Cardiac cycle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive material. Here is the full, detailed answer:
The Cardiac Cycle
The cardiac cycle refers to the sequence of electrical and mechanical events that occur during a single heartbeat - from the beginning of one beat to the beginning of the next. At a resting heart rate of 72 beats/min, the cycle lasts approximately 0.833 seconds (1/72 min). - Guyton and Hall Textbook of Medical Physiology
Each cycle is initiated by spontaneous action potential generation in the sinoatrial (SA) node in the superior lateral wall of the right atrium. The impulse travels through both atria, then through the AV node and AV bundle to the ventricles - with a >0.1 second delay at the AV node that allows the atria to contract before the ventricles, acting as "primer pumps." - Guyton and Hall
Phases of the Cardiac Cycle (Wiggers Diagram)
Costanzo's physiology divides the cycle into 7 phases (A through G). The classic Wiggers diagram (Fig. 4.25 from Costanzo) shows all simultaneous events: left ventricular pressure, aortic pressure, left atrial pressure, ventricular volume, heart sounds, venous pulse, and ECG.
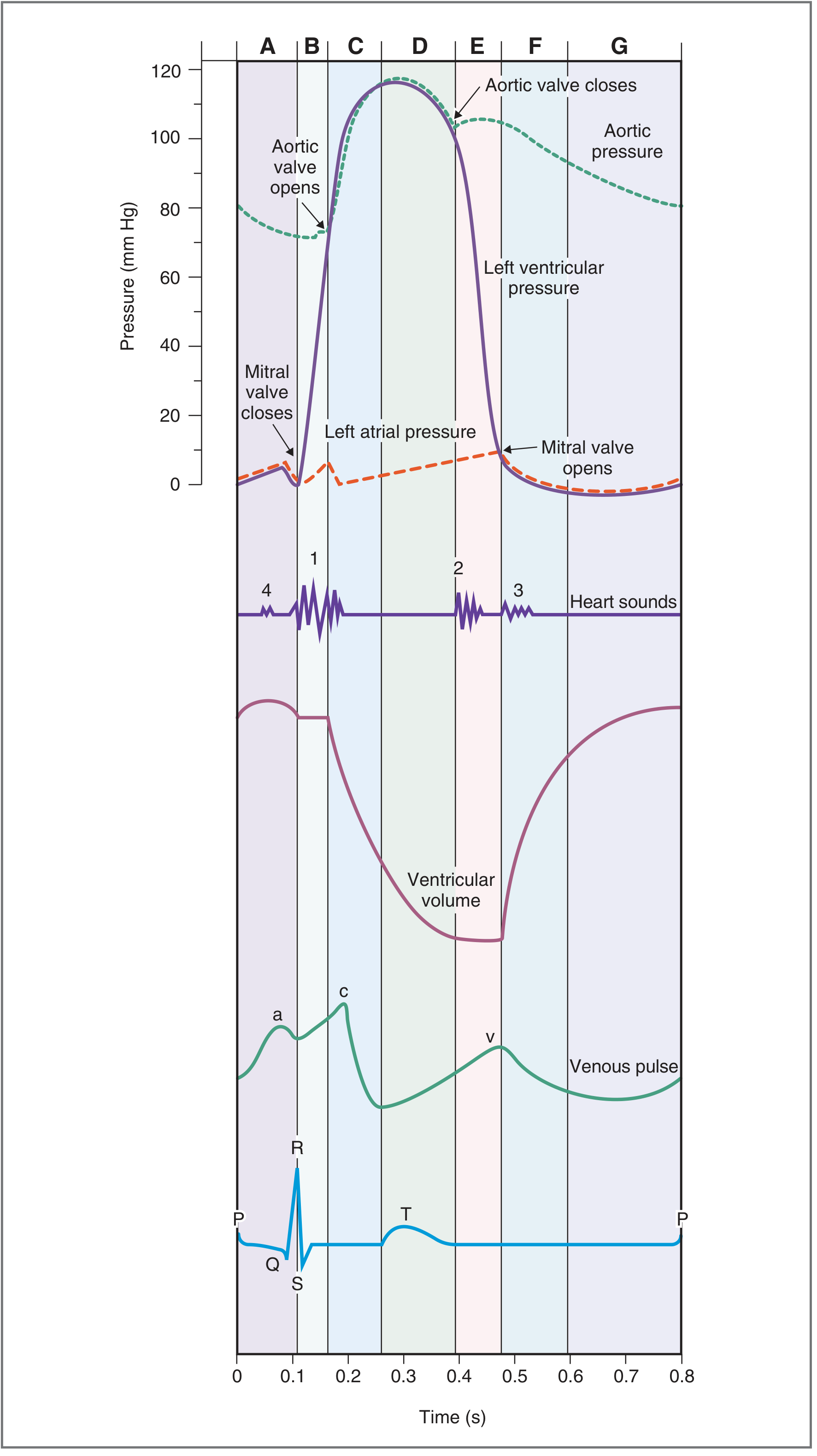
Phase A - Atrial Systole
- ECG: P wave (atrial depolarization)
- Valves: Mitral (AV) valve already open; aortic valve closed
- Events: The left atrium contracts, propelling additional blood into the left ventricle. This accounts for the final ~30% of ventricular filling (about 70% of filling occurs passively earlier in diastole). Left atrial pressure rises and this pressure wave is reflected back to the jugular veins as the "a" wave of the venous pulse.
- Heart sounds: S4 (not audible normally; heard in ventricular hypertrophy where compliance is reduced - the atrium contracts against a stiff ventricle)
- The ventricle reaches its maximum volume at the end of atrial systole = end-diastolic volume (EDV) ~130 mL
- Costanzo Physiology 7th Edition, p. 160-161
Phase B - Isovolumetric Ventricular Contraction (IVC)
- ECG: QRS complex (ventricular depolarization)
- Valves: Mitral valve closes (as LV pressure exceeds LA pressure); aortic valve remains closed - so all valves are closed
- Events: Ventricular muscle contracts vigorously. Intraventricular pressure rises sharply, but because all valves are closed, ventricular volume does not change (hence "isovolumetric"). This phase lasts approximately 0.05 seconds, until LV pressure exceeds aortic diastolic pressure (~80 mmHg).
- The AV valves bulge into the atria during this phase, causing a small, sharp rise in atrial pressure seen as the "c" wave on the venous pulse.
- Heart sounds: S1 ("lub") - caused by closure of the mitral and tricuspid valves. Mitral closes slightly before tricuspid, producing physiological splitting of S1.
