Atazolisumab cancer treatment injection??
Reading File
Finding Sources
Searching PubMed
atezolizumab cancer immunotherapy
Searching the Web
atezolizumab Tecentriq cancer treatment 2025 indications mechanism
Reading File
Reading File
Here is a thorough overview of Atezolizumab (Tecentriq) - I believe that's the drug you are asking about (there is no drug called "Atazolisumab"):
Atezolizumab (Tecentriq)
What it is
Atezolizumab (brand name Tecentriq) is a humanized IgG1 monoclonal antibody that targets PD-L1 (Programmed Death-Ligand 1). It belongs to the class of drugs called immune checkpoint inhibitors. It was first FDA-approved in 2016.
- Goodman & Gilman's Pharmacological Basis of Therapeutics
Mechanism of Action
Cancer cells "hide" from the immune system by expressing PD-L1 on their surface. PD-L1 binds to the PD-1 receptor on T-cells, sending a "don't attack me" signal that shuts down T-cell activity.
Atezolizumab blocks PD-L1, preventing it from binding to PD-1. This releases the brakes on T-cells, allowing them to recognize and destroy cancer cells.
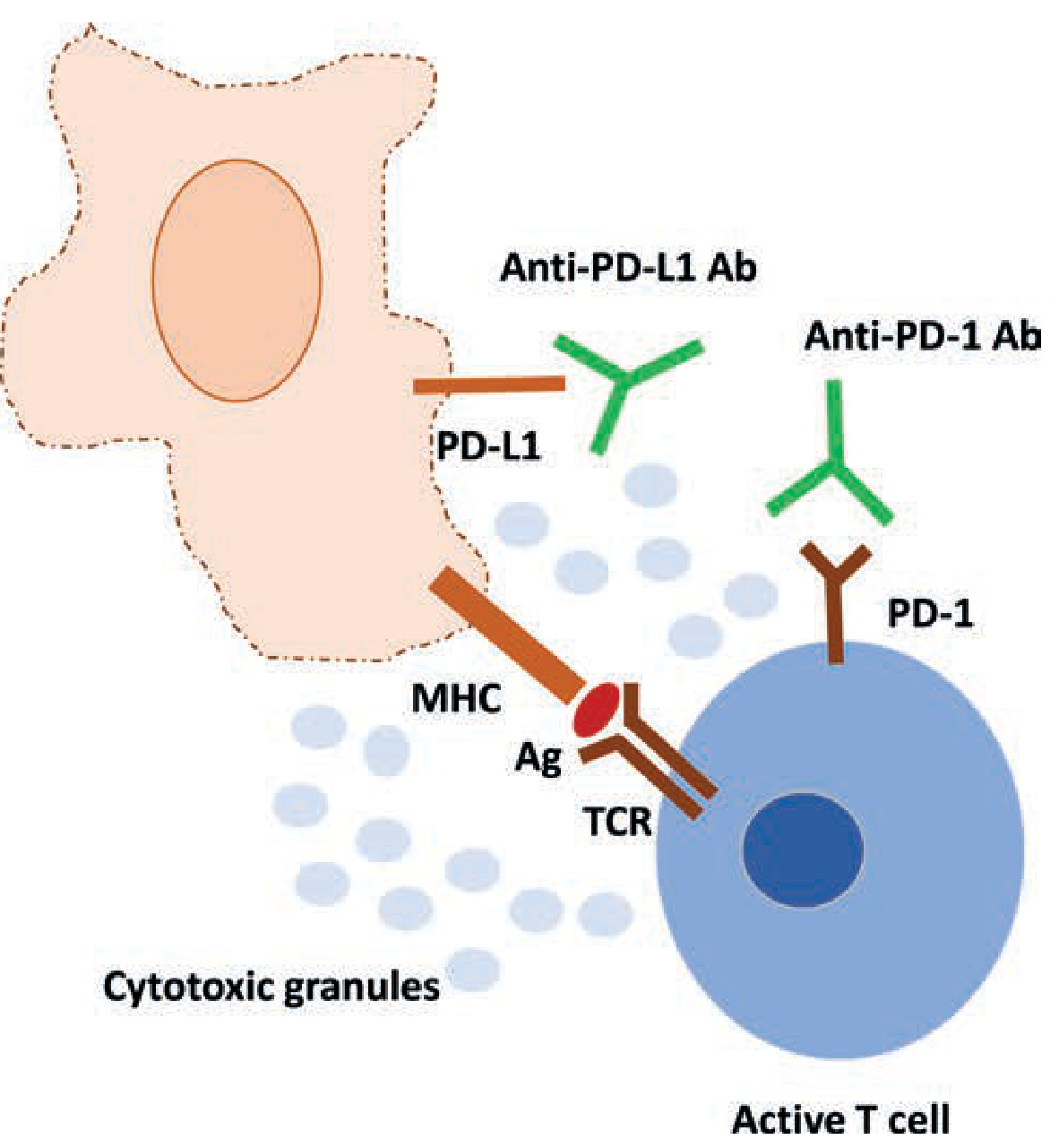
Active T-cell restored to kill tumor cells once PD-L1 is blocked - Fishman's Pulmonary Diseases
How it is Given
-
Intravenous (IV) infusion - administered over 60 minutes, every 3 weeks
-
There is also a newer formulation: Tecentriq Hybreza (atezolizumab + hyaluronidase-tqjs) which can be given subcutaneously (under the skin)
-
Half-life: approximately 27 days
-
Goodman & Gilman's, p.1443
Approved Cancer Indications
| Cancer Type | Setting | Notes |
|---|---|---|
| Non-small cell lung cancer (NSCLC) | 1st line, 2nd line, adjuvant | Requires PD-L1 testing for some indications; no EGFR/ALK mutations |
| Extensive-stage small cell lung cancer (ES-SCLC) | 1st line + carboplatin/etoposide | First regimen in 30 years to improve SCLC survival |
| Urothelial carcinoma (bladder cancer) | Metastatic | PD-L1 expression required for some settings |
