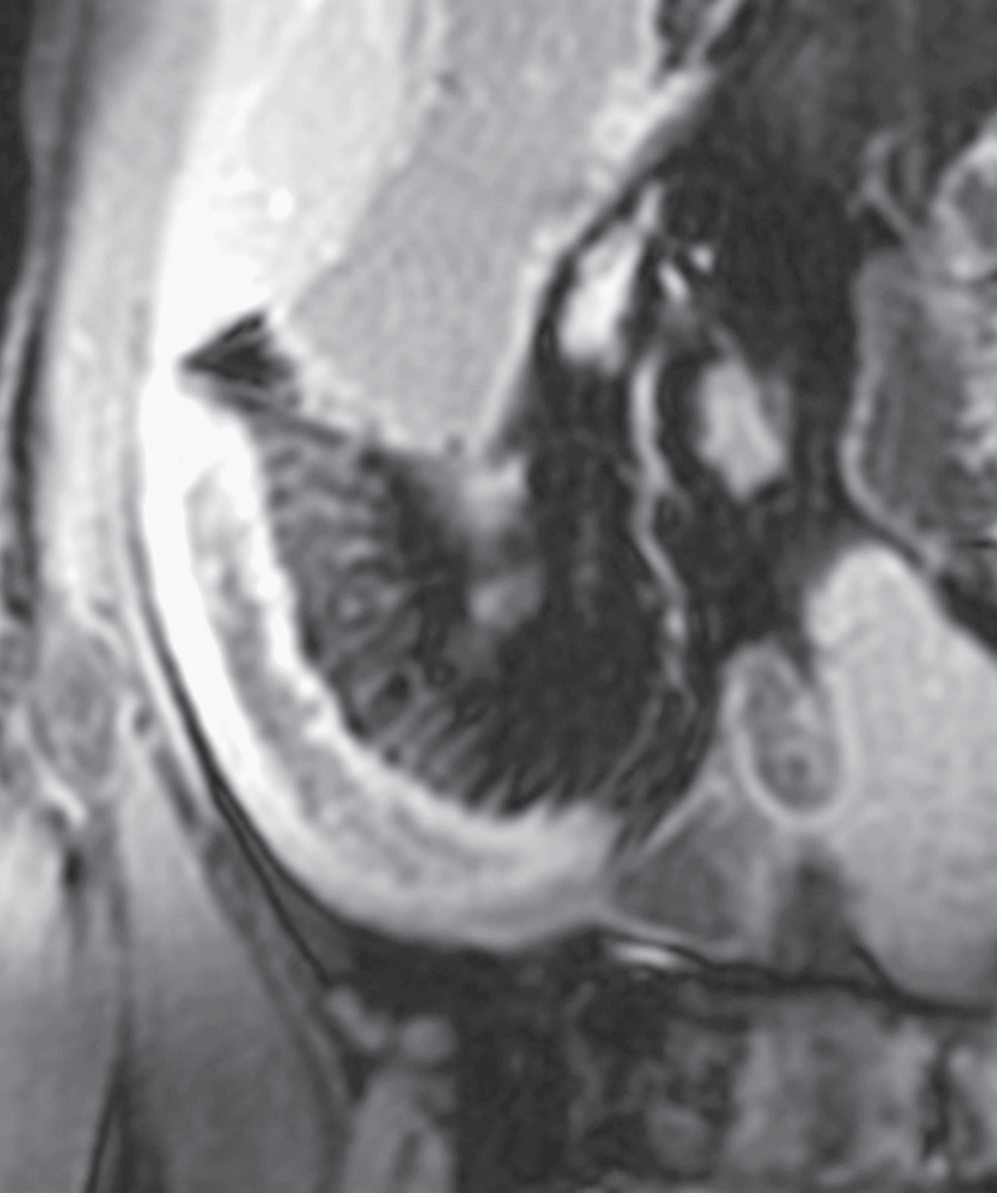
Imaging
MR enterography is a key modality. Findings in active CD include:
- Mural hyperenhancement
- Mural thickening
- "Comb sign" — engorged peri-enteric vasculature medial to the inflamed loop, resembling the teeth of a comb
CT may show thickened distal ileum with mesenteric engorgement and stranding, sometimes with proximal dilatation.
Complications
| Complication | Notes |
|---|---|
| Strictures / obstruction | Fibrotic narrowing; chronic partial SBO more common than complete |
| Fistulas | Enteroenteric, enterocutaneous, perianal — due to transmural disease |
| Abscesses | Intra-abdominal; increasingly managed with percutaneous drainage + antibiotics |
| Perianal disease | Fissures, fistulas, abscesses |
| Short bowel syndrome | Risk increases with repeated resections |
| Intestinal malignancy | Long-standing IBD increases risk |
| Toxic megacolon | Rare but surgical emergency |
Up to 75% of patients with CD are at risk for adhesions, incisional hernias, and internal hernias from prior surgery.
Treatment
Medical
- Corticosteroids — induce remission in active disease
- Immunomodulators (azathioprine, 6-mercaptopurine, methotrexate) — maintenance
- Biologics (anti-TNF agents like infliximab, adalimumab; anti-integrins; anti-IL-12/23) — for moderate-to-severe or refractory disease
Surgical
Surgery is integral but not curative. Key principles:
- Preserve intestinal length — wide margins do not reduce recurrence risk and repeated resection risks short bowel syndrome
- Indications: intra-abdominal abscess, medically intractable fistula, fibrotic stricture with obstruction, toxic megacolon, dysplasia/cancer, glucocorticoid-refractory disease
- Most common procedure: ileocecal resection with primary anastomosis (often laparoscopic)
- Bowel-sparing approaches (stricturoplasty) preferred over resection where possible
Surgical statistics:
- ~75% of patients undergo at least one abdominal operation over 20 years
- Risk of surgery at 1, 5, and 10 years: 16%, 33%, 47% respectively
- ~30% require a second operation within 5 years of the first
- Rates of surgery have declined significantly over the past 6 decades, likely reflecting more effective and earlier medical therapy
— Sleisenger and Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.