- Costanzo Physiology 7th Edition, p. 162; Ganong's Review, p. 539
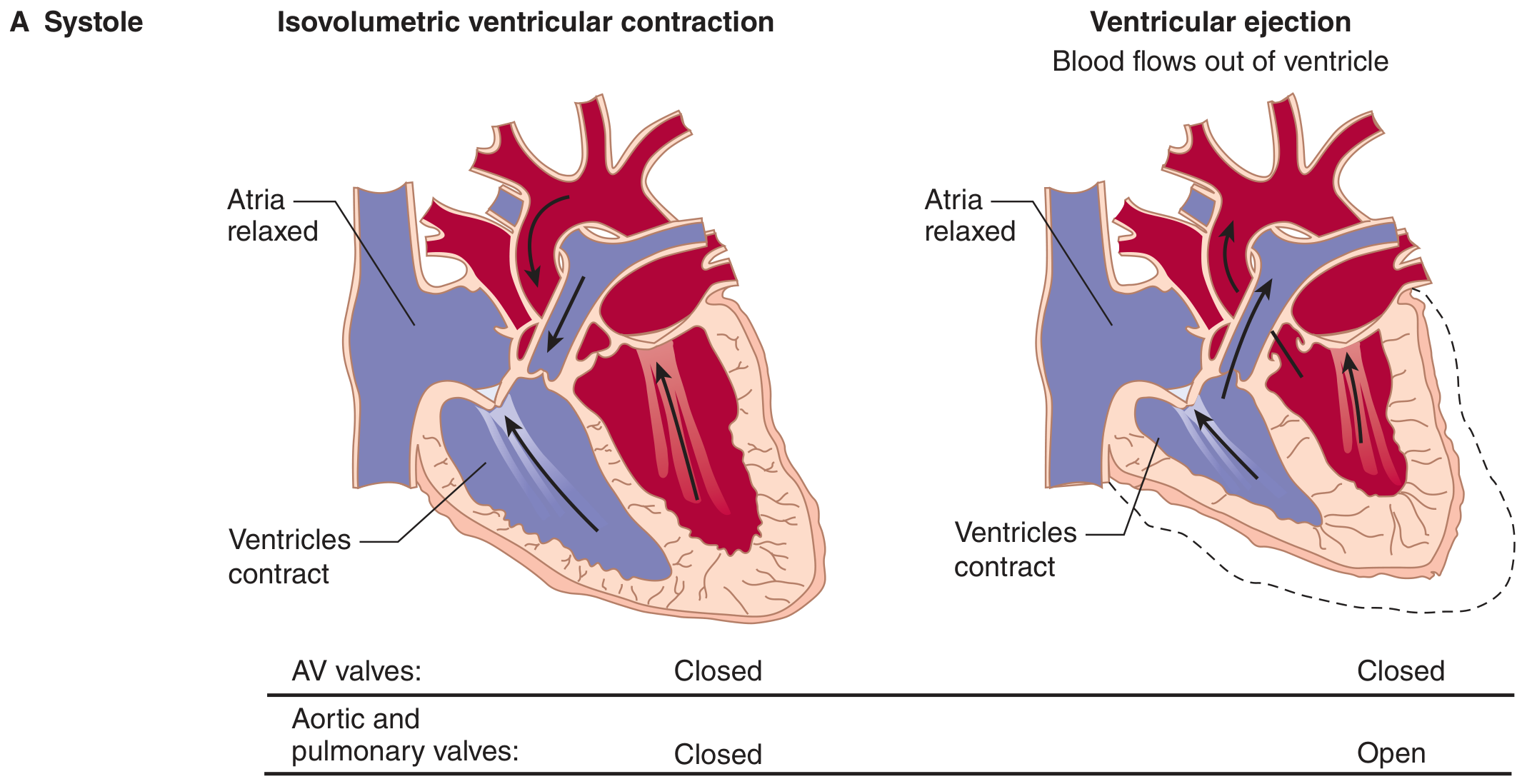
Phase C - Rapid Ventricular Ejection
- ECG: ST segment
- Valves: Aortic (and pulmonary) valve opens when LV pressure exceeds aortic pressure; mitral valve remains closed
- Events: Blood is rapidly ejected into the aorta. LV pressure and aortic pressure both rise steeply and reach their peak (~120 mmHg in the LV, ~120 mmHg in the aorta). Ventricular volume falls rapidly as most of the stroke volume is ejected. Atrial filling from the pulmonary veins begins, so left atrial pressure slowly rises.
- Heart sounds: None
- Peak LV pressure: ~120 mmHg (left), ~25 mmHg (right)
Phase D - Reduced Ventricular Ejection
- ECG: T wave begins (ventricular repolarization starts)
- Valves: Aortic valve still open
- Events: The ventricles begin to repolarize and ventricular pressure falls. Blood continues to be ejected but at a reduced rate. Blood "runs off" into the peripheral arteries faster than the ventricle can add it, so aortic pressure begins to fall. Ventricular volume reaches its minimum = end-systolic volume (ESV) ~50 mL.
- Ejection fraction = (EDV - ESV) / EDV = (130 - 50)/130 ≈ ~65% - a key index of ventricular function.
- Stroke volume = EDV - ESV = ~80 mL
- Ganong's Review of Medical Physiology, p. 540
Phase E - Isovolumetric Ventricular Relaxation (IVR)
- ECG: After T wave (ventricles fully repolarized)
- Valves: Aortic valve closes (LV pressure falls below aortic pressure); mitral valve remains closed - again all valves are closed
- Events: Ventricular pressure falls rapidly but volume does not change (all valves closed). This lasts until LV pressure falls below left atrial pressure, at which point the mitral valve opens. The brief period just before aortic valve closure (when momentum keeps blood moving forward despite falling pressure) is called protodiastole (~0.04 s).
- Heart sounds: S2 ("dup") - caused by closure of the aortic then pulmonary valve.
- Physiological splitting of S2: Aortic closes before pulmonic. On inspiration, intrathoracic pressure falls → increased venous return to the right heart → increased RV stroke volume (Frank-Starling) → prolonged RV ejection time → delayed pulmonic valve closure → wider splitting of S2. This is normal.