| Triple-negative breast cancer (TNBC) | 1st line + paclitaxel | |
| Hepatocellular carcinoma (HCC) | 1st line + bevacizumab | Unresectable or metastatic |
| Melanoma | BRAF V600 mutation-positive | With cobimetinib + vemurafenib |
| Cervical cancer adenocarcinoma | Selected settings | Added 2025 |
- Goodman & Gilman's; Genentech prescribing information (2025)
Key Side Effects
Common (≥20% of patients):
- Fatigue
- Decreased appetite
- Shortness of breath (dyspnea)
- Cough
- Nausea
- Musculoskeletal pain
- Constipation
Immune-related adverse effects (irAEs) - because it activates the immune system, it can cause autoimmune-like reactions:
- Hepatitis (liver inflammation)
- Colitis (gut inflammation)
- Thyroid disorders (hypothyroidism/hyperthyroidism)
- Adrenal insufficiency
- Hypophysitis (pituitary inflammation)
- Rare but serious: type 1 diabetes, pancreatitis, myasthenia gravis, Guillain-Barre syndrome, eye inflammation
Important: Patients with myasthenia gravis should avoid or use this drug with extreme caution as it can trigger severe flares.
Pregnancy: Can cause embryo-fetal harm - women of childbearing potential must be warned.
- Goodman & Gilman's, p.1443; Bradley & Daroff's Neurology
Recent Evidence (2024-2025)
Recent systematic reviews confirm atezolizumab's efficacy in:
- NSCLC (squamous and non-squamous): Network meta-analysis supports its role in advanced squamous NSCLC (PMID 41035637)
- HCC: Atezolizumab + bevacizumab remains a top regimen for unresectable HCC based on quality of life and survival data (PMID 40810932)
- Triple-negative breast cancer: Confirmed role in metastatic TNBC (PMID 39742383)
Important Notes
- PD-L1 testing is required before using atezolizumab for certain indications - not all patients qualify.
- It is not used in cancers with EGFR mutations or ALK rearrangements in NSCLC (targeted therapy is preferred there).
- Immune-related side effects can appear weeks to months after starting treatment and may require steroids or stopping the drug.
