Ecmo
Reading File
Finding Sources
Searching PubMed
"extracorporeal membrane oxygenation" ECMO
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive overview of ECMO based on authoritative medical textbooks.
Extracorporeal Membrane Oxygenation (ECMO)
What Is ECMO?
ECMO (also called extracorporeal life support, ECLS) is a form of prolonged cardiopulmonary bypass that provides temporary support to the heart and/or lungs in patients with severe, refractory failure. The concept traces back to Gibbon's cardiopulmonary bypass circuit, first used successfully in 1953. The first successful use for trauma-induced ARDS was reported in 1972.
Basic Circuit Components
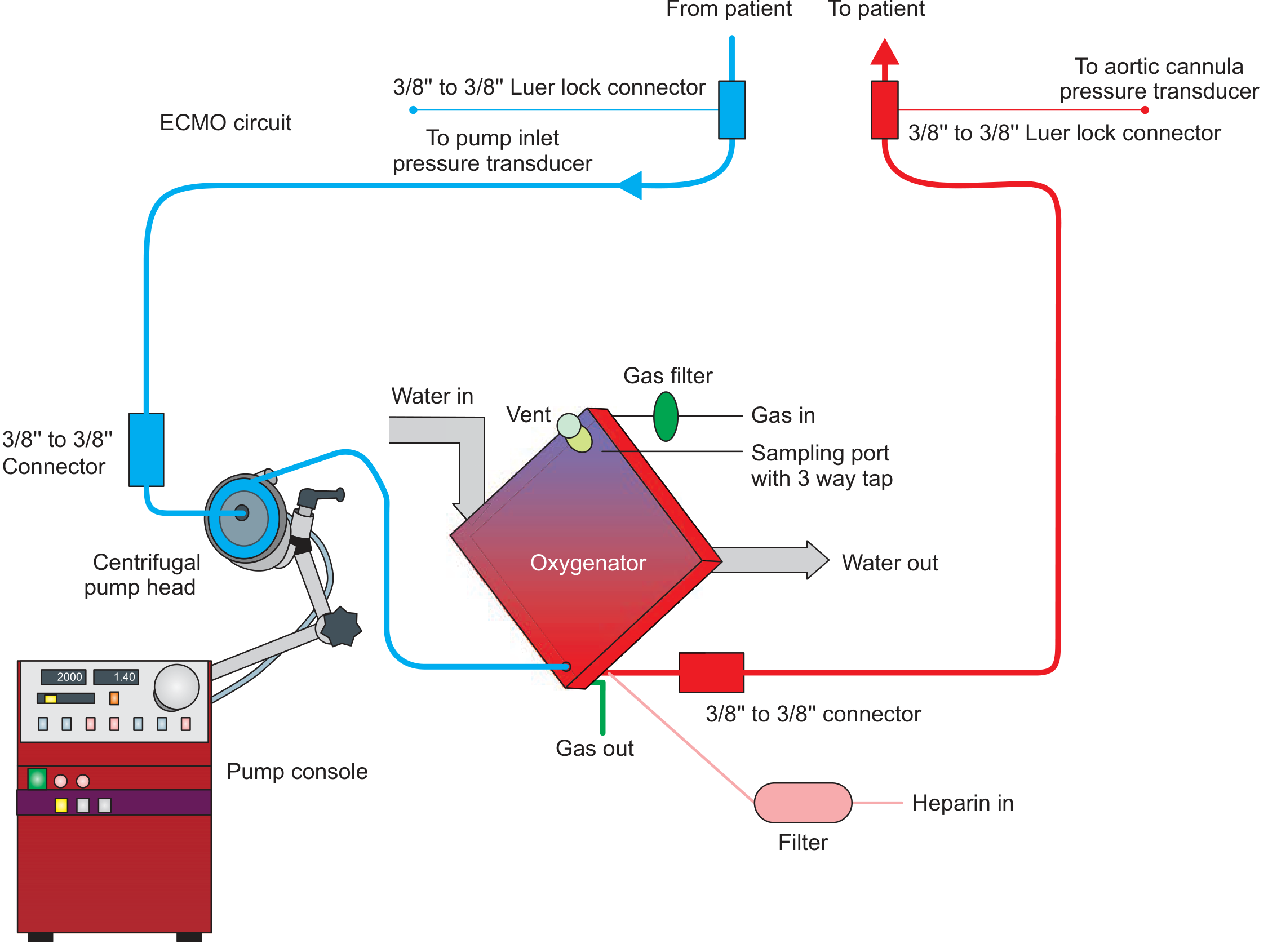
Figure: Basic ECMO circuit - Fishman's Pulmonary Diseases and Disorders, p. 2641
An ECMO circuit consists of four main components:
- Inflow (drainage) cannula - drains venous blood from the patient
- Centrifugal pump - magnetically levitated disc that creates a vortex; preload-dependent and afterload-sensitive
- Membrane oxygenator - thousands of hollow-bore microtubules through which oxygen flows; blood oxygenation occurs across a 2 m² surface (vs. 91-118 m² in the human lung)
- Outflow (return) cannula - returns oxygenated blood to the patient
The oxygenator also includes a heat exchanger to compensate for heat loss as blood crosses the membrane.