- Costanzo Physiology 7th Edition, p. 162
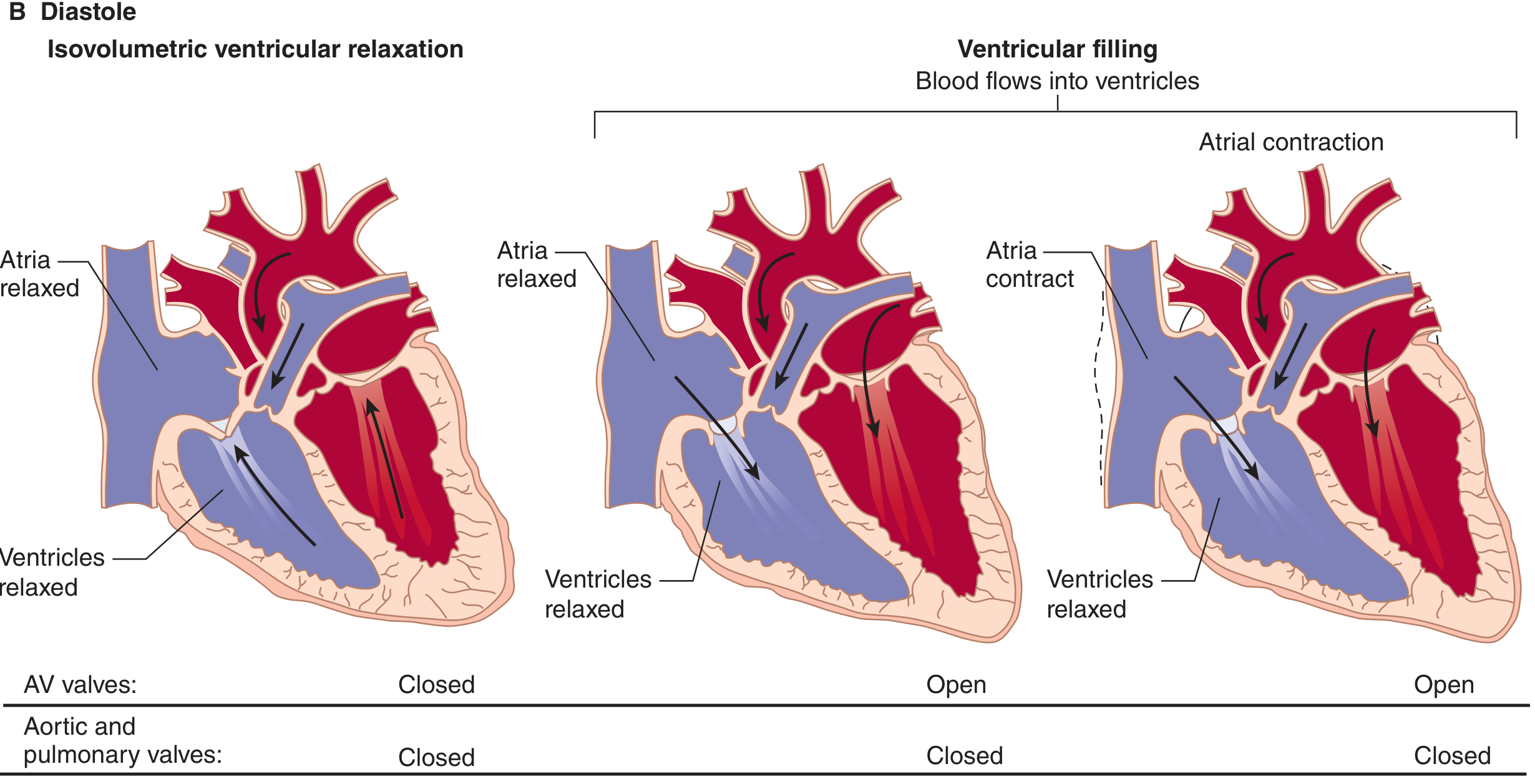
Phase F - Rapid Ventricular Filling
- ECG: No corresponding wave
- Valves: Mitral valve opens (LV pressure falls below LA pressure)
- Events: Blood rushes from atrium into ventricle passively down a pressure gradient. Ventricular volume increases rapidly. Ventricular pressure remains low and relatively constant. Atrial pressure drops as blood moves into the ventricle, then the "v" wave of the venous pulse (passive atrial filling during systole) terminates as blood drains through the open mitral valve.
- Heart sounds: S3 ("ventricular gallop") - produced by rapid filling of the ventricle. Normal in children and young adults; abnormal in older adults and may indicate heart failure or a dilated, poorly compliant ventricle.
Phase G - Reduced Ventricular Filling (Diastasis)
- ECG: Isoelectric (interval before next P wave)
- Valves: Mitral valve still open
- Events: Filling continues at a slower rate as the pressure gradient between atrium and ventricle equalizes. This is the longest phase of the cardiac cycle and is the one most affected by changes in heart rate. Increases in heart rate shorten or eliminate diastasis, reducing end-diastolic volume and, by the Frank-Starling mechanism, reducing stroke volume.
- Heart sounds: None
- Costanzo Physiology 7th Edition, p. 162
Summary Table of the 7 Phases
| Phase | ECG | Valves | Heart Sound | Key Feature |
|---|---|---|---|---|
| A Atrial Systole | P wave | MV open, AoV closed | S4 (abnormal) | "a" wave; final ventricular filling |
| B Isovolumetric Ventricular Contraction | QRS | All closed | S1 | Pressure rises, volume constant |
| C Rapid Ventricular Ejection | ST segment | AoV opens | — | Peak pressure, most SV ejected |
| D Reduced Ventricular Ejection | T wave | AoV open | — | ESV reached; aortic pressure falls |
| E Isovolumetric Ventricular Relaxation | After T wave | All closed | S2 | Pressure falls, volume constant |
| F Rapid Ventricular Filling | — | MV opens | S3 (if abnormal) | "v" wave ends; passive filling |
| G Diastasis | — | MV open | — | Slow filling; longest phase |
AoV = aortic valve; MV = mitral valve; SV = stroke volume; ESV = end-systolic volume
Pressure-Volume Loop of the Left Ventricle
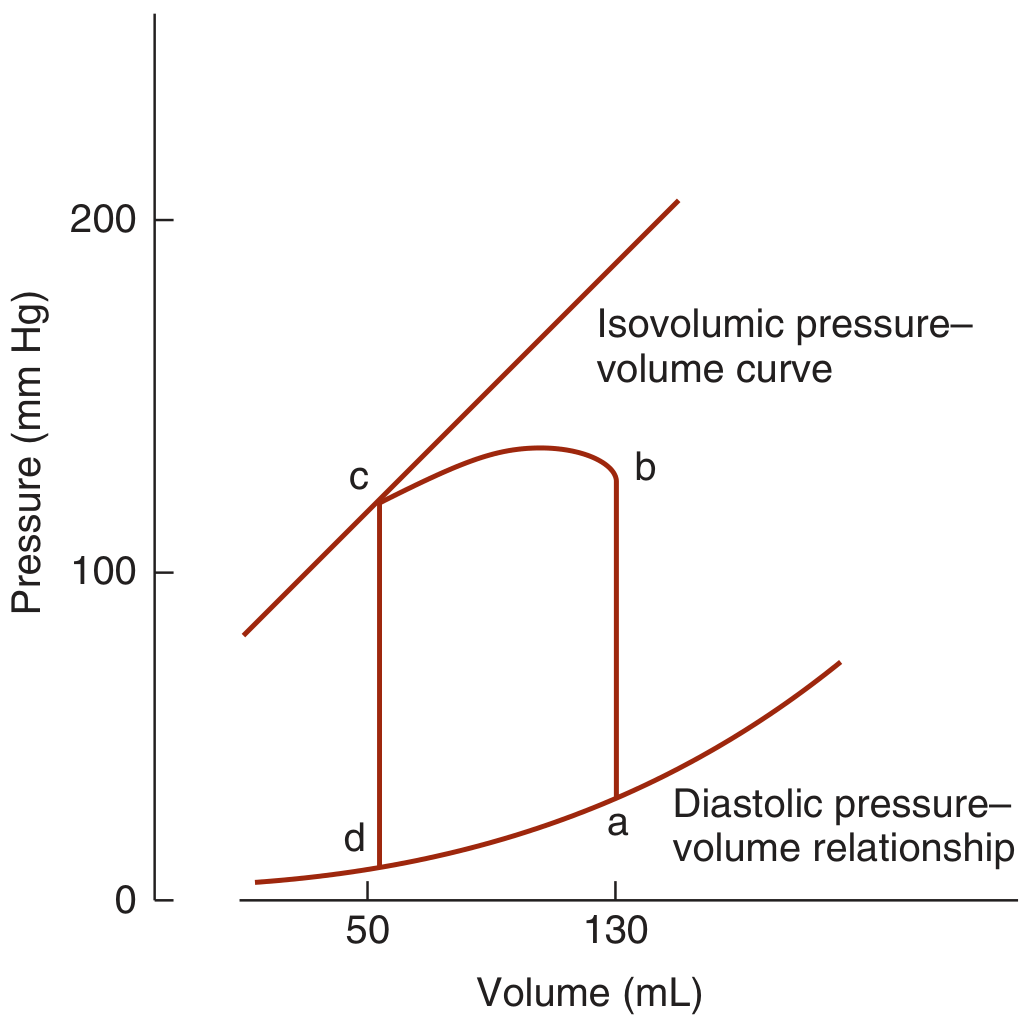
The P-V loop traces the entire cardiac cycle:
- d → a: Diastolic filling (volume increases ~50 to ~130 mL at low pressure)
- a → b: Isovolumetric contraction (pressure rises steeply, volume unchanged)
- b → c: Ventricular ejection (volume falls as blood enters aorta)
- c → d: Isovolumetric relaxation (pressure falls, volume unchanged)
The width of the loop = stroke volume. The area of the loop = stroke work.
- Ganong's Review of Medical Physiology, 26th Edition, p. 540
Key Numbers to Remember
| Parameter | Value |
|---|---|
| Cycle duration (HR 72 bpm) | ~0.833 s |
| Systole duration | ~0.3 s |
| Diastole duration | ~0.5 s |
| End-diastolic volume (EDV) | ~130 mL |
| End-systolic volume (ESV) | ~50 mL |
| Stroke volume | ~80 mL |
| Ejection fraction | ~65% |
| Peak LV pressure | ~120 mmHg |
| Peak RV pressure | ~25 mmHg |
| IVC duration | ~0.05 s |
| IVR duration | ~0.05-0.08 s |
Effect of Heart Rate
As heart rate increases, cycle duration decreases. Diastole is disproportionately shortened more than systole. At very high heart rates, diastasis is eliminated first, then rapid filling is compressed. This reduces ventricular filling time and end-diastolic volume, limiting stroke volume - a critical limitation of tachycardia. At normal HR 72 bpm, systole = 40% of cycle; at 3x HR, systole = 65% of cycle. - Guyton and Hall Textbook of Medical Physiology
Jugular Venous Pulse (JVP) Waveforms
The CVP/JVP waveform reflects events in the cardiac cycle:
- a wave: Atrial contraction (Phase A)
- c wave: Tricuspid valve bulging into atrium during isovolumetric contraction (Phase B)
- x descent: Atrial relaxation + AV valve pulled downward during ventricular ejection
- v wave: Passive atrial filling while tricuspid valve is closed (Phases B-E)
- y descent: AV valve opens, blood drains from atrium to ventricle (Phase F)
- Miller's Anesthesia 10th Edition
WBC count and function
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have excellent material with real microscopy images and detailed function data. Let me compile the comprehensive answer:
White Blood Cell (WBC) Count and Function
White blood cells (WBCs), also called leukocytes, are nucleated cells that circulate in blood and form the cellular basis of the immune system. Unlike red blood cells, they are true cells with nuclei and organelles, and they carry out their primary functions largely in the tissues - the bloodstream is mainly their transport route.