Disclaimer: This information is for educational purposes only. Atezolizumab must be prescribed and monitored by a qualified oncologist. Dosing, eligibility, and management of side effects require specialist oversight.
Is it used in adenocarcinoma of stomach
Finding Sources
Finding Sources
Searching PubMed
atezolizumab gastric adenocarcinoma
Searching the Web
atezolizumab gastric stomach adenocarcinoma FDA approval 2025
Reading Article
PMID: 37963317
Reading Article
PMID: 40244574
Finding Sources
Here is a clear, evidence-based answer:
Atezolizumab in Gastric Adenocarcinoma
Short Answer: Not FDA-approved for gastric cancer, but actively studied in clinical trials
As of May 2026, atezolizumab does not have an FDA-approved indication specifically for gastric or gastroesophageal junction (GEJ) adenocarcinoma. The checkpoint inhibitors with approved roles in gastric cancer are nivolumab and pembrolizumab (both PD-1 inhibitors, not PD-L1 like atezolizumab).
What IS Approved for Gastric Adenocarcinoma (2025)
| Drug | Target | Indication |
|---|---|---|
| Nivolumab (Opdivo) | PD-1 | 1st-line metastatic gastric/GEJ + chemo; adjuvant post-surgery |
| Pembrolizumab (Keytruda) | PD-1 | HER2+, PD-L1 CPS ≥1 gastric/GEJ + trastuzumab + chemo (full FDA approval March 2025) |
| Durvalumab (Imfinzi) | PD-L1 | Resectable gastric/GEJ - neoadjuvant + adjuvant setting (FDA approved late 2025) |
Notably, durvalumab - another PD-L1 inhibitor like atezolizumab - received its first gastric cancer approval in late 2025, but atezolizumab has not followed suit yet.
Atezolizumab in Gastric Cancer - Clinical Trial Evidence
There are two key trials showing promising (though early) results:
1. DANTE Trial (Phase II/III) - Resectable Esophagogastric Adenocarcinoma
- Regimen: Atezolizumab + FLOT (fluorouracil, leucovorin, oxaliplatin, docetaxel) perioperatively
- Key findings: Adding atezolizumab improved tumor downstaging and pathologic complete response rates (24% vs 15%, p=0.032) compared to FLOT alone
- Best results in: PD-L1 CPS ≥10 (33% vs 12% pCR) and MSI-high tumors (63% vs 27% pCR)
- Safety: Comparable to FLOT alone
- J Clin Oncol, 2024 (PMID 37963317)
2. Phase II RCT - HER2-positive Gastric/GEJ Cancer (JAMA Oncology, 2025)
- Regimen: Atezolizumab + trastuzumab + XELOX (capecitabine + oxaliplatin) vs trastuzumab + XELOX alone
- Key finding: pCR rate significantly higher with atezolizumab added (38% vs 14%)
- Population: Locally advanced, resectable, ERBB2 (HER2)-positive gastric/GEJ cancer
- JAMA Oncol, 2025 (PMID 40244574)
3. PANDA Trial (Phase II) - Neoadjuvant Setting
- Tested atezolizumab + chemotherapy as neoadjuvant therapy in gastric and GEJ adenocarcinoma
- Published in Nature Medicine, 2024 (PMID 38191613)
Key Biomarkers That Matter
The trials suggest atezolizumab is most likely to benefit patients who are:
- MSI-high (microsatellite instability-high) - strongest response
- PD-L1 CPS ≥10 - better pathologic responses
- HER2-positive - when combined with trastuzumab
Bottom Line
| Status | Details |
|---|---|
| FDA-approved for gastric cancer? | No |
| Being studied in gastric cancer? | Yes - active Phase II/III trials |
| Promising signals? | Yes, especially in MSI-H and PD-L1-high tumors |
| Standard of care? | No - nivolumab and pembrolizumab are preferred |
So while atezolizumab is not the current standard for gastric adenocarcinoma, it is under active investigation and may gain approval in the future, particularly in the perioperative or HER2-positive settings if Phase III data matures favorably.
