How to differentiate between sah and edh
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative sources. Let me compile a thorough answer.
Differentiating SAH vs EDH
These two are fundamentally different hemorrhages — SAH (subarachnoid hemorrhage) occurs in the subarachnoid space (between arachnoid and pia), while EDH (epidural hematoma) occurs between the skull and the dura. Their etiology, clinical course, and imaging appearance are distinct.
1. Anatomical Location
| Feature | EDH | SAH |
|---|---|---|
| Space | Between skull and dura (potential space) | Between arachnoid and pia (subarachnoid cisterns, sulci) |
| Layers involved | Outside dura | Outside brain parenchyma, inside dura |
| Blood spreads | Focally (bounded by dural attachments at sutures) | Diffusely through CSF pathways, cisterns, and sulci |
2. Etiology & Source of Bleeding
| Feature | EDH | SAH |
|---|---|---|
| Primary cause | Trauma (almost always) | Trauma OR spontaneous (aneurysm rupture, AVM) |
| Vessel source | Middle meningeal artery (most common — temporal/temporoparietal trauma) | Cortical surface vessels, ruptured aneurysm (Circle of Willis), AVM |
| Associated fracture | Temporal skull fracture crosses middle meningeal artery in adults | Usually absent in spontaneous SAH |
| Blood type | Arterial (high-pressure → rapid expansion) | Mixed arterial/venous; aneurysmal → often arterial |
Blunt trauma to the temporal or temporoparietal area with an associated skull fracture and middle meningeal arterial disruption is the primary mechanism of EDH. — Tintinalli's Emergency Medicine
Subarachnoid hemorrhage almost always accompanies parenchymal trauma but can also develop spontaneously secondary to vascular anomalies. — Robbins, Cotran & Kumar Pathologic Basis of Disease
3. Clinical Presentation
| Feature | EDH | SAH |
|---|---|---|
| Classic history | Trauma → LOC → lucid interval → rapid neurologic deterioration | Spontaneous: sudden "thunderclap" headache ("worst headache of life") |
| Lucid interval | Present in ~50% (NOT pathognomonic — can also occur with other mass lesions) | Not typically present; onset is abrupt |
| Headache | Present, but trauma-related | Severe, sudden onset; often with photophobia, meningismus |
| LOC | May be brief initially, worsens rapidly | Rapid deterioration; may be sudden |
| Meningeal signs | Absent | Present — neck stiffness, Kernig/Brudzinski signs (due to blood in CSF irritating meninges) |
| Speed of deterioration | Hours (arterial pressure → herniation rapidly) | Variable — rapid if large aneurysm rupture |
| Underlying brain injury | Often absent (brain parenchyma usually intact) | Often concurrent parenchymal injury in traumatic SAH |
The classic history of an EDH involves a significant blunt head trauma with loss of consciousness, followed by a lucid period and subsequent rapid neurologic demise. This clinical presentation occurs in a minority of cases. — Tintinalli's Emergency Medicine