Normal WBC Count (Reference Range)
| Parameter | Normal Value |
|---|---|
| Total WBC count | 4,000 - 11,000 cells/μL (4-11 × 10⁹/L) |
| More conservative lab range | ~4,000-7,000/μL |
| Leukocytosis (elevated) | >10,000-11,000/μL |
| Leukopenia (low) | <4,000/μL |
Important note: Absolute counts (not percentages) are what matter clinically - a relative increase in one cell type may simply reflect a decrease in another. - Henry's Clinical Diagnosis and Management by Laboratory Methods
Classification of WBCs
WBCs are divided into two major groups based on the presence or absence of visible cytoplasmic granules:
Hematopoietic Lineage
All WBCs arise from a pluripotent hematopoietic stem cell (HSC) in the bone marrow, which gives rise to:
- Common Myeloid Progenitor (CMP) → granulocytes (neutrophils, eosinophils, basophils) and monocytes
- Common Lymphoid Progenitor (CLP) → T cells, B cells (and plasma cells)
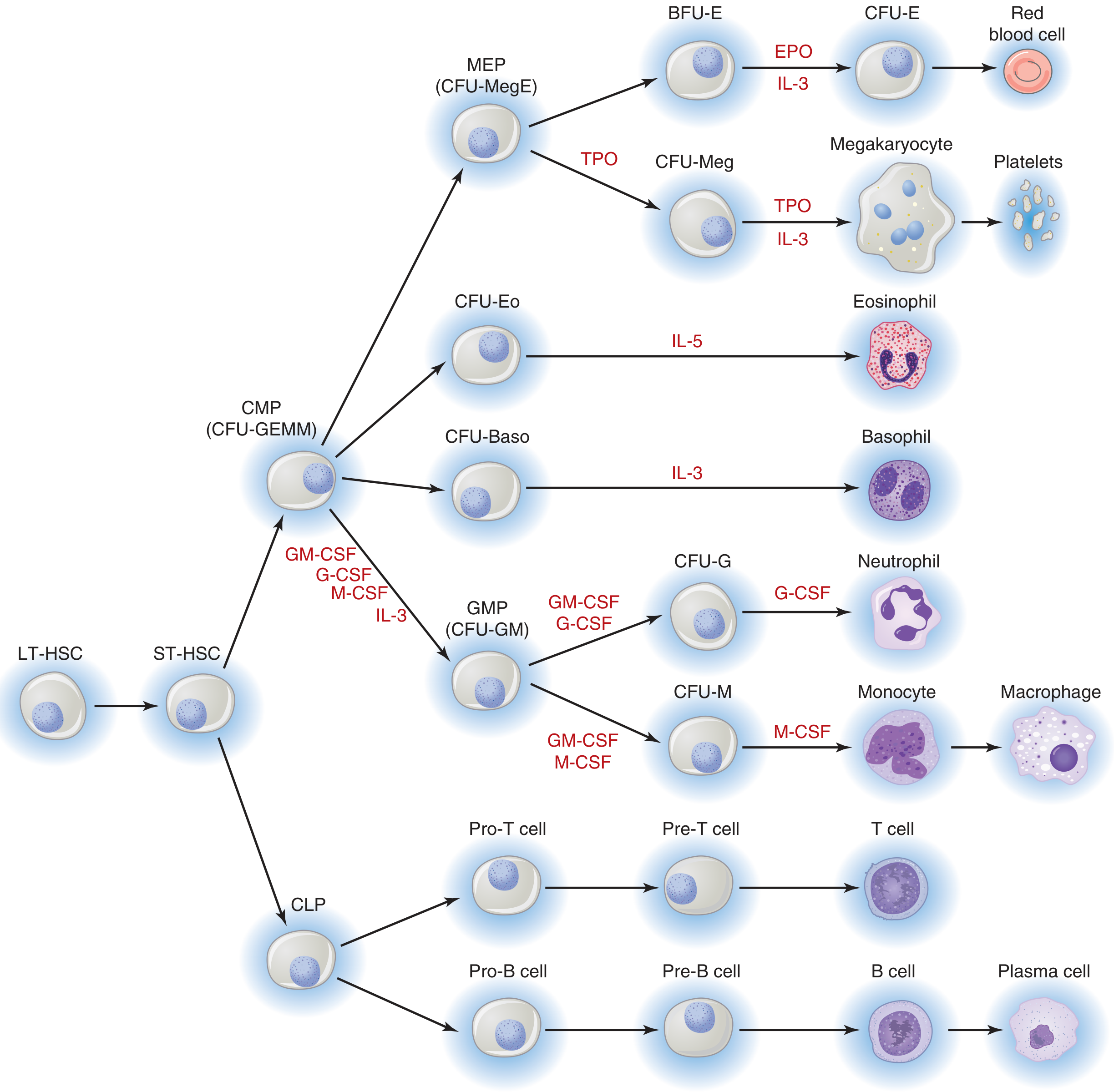
- Medical Physiology (Boron & Boulpaep)
Differential Count and Functions
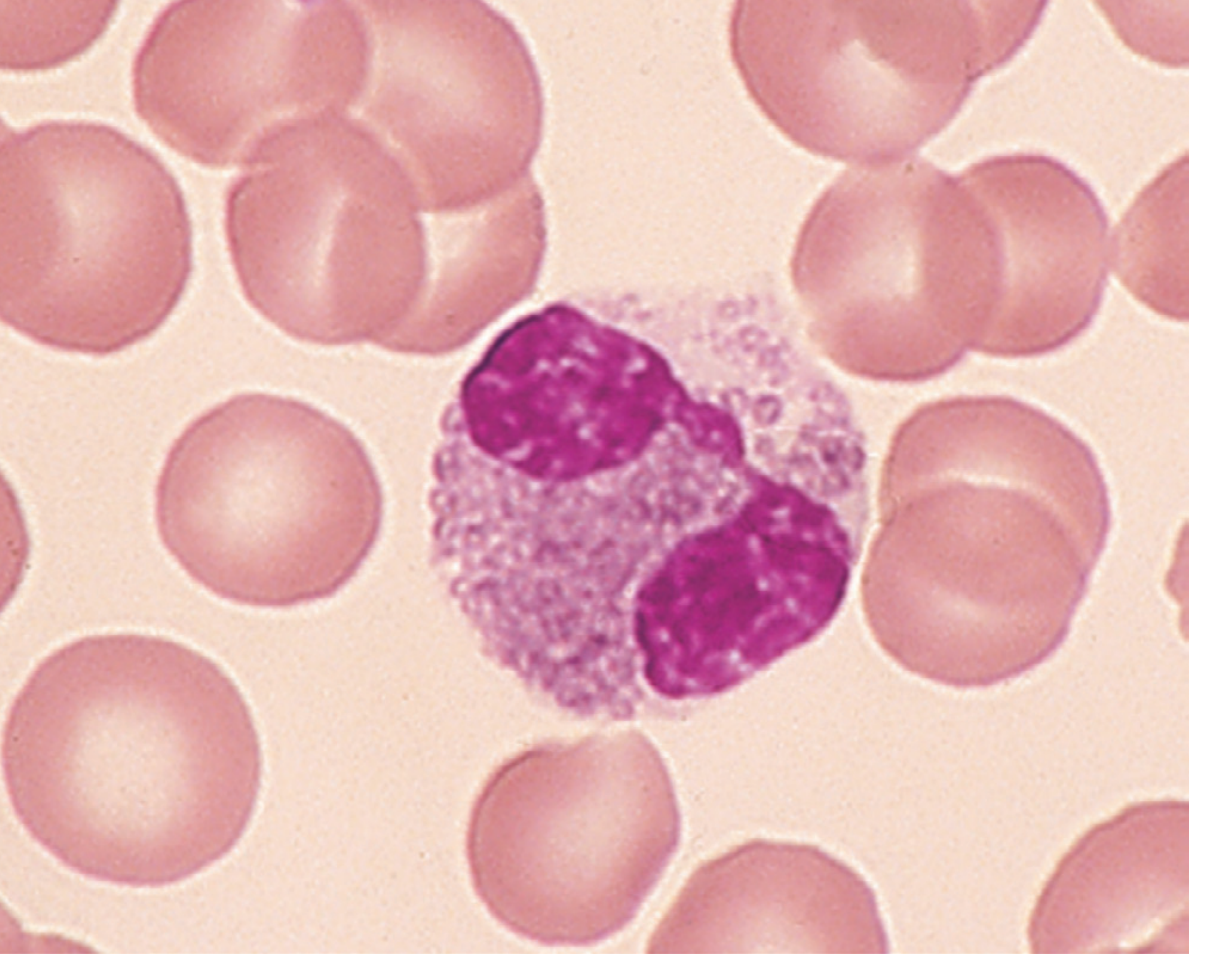
1. Neutrophils ("Polys" / PMNs)
Normal %: 50-70% of total WBCs | Absolute count: 1,800-7,700/μL
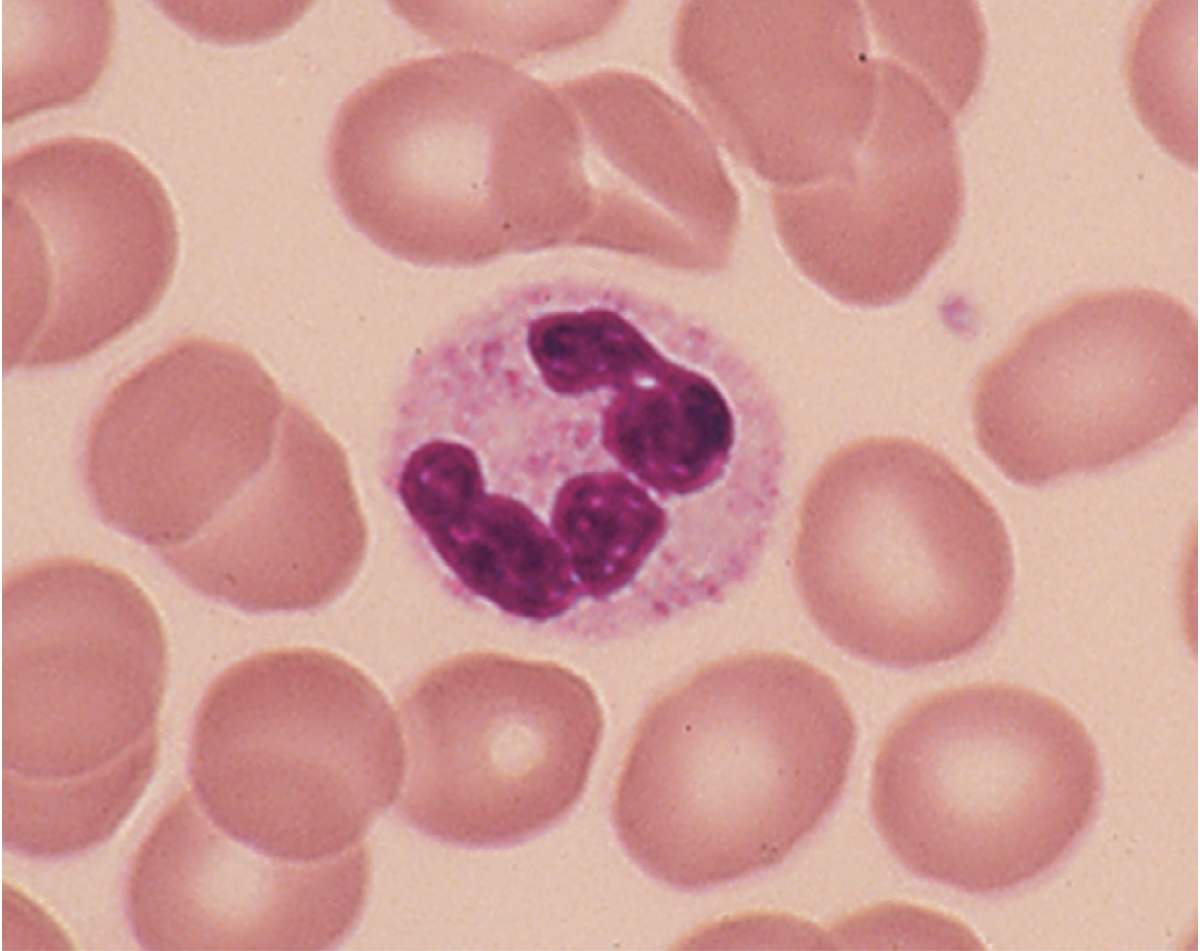
Morphology:
- Multilobed nucleus (3-5 lobes, hence "polymorphonuclear" or PMN)
- Fine, lilac-colored specific granules + azurophilic (primary) granules
- Diameter ~12-15 μm
Functions:
- The primary phagocytes of acute bacterial and fungal infection
- Key steps: Chemotaxis (migration to site of infection) → Adherence/margination (rolling and firm adhesion to endothelium via selectins and integrins) → Diapedesis (crossing endothelium) → Phagocytosis → Killing via:
- Oxidative burst (respiratory burst) - NADPH oxidase → superoxide → H₂O₂ → hypochlorous acid (HOCl via myeloperoxidase)
- Non-oxidative killing - defensins, elastase, cathepsin G (from granules)
- Circulating half-life: ~6-8 hours; survive only hours in tissues
- Band forms (immature neutrophils) in blood = "left shift" = sign of active infection/inflammation
Clinical significance of neutropenia:
- ANC <1000/μL → increased infection susceptibility
- ANC <500/μL → impaired control of endogenous flora (mouth, gut)
- ANC <200/μL → local inflammatory process is absent - Harrison's Principles of Internal Medicine 22E
Causes of neutrophilia:
- Bacterial/fungal infection, inflammation (tissue necrosis, MI), glucocorticoids, epinephrine release (exercise, stress), G-CSF therapy, myeloproliferative disease, cigarette smoking
- Leukemoid reaction: WBC ≥30,000-50,000/μL from reactive (non-leukemic) cause
Exceptions - infections causing lymphocytosis (NOT neutrophilia):
- Tuberculosis, brucellosis, pertussis, infectious mononucleosis (EBV), viral infections
2. Lymphocytes
Normal %: 20-40% | Absolute count: 1,000-4,800/μL
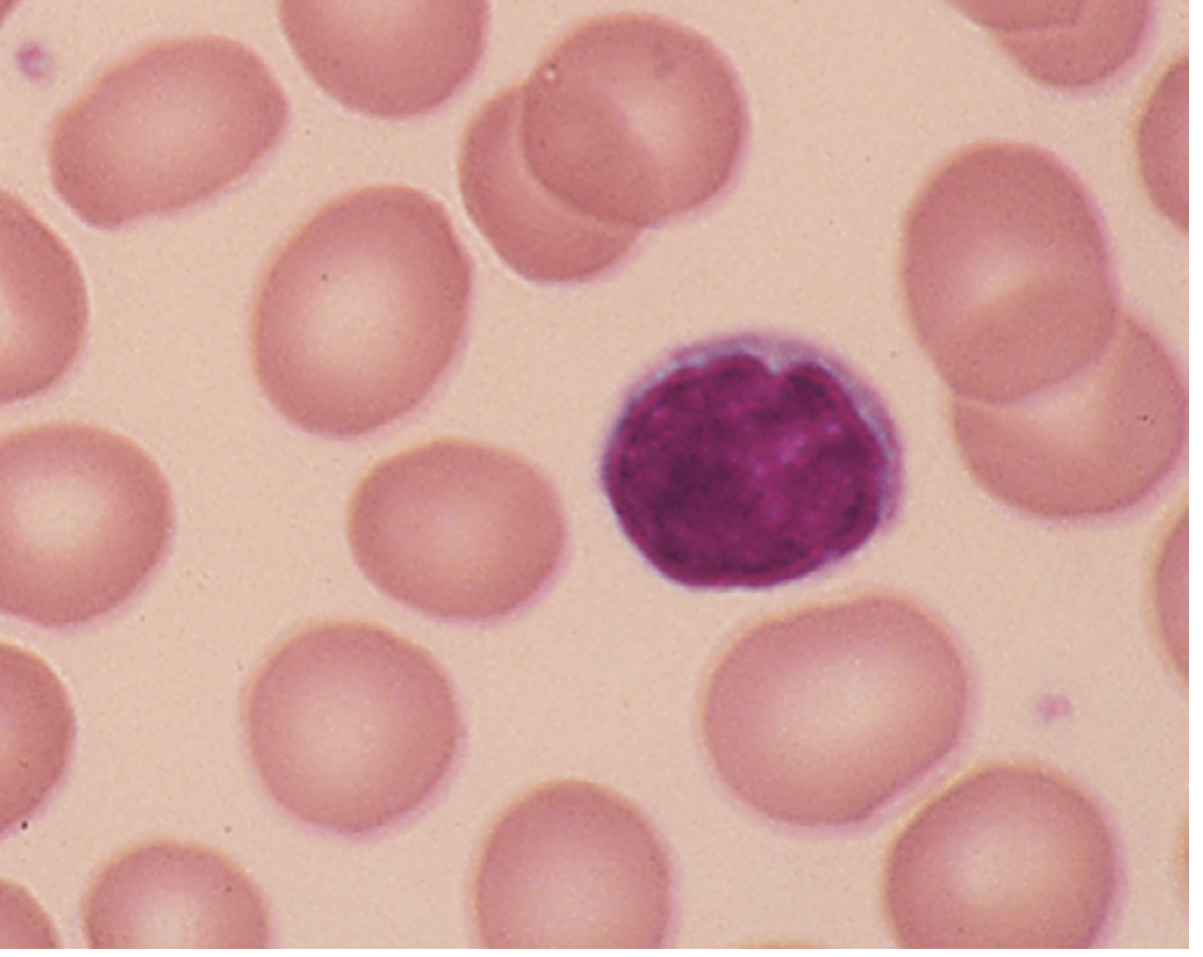
Morphology:
- Smallest WBC (~8-10 μm)
- Dense, round, deep purple nucleus
- Thin rim of pale cytoplasm (scant)
Types and functions:
| Type | Marker | Function |
|---|---|---|
| T lymphocytes | CD3+ | Cell-mediated immunity; T helper (CD4+) coordinate immune response; T cytotoxic (CD8+) kill virus-infected and tumor cells; T regulatory (Treg) suppress excessive immune responses |
| B lymphocytes | CD19/CD20+ | Humoral immunity; differentiate into plasma cells that produce antibodies (IgM, IgG, IgA, IgE, IgD) |
| NK cells | CD16/CD56+ | Natural killer cells; kill virus-infected and tumor cells without prior sensitization |
Lymphocytosis causes: Viral infections (EBV/mono, CMV, hepatitis, HIV), pertussis, TB, chronic infections, lymphoproliferative malignancies (CLL, lymphoma)
3. Monocytes
Normal %: 2-8% | Absolute count: 200-800/μL
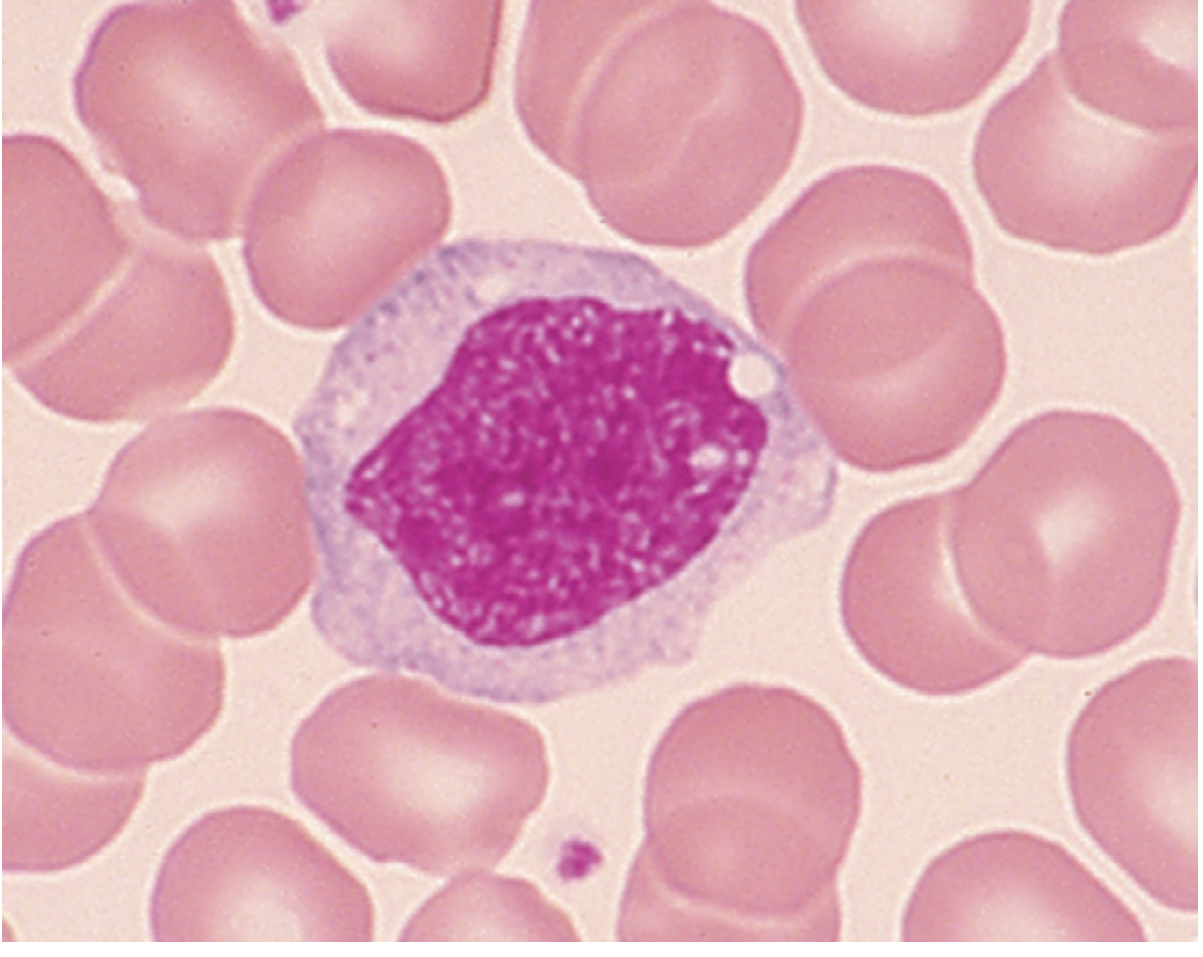
Morphology:
- Largest WBC (~15-20 μm)
- Kidney-shaped, horse-shoe or folded nucleus (not segmented)
- Abundant pale, gray-blue cytoplasm; vacuoles may be present
Functions:
- Circulate in blood for ~1-3 days, then enter tissues and differentiate into macrophages (liver - Kupffer cells; lung - alveolar macrophages; CNS - microglia; spleen - splenic macrophages; bone - osteoclasts)
- Phagocytosis and killing of bacteria, fungi, parasites
- Antigen presentation to T cells via MHC class II molecules
- Cytokine production (IL-1, IL-6, TNF-α) orchestrating inflammation
- Scavenging of dead cells and cellular debris
Monocytosis causes: TB, rickettsia, listeria, inflammatory bowel disease, acute monocytic leukemia (M5-AML), chronic myelomonocytic leukemia (CMML)
4. Eosinophils
Normal %: 1-4% | Absolute count: 100-400/μL
Morphology:
- Bilobed nucleus (2 lobes)
- Packed with large, bright orange-red (eosinophilic) granules - the most distinctive feature
