Knee ligaments and their injury
Reading File
Finding Sources
Finding Sources
Searching PubMed
"knee ligament" AND injury
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compose the full answer.
Knee Ligaments and Their Injuries
Anatomy Overview
The knee is stabilized by four primary ligaments arranged in two functional pairs. The image below shows their arrangement from anterior and posterior views:
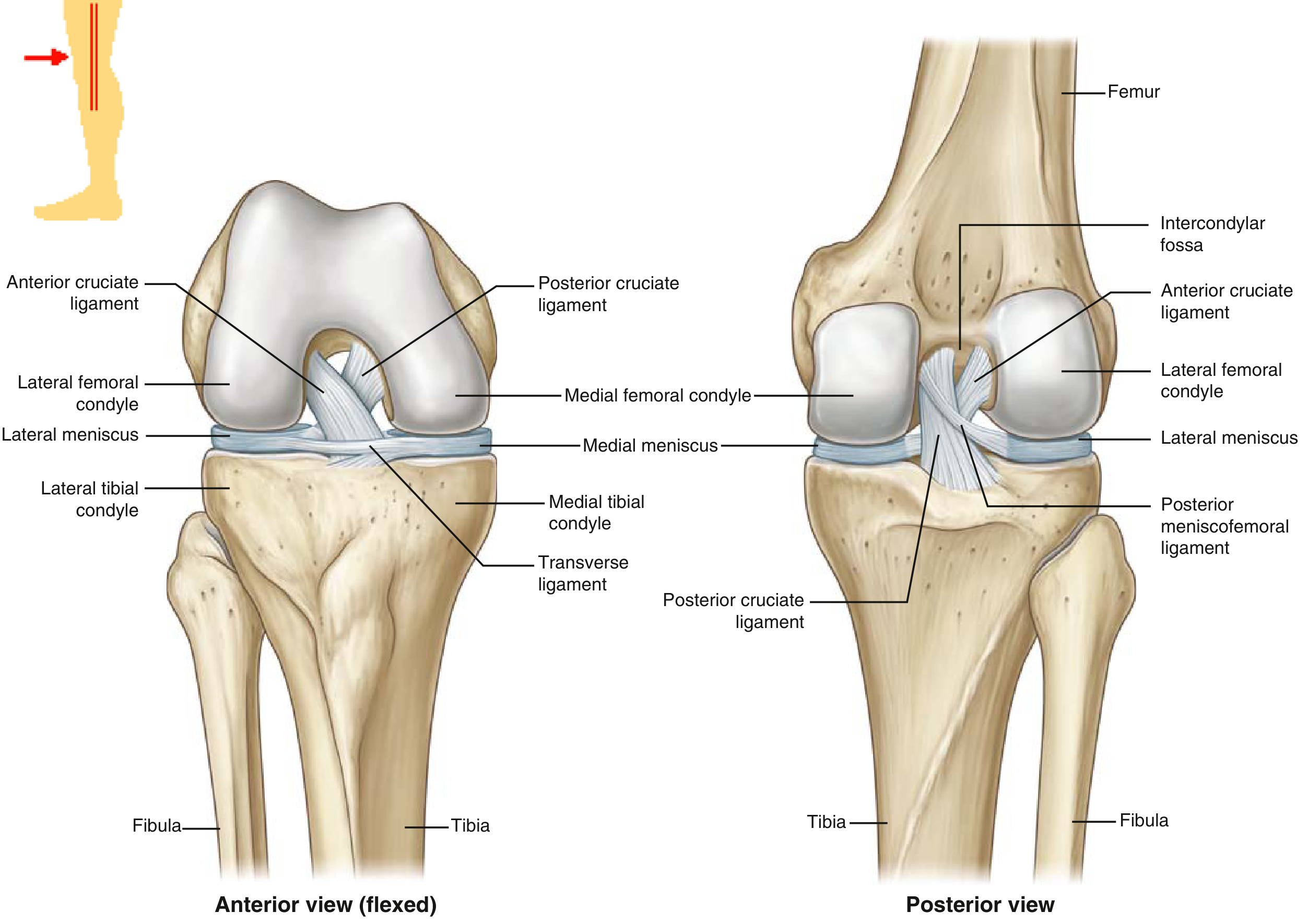
1. Anterior Cruciate Ligament (ACL)
Anatomy
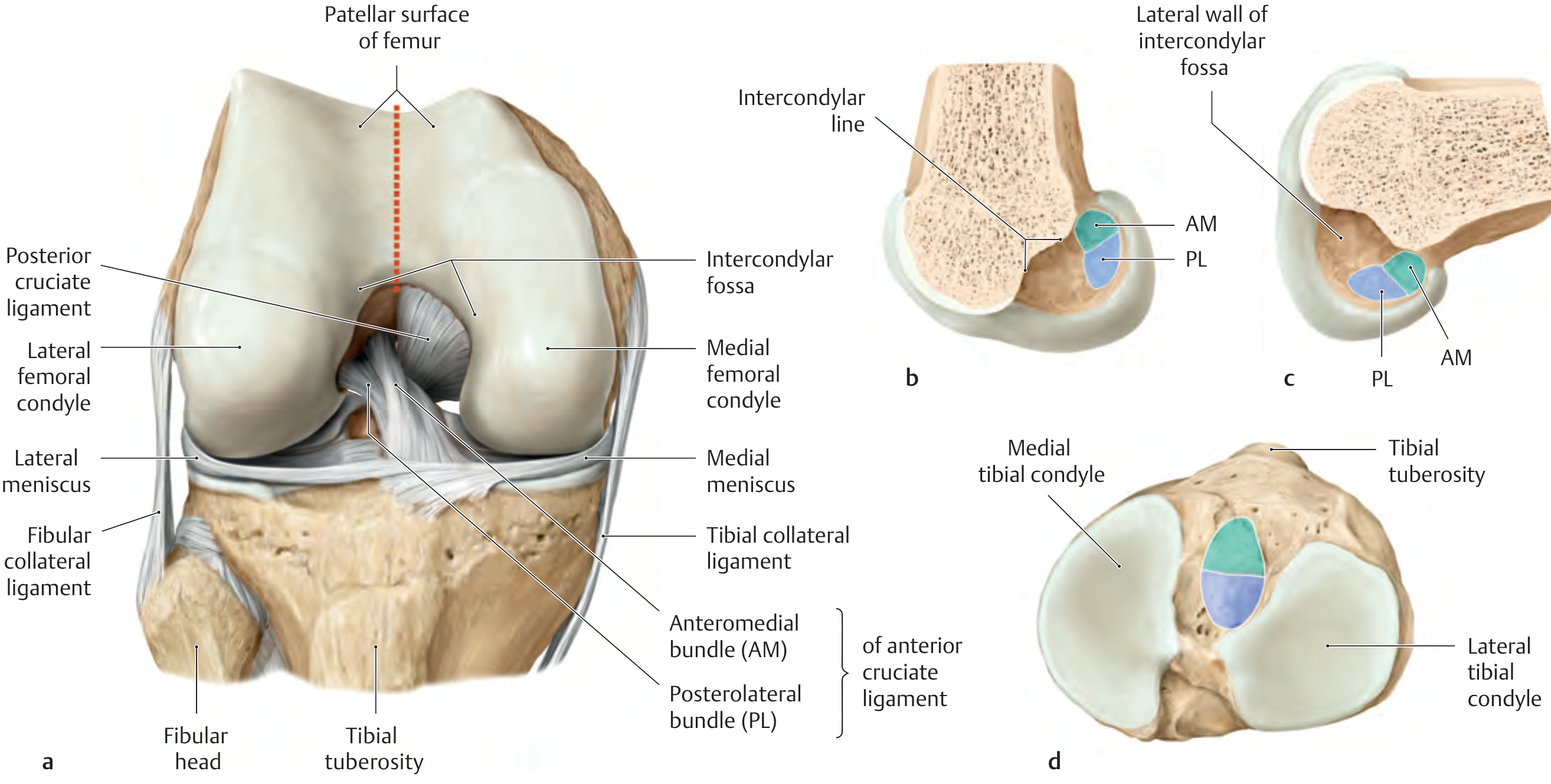
The ACL runs from the posterior lateral intercondylar fossa of the femur to the anterior aspect of the tibial eminence. It has two distinct fiber bundles:
- Anteromedial (AM) bundle (~38 mm long): primary anterior restraint against tibial translation; taut in flexion; evaluated by the Lachman and anterior drawer tests
- Posterolateral (PL) bundle (~20 mm long): rotatory restraint; taut in extension; evaluated by the pivot shift test
The ACL courses parallel to the roof of the intercondylar notch on sagittal imaging, and its in-situ force is highest at 30 degrees of flexion in response to anterior tibial load.