4. CT Imaging (Key Differentiator)
EDH — Biconvex (lenticular/football) hyperdense lesion

- Shape: Biconvex (lenticular, football-shaped) — bounded by dural attachments at sutures, cannot cross suture lines
- Location: Most commonly temporal region
- Density: Hyperdense (white) acutely — uniform
- Mass effect: Midline shift, brain compression
- Does NOT cross suture lines
SAH — Blood filling cisterns and sulci
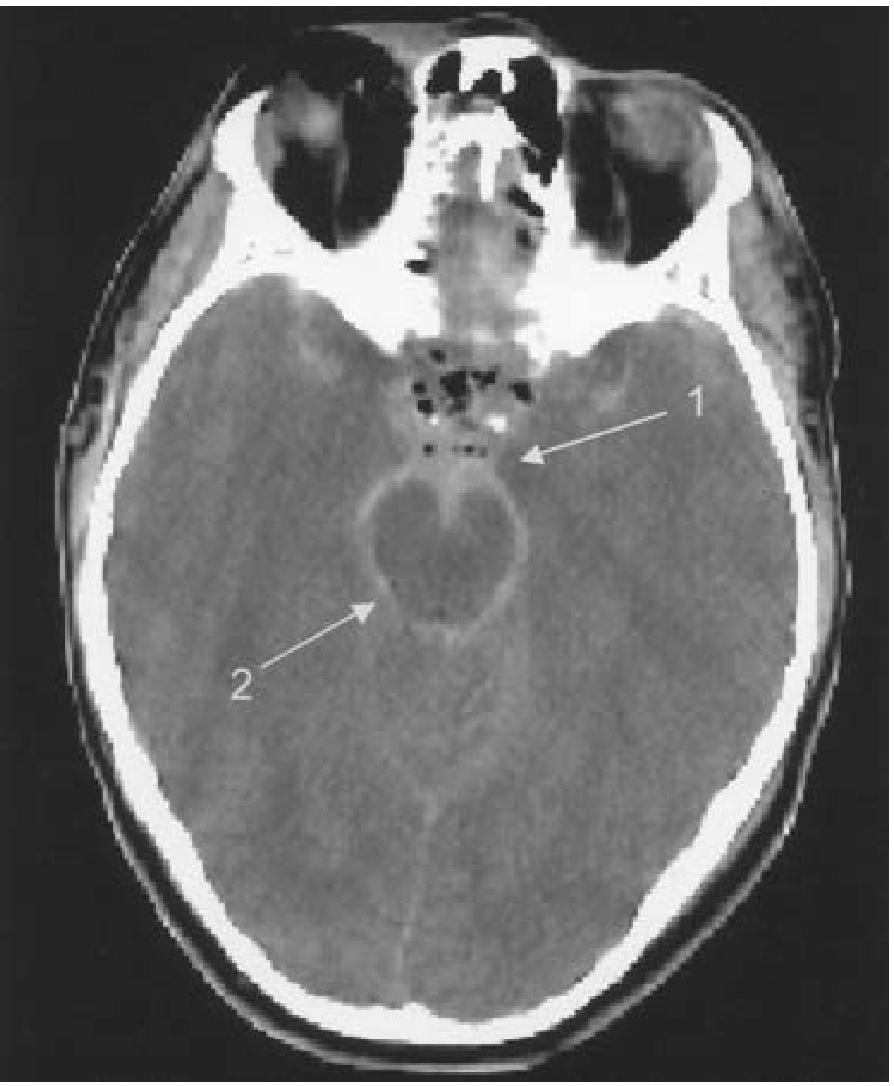
- Shape: Diffuse — fills sulci, cisterns (sylvian fissure, interhemispheric fissure, basal cisterns)
- Location: Spreads throughout subarachnoid space; aneurysmal SAH often at base of brain
- Density: Hyperdense in sulci and cisterns ("star sign" or basal cistern hyperdensity)
- Can cross suture lines (because blood is in CSF, not a mass)
- CT may be negative in ~15% of SAH within 12–24h → LP required if CT negative and clinical suspicion high (xanthochromia after 2–4 hrs)
5. LP / CSF Findings
| Feature | EDH | SAH |
|---|---|---|
| LP role | Not typically indicated (CT diagnostic) | Critical when CT is negative — shows xanthochromia or persistent RBCs in CSF |
| CSF | Normal (blood is extradural) | Xanthochromia, uniformly bloody (non-clearing), elevated opening pressure |
6. Management & Urgency
| Feature | EDH | SAH |
|---|---|---|
| Urgency | Neurosurgical emergency — fatal herniation within hours without drainage | Urgent — neurosurgical/neurointerventional evaluation |
| Treatment | Surgical evacuation (craniotomy) | Aneurysm clipping/coiling; nimodipine for vasospasm prevention; ICP management |
| Prognosis | Excellent if evacuated before herniation — underlying brain often intact | More guarded; secondary injury from vasospasm (occurs 4–14 days post-ictus) is a major complication |
The high-pressure arterial bleeding of an EDH can lead to herniation within hours after injury. Underlying injury of the brain parenchyma is often absent; full recovery may be expected if the hematoma is evacuated prior to herniation. — Tintinalli's Emergency Medicine
Secondary injury may emerge in SAH and is associated with vasospasm. — Robbins, Cotran & Kumar Pathologic Basis of Disease
Summary Table
| Feature | EDH | SAH |
|---|---|---|
| Cause | Trauma (MMA injury) | Trauma or spontaneous (aneurysm/AVM) |
| Blood source | Arterial (middle meningeal a.) | Aneurysm, cortical vessels |
| Space | Epidural (skull ↔ dura) | Subarachnoid (arachnoid ↔ pia) |
| Classic history | Lucid interval after trauma | Sudden "thunderclap" headache |
| Meningismus | Absent | Present |
| CT shape | Biconvex, focal | Diffuse cisterns/sulci hyperdensity |
| Crosses sutures? | No | Yes |
| LP | Not needed | Xanthochromia if CT negative |
| Urgency | Hours (arterial) | Urgent (vasospasm risk) |
| Prognosis | Good if early surgery | Variable; vasospasm is key risk |
Sources: Tintinalli's Emergency Medicine, Robbins, Cotran & Kumar Pathologic Basis of Disease, Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.