- Contains major basic protein (MBP), eosinophil cationic protein (ECP), eosinophil peroxidase
Functions:
- Defense against parasitic infections (helminths/worms) - release toxic granule contents (MBP, ECP) extracellularly to kill parasites too large to phagocytose
- Modulates allergic/hypersensitivity reactions (via IgE and mast cell interactions)
- Recruited to allergic inflammatory sites (asthma, rhinitis, atopic dermatitis)
Eosinophilia causes: Allergic diseases (asthma, atopic dermatitis, allergic rhinitis), parasitic infections, drug reactions, hypereosinophilic syndrome, hematologic malignancies (CML, lymphoma)
5. Basophils
Normal %: 0-1% | Absolute count: 0-100/μL (rarest WBC)
Morphology:
- Bilobed/irregular nucleus (often obscured by granules)
- Large, dark blue-purple (basophilic) granules that may overlie the nucleus
- The granules contain heparin and histamine
Functions:
- IgE-mediated allergic responses - IgE binds to FcεRI receptors on basophil surface; antigen cross-linking triggers degranulation → release of:
- Histamine → vasodilation, bronchoconstriction, itch
- Heparin → anticoagulation at sites of inflammation
- Leukotrienes (LTC₄) → sustained bronchoconstriction
- The blood counterpart of mast cells (which reside in tissues)
Basophilia causes: CML (basophilia is a key feature; >1% basophils is suggestive), other myeloproliferative diseases, some inflammatory/allergic states
Differential Count Summary Table
| Cell | % of WBC | Absolute Count (/μL) | Key Feature | Main Function |
|---|---|---|---|---|
| Neutrophil | 50-70% | 1,800-7,700 | Multilobed nucleus (3-5 lobes) | Bacterial/fungal phagocytosis |
| Lymphocyte | 20-40% | 1,000-4,800 | Small, dense round nucleus | Adaptive immunity (T & B cells) |
| Monocyte | 2-8% | 200-800 | Largest WBC; kidney-shaped nucleus | Phagocytosis → tissue macrophages |
| Eosinophil | 1-4% | 100-400 | Bilobed; bright orange granules | Anti-parasitic; allergic response |
| Basophil | 0-1% | 0-100 | Large dark blue granules | Allergic response (histamine/heparin) |
Memory aid: "Never Let Monkeys Eat Bananas" = Neutrophils, Lymphocytes, Monocytes, Eosinophils, Basophils (order by abundance)
Abnormal WBC Counts: Clinical Correlations
| Abnormality | Definition | Common Causes |
|---|---|---|
| Leukocytosis | WBC >11,000/μL | Infection, inflammation, stress, steroids, leukemia |