Tensile strength: ~2,200-2,500 N (in young individuals)
ACL Injury
Epidemiology: ACL ruptures account for 40-50% of all knee ligament injuries. Female athletes have a 2-8x higher risk than males, attributed to:
- Different (more erect) landing biomechanics and greater valgus loading on landing
- Increased quadriceps-to-hamstring strength ratio causing greater anterior shear
- Smaller ligament cross-section, smaller femoral notch, and greater generalized laxity
- Highest-risk sports: skiing, soccer, basketball, football
Mechanism: Typically a valgus load with internal tibial rotation and anterior tibial translation while the knee is near full extension. Often a non-contact pivoting/deceleration injury. Hyperextension and marked internal rotation can also cause isolated ACL disruption.
Presentation:
- Audible "pop" at the time of injury
- Rapid hemarthrosis (within 12 hours)
- Need to be "carried off" the field
- Giving-way/instability on pivoting
Clinical tests:
| Test | Technique | What it detects |
|---|---|---|
| Lachman test (most sensitive) | Anterior force on tibia with knee at 30° flexion, femur stabilized | AM bundle / anterior translation |
| Anterior drawer test | Tibia pulled anteriorly at 90° knee flexion | Anterior translation |
| Pivot shift test | Valgus + internal rotation while slowly flexing; "clunk" at 20-40° | PL bundle / rotatory instability |
Imaging: MRI achieves ~95% accuracy. Signs of ACL rupture include: abnormal horizontal course, wavy/irregular appearance, fluid-filled gaps in a discontinuous ligament. Secondary signs: lateral compartment bone contusions (the "kissing contusion"), anterior tibial subluxation, and buckling of the PCL.
Associated injuries:
- Acute lateral meniscal tears (more common acutely); medial meniscal tears with chronic ACL deficiency
- MCL injury in ~25% of cases
- Posterolateral corner (PLC) injury in ~10% - frequently missed, and its non-recognition is a leading cause of ACL reconstruction failure
- The "unhappy triad" (ACL + MCL + medial meniscus) is a classic combination
Management:
- Initial: RICE, brace, analgesia, physiotherapy, swelling reduction
- Conservative: Appropriate for low-demand patients without instability
- Surgical (ACL reconstruction): Indicated for young/high-demand athletes, multiligament injuries, persistent instability. Deferred until acute inflammation resolves and full ROM is restored
- Common grafts: bone-patellar tendon-bone (BTB, ~2,900 N), quadrupled hamstring (~4,000 N - strength depends on fixation)
- There is currently no high-level evidence that ACL reconstruction reduces the long-term risk of arthritis; chondral and meniscal injuries at the time of rupture are the main predictors of arthritic change
2. Posterior Cruciate Ligament (PCL)
Anatomy
The PCL is the strongest ligament in the knee (tensile strength ~2,500-3,000 N), running from the posterior tibial plateau to the medial wall of the intercondylar notch. It appears as a homogeneously hypointense, gently curving structure on sagittal MRI in extension.
PCL Injury
Mechanism: Requires significant trauma. Classic mechanisms:
- "Dashboard injury": direct posterior blow to the flexed knee in a motor vehicle accident
- Direct blow to the front of the tibia with the knee flexed
- Hyperflexion under load
Clinical tests:
- Posterior drawer test: posterior force on tibia at 90° flexion
- Posterior sag sign: spontaneous posterior subluxation of tibia at 90° flexion - loss of the medial tibial step-off
- Quadriceps active test: patient extends knee at 60° flexion with foot on table; visible tibial reduction = positive
Associated injury: PCL injuries are frequently accompanied by posterolateral corner (PLC) injury - a combination that severely compromises knee stability.
MRI: Discontinuity or fluid signal within the PCL substance indicates a tear.