Types of ECMO
VV ECMO (Veno-Venous)
- Drains blood from a vein and returns it to a vein (typically femoral/internal jugular)
- Provides pulmonary support only - no hemodynamic support
- Primary modality for isolated ARDS and acute respiratory failure
- Requires adequate native cardiac function
VA ECMO (Veno-Arterial)
- Drains venous blood and returns oxygenated blood into the arterial system (usually femoral artery)
- Provides both cardiac and pulmonary support
- Indicated for cardiogenic shock, cardiac arrest, biventricular failure, myocarditis, myocardial stunning
- Can cause left ventricular fluid overload and pulmonary edema because it does not unload the LV - often requires additional LV venting strategies (inotropes, IABP, Impella)
VAV ECMO (Veno-Arterio-Venous)
- Hybrid configuration used when ARF is accompanied by biventricular failure
RVAD-ECMO (Protek Duo)
- Cannula traverses the tricuspid and pulmonic valves; drains from SVC/right atrium and returns blood to the pulmonary artery
- Used for isolated RV failure with ARDS - provides both RV support and oxygenation
Indications
| Category | Examples |
|---|---|
| Pulmonary (VV ECMO) | Severe ARDS, refractory hypoxemia (PaO2/FiO2 <80 despite optimal vent settings), bridge to lung transplant |
| Cardiac (VA ECMO) | Cardiogenic shock, post-cardiotomy failure, myocarditis, massive PE, cardiac arrest (ECPR) |
| Combined | ARDS with cor pulmonale, sepsis-induced cardiomyopathy with ARDS (occurs in 15-20% of patients) |
| Bridge | Bridge to recovery, bridge to VAD, bridge to transplant |
Criteria for VA ECMO support are still being established and are highly institution-dependent.
ECMO Gas Exchange Physiology
- The oxygenator is very efficient at CO2 removal - complete CO2 removal can be achieved with high sweep gas flows at blood flow rates <1 L/min
- Oxygenation requires higher flows - approximately 4 L/min must be maintained to achieve adequate O2 delivery (~260 mL O2/min), with post-oxygenator PaO2 >300 mmHg
- Pre- and post-membrane pressure sensors monitor oxygenator function; a normal transmembrane pressure drop should not exceed 30 mmHg
Anticoagulation
Anticoagulation is required throughout ECMO to prevent circuit thrombosis:
| Agent | Notes |
|---|---|
| Unfractionated heparin (UFH) | Most common; easy to monitor (aPTT, ACT); reversible; risk of HIT and variable anticoagulant effect |
| Bivalirudin | Direct thrombin inhibitor; lower HIT risk; independent of antithrombin III; half-life ~25 min; no FDA-approved reversal agent |
| Argatroban | Direct thrombin inhibitor; hepatically cleared; half-life ~45-50 min |
A retrospective study of VV ECMO patients found bivalirudin resulted in decreased circuit thrombosis, decreased transfusion requirements, and significantly fewer major bleeding events (11.7% vs. 40.7% for heparin).
Complications
Bleeding
- Most common complication - caused by anticoagulation, thrombocytopenia, mechanical platelet destruction, loss of clotting factors
- Common sites: epistaxis, GI bleeding
- Rare but severe: intracranial hemorrhage, pulmonary hemorrhage
Thrombotic
- Activation of neutrophils, monocytes, leukocytes in the circuit
- Risk of clot formation in the circuit (oxygenator thrombosis)
- Occasional cytokine storm
Vascular
- Arterial injury, pneumothorax during cannulation
- Mitigated by ultrasound-guided access, TEE guidance, echocardiography
LV-specific (VA ECMO)
- Pulmonary edema and LV fluid overload - because VA ECMO increases afterload on an already impaired LV without providing direct LV unloading
Cannulation and Monitoring
- Ultrasound guidance is mandatory for percutaneous vascular access
- Transesophageal echocardiography (TEE) should be performed before and during cannulation to:
- Assess RV and LV function
- Rule out patent foramen ovale, ASD, VSD (which would cause recirculation)
- Detect pericardial effusion
- Guide cannula tip positioning
- Fluoroscopy is also used, especially for PA cannulas (Protek Duo)
- Transmembrane pressure monitoring and flow monitoring are standard of care
Weaning and Discontinuation
ECMO is used as a bridge to one of three outcomes:
- Bridge to recovery - days to weeks; device removed when native cardiac/pulmonary function recovers
- Bridge to durable device - transition to LVAD or BiVAD
- Bridge to transplant - heart or lung transplant
Note: ECMO is not a sustainable long-term device due to infection risk and ongoing complications. VA ECMO and IABP are acute devices that are replaced by VADs when durable support is needed.
Recent Evidence (2024-2026)
A 2026 systematic review and meta-analysis (PMID 40920225) examined ECMO cannulation by intensivists, relevant to expanding operator scope in high-acuity settings.
A 2024 Lancet individual patient data meta-analysis (PMID 39236726) on temporary mechanical circulatory support in infarct-related cardiogenic shock provides updated guidance on device selection including ECMO vs. other support options.
Sources: Fishman's Pulmonary Diseases and Disorders, Chapter 149 (pp. 2641-2703); Fischer's Mastery of Surgery, 8th ed. (pp. 345-346)
This is a shared conversation. Sign in to Orris to start your own chat.