| Leukopenia | WBC <4,000/μL | Viral infections, chemotherapy, aplastic anemia, SLE |
| Neutrophilia | Neutrophils >7,700/μL | Bacterial infection, trauma, steroids, MI |
| Neutropenia | Neutrophils <1,800/μL | Chemotherapy, viral infections, autoimmune, drugs |
| Lymphocytosis | Lymphocytes >4,800/μL | Viral infections (EBV, CMV), CLL, pertussis |
| Eosinophilia | Eosinophils >400/μL | Parasites, allergy, asthma, drugs (DRESS) |
| Basophilia | Basophils >100/μL | CML, myeloproliferative diseases |
| Monocytosis | Monocytes >800/μL | TB, CMML, M4/M5 AML, inflammatory conditions |
| Leukemoid reaction | WBC ≥30,000-50,000/μL | Reactive (non-clonal); mimics leukemia on smear |
- Henry's Clinical Diagnosis and Management by Laboratory Methods; Harrison's Principles of Internal Medicine 22E
Key Functional Concepts
Neutrophil Steps in Acute Inflammation
- Margination - neutrophils move to vessel wall periphery
- Rolling - loose attachment via P-selectin/E-selectin on endothelium and L-selectin on neutrophil
- Firm adhesion - ICAM-1 (endothelium) with LFA-1/Mac-1 integrins (neutrophil); upregulated by IL-1, TNF-α
- Diapedesis - migration through endothelial junctions into tissue
- Chemotaxis - directed migration along chemotactic gradient (C5a, LTB4, IL-8/CXCL8, bacterial fMLP)
- Phagocytosis - engulfment enhanced by opsonins (IgG, C3b)
- Killing - oxidative burst + granule discharge
Lymphocyte Immune Functions
- T helper (CD4+): Activate macrophages (via IFN-γ), help B cells make antibodies (via IL-4/IL-5/IL-6), coordinate entire adaptive response
- T cytotoxic (CD8+): Kill virus-infected cells and tumor cells by perforin/granzyme pathway and Fas-FasL
- B cells/Plasma cells: Produce antibodies; class switch from IgM → IgG/IgA/IgE depending on cytokine signals
- Memory cells from both T and B lineages ensure faster, stronger responses to repeat exposures
The Monocyte-Macrophage System
Monocytes (blood) → Macrophages (tissues). Macrophages are the dominant cell for:
- Phagocytosis of dead cells (efferocytosis)
- Killing of intracellular pathogens (mycobacteria, fungi)
- Antigen presentation to CD4+ T cells
- Granuloma formation in chronic inflammation
Sources: Harrison's Principles of Internal Medicine 22E; Henry's Clinical Diagnosis and Management by Laboratory Methods; Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.