3. Medial Collateral Ligament (MCL)
Anatomy
The MCL has three layers:
- Superficial MCL (sMCL): primary stabilizer against valgus stress; tensile strength ~550 N
- Deep MCL (dMCL): tightly adherent to the medial meniscus; ~100 N
- Posterior oblique ligament (POL): ~250 N; resists internal rotation
Grading of MCL injuries:
| Grade | Description | Healing |
|---|---|---|
| I | Pain, no laxity (stretching only) | 11-20 days |
| II | Partial tear, increased laxity with firm endpoint | 11-20 days |
| III | Complete tear, no endpoint | 5-7 weeks (some never heal) |
Mechanism: Valgus stress to the knee (direct blow to the lateral side)
Clinical test: Valgus stress test at 0° and 30° flexion (laxity at 30° = isolated MCL; laxity at 0° = MCL + cruciate involvement)
MRI: Grades I-II show periligamentous edema with intact fibers. Grade III shows frank discontinuity or thickening. Distal MCL tears can sometimes form a "Stener-like lesion" with interposed tissue blocking healing - recent systematic review data (PMID: 40583380) show good outcomes with surgical treatment for these.
Management: Grade I/II - conservative (brace, physio). Grade III isolated - usually conservative. Grade III combined with ACL/PCL injury - may require repair/reconstruction.
4. Lateral Collateral Ligament (LCL) / Fibular Collateral Ligament
Anatomy
The LCL runs from the lateral femoral epicondyle to the fibular head. It is cord-like and does not attach to the lateral meniscus (unlike the MCL and medial meniscus). Tensile strength ~750 N. It is part of the posterolateral corner (PLC) complex, along with the popliteus tendon, popliteofibular ligament, and biceps femoris.
Mechanism: Varus stress or hyperextension with external rotation
Clinical test: Varus stress test at 0° and 30° flexion; dial test for posterolateral rotation
Key point: Isolated LCL injury is rare; it usually occurs as part of a PLC or multi-ligament injury. Unrecognized PLC injury is a leading cause of cruciate reconstruction failure.
5. Anterolateral Ligament (ALL)
A relatively recently described structure on the anterolateral aspect of the knee, running from the lateral femoral condyle to the proximal tibia. It is thought to contribute to rotatory stability. Interest in the ALL has grown in the context of ACL reconstruction, as injury to it may contribute to residual pivot-shift after standard ACL repair.
Ligament Healing Biology
Healing follows four overlapping phases (from Campbell's Operative Orthopaedics, 15th Ed):
- Hemorrhage - hematoma formation
- Inflammation - inflammatory cells clear necrotic tissue, form granulation tissue
- Repair - fibroblasts produce extracellular matrix; immature collagen forms (begins ~5-7 days)
- Remodeling - collagen aligns along the long axis; begins weeks after injury, lasts months to years
Even after apparent healing, the repaired ligament has more collagen fibrils of smaller diameter and different "crimping" patterns compared to the native ligament - explaining persistent functional differences.
The ACL heals poorly due to its intra-articular, synovial environment (poor vascular supply, no scaffolding), which is why it typically requires reconstruction rather than repair. The MCL heals reliably because it is extrasynovial with a good blood supply.
Tensile Strength Summary
| Ligament | Tensile Strength |
|---|---|
| PCL | ~2,500-3,000 N |
| ACL | ~2,200-2,500 N |
| LCL | ~750 N |
| sMCL | ~550 N |
| POL | ~250 N |
| dMCL | ~100 N |
Key Clinical Pearls
- A hemarthrosis after a knee injury is an ACL tear until proven otherwise (~70% of acute hemarthroses)
- The Lachman test (30° flexion) is more sensitive than the anterior drawer test (90° flexion) for ACL injury - at 90°, the posterior horn of the medial meniscus acts as a secondary stabilizer masking translation
- Bone contusions on MRI (lateral femoral condyle + posterior lateral tibial plateau) are a hallmark of acute ACL injury and typically resolve in 6-12 weeks
- The posterior horn of the medial meniscus is a major secondary stabilizer against anterior translation in ACL-deficient knees - its loss dramatically accelerates instability
- The four-bar linkage model of knee kinematics explains why the cruciate ligaments are isometric only at a single flexion axis, and why graft placement must be anatomic
Sources: Miller's Review of Orthopaedics, 9th Ed | Bailey & Love's Short Practice of Surgery, 28th Ed | Campbell's Operative Orthopaedics, 15th Ed 2026 | THIEME Atlas of General Anatomy & Musculoskeletal System | Firestein & Kelley's Textbook of Rheumatology (2022) | Rockwood & Green's Fractures in Adults, 10th Ed 2025
This is a shared conversation. Sign in to Orris to start your own chat.