WES and ngs difference
Finding Sources
Finding Sources
Searching the Web
WES whole exome sequencing vs NGS next generation sequencing differences comparison
Reading File
Reading File
Excellent - I have comprehensive information. Here is a clear, structured breakdown:
NGS vs WES - The Key Distinction
The Core Relationship
NGS is the technology. WES is one application of that technology.
Think of it this way:
- NGS = the sequencing platform/method (like saying "digital photography")
- WES = one specific type of study done using NGS (like saying "portrait photography")
WES, WGS, and targeted panels are all types of NGS. You cannot have WES without NGS, but NGS encompasses far more than just WES.
What is NGS (Next Generation Sequencing)?
NGS, also called massively parallel sequencing (MPS), is a high-throughput DNA sequencing technology that replaced the older "first generation" Sanger sequencing.
How it works (3 steps):
- Library construction - DNA is fragmented into small pieces (75-400 base pairs), size-sorted, ligated to adapter sequences, and immobilized on a solid support
- Sequencing - All fragments are sequenced simultaneously in parallel (millions at once)
- Analysis - Powerful computing assembles the fragments back into a coherent sequence
Key advantages over Sanger sequencing:
-
Much faster - sequences millions of fragments at once
-
Higher sensitivity for detecting low-frequency variants
-
More cost-effective when multiple targets are needed
-
Can detect variants present in only a small fraction of cells (important in cancer)
-
Quick Compendium of Clinical Pathology, 5th ed., p.373
Types of NGS - Where WES Fits In
| NGS Type | What It Sequences | Genome Coverage | Clinical Use |
|---|---|---|---|
| Targeted Panel | Specific genes of interest (e.g., 50-500 genes) | <1% | Cancer somatic mutations, specific disease panels |
| WES (Whole Exome Sequencing) | All protein-coding regions (exons) | ~1-2% of genome (~30 Mb) | Rare genetic/Mendelian diseases, cancer |
| WGS (Whole Genome Sequencing) | Entire genome, coding + non-coding | ~100% (~3.3 Gb) | Complex cases, structural variants, research |
| RNA-seq | Transcriptome (expressed RNA) | Gene expression | Cancer subtyping, splicing variants |
| Bisulfite-seq | Methylation patterns in DNA | Epigenome | Epigenetics research |
WES (Whole Exome Sequencing) - In Detail
The exome = all the protein-coding regions (exons) of the genome.
Key facts:
- The exome is only ~1-2% of the total genome (~30 megabases vs genome's 3.3 gigabases)
- Contains approximately 20,000 genes and 180,000 exons
- Despite being only 1-2% of the genome, the exome harbors ~85% of all disease-causing mutations
- This makes it very efficient - you sequence a tiny fraction of DNA but capture most of the clinically relevant variants
How WES differs from WGS (both use NGS):
| Feature | WES | WGS |
|---|---|---|
| Region sequenced | Exons only (coding) | Entire genome |
| Genome covered | ~1-2% | ~100% |
| Data generated per sample | ~10 GB | ~90 GB |
| Typical coverage depth | 100x | 30x |
| Cost | Lower | Higher (but gap is closing) |
| Detects coding variants | Excellent | Excellent |
| Detects non-coding/regulatory variants | No | Yes |
| Detects structural variants (large rearrangements) | Limited | Better |
| Copy number variants | Limited | Better |
| Data analysis burden | Moderate | High |
- PMC comparison study; Psomagen/Geneyx technical references
Clinical Applications - When to Use What
Use Targeted NGS Panel when:
- Specific cancer mutation testing (e.g., BRCA1/2, KRAS, EGFR)
- Known disease with limited gene suspects
- Fast turnaround needed
- Highest depth of coverage needed
Use WES when:
- Diagnosing rare or undiagnosed Mendelian diseases
- Intellectual disability, developmental delay, autism spectrum disorder
- Cancer genomics (somatic mutation profiling)
- Family trios (proband + parents) for de novo mutation hunting
- First-tier test when no specific gene is suspected
Use WGS when:
-
WES has failed to find a diagnosis
-
Suspected structural rearrangement or copy number variant
-
Non-coding regulatory mutations suspected
-
Population-scale genomics research
-
Goldman-Cecil Medicine, 22nd ed., p.315
A Note on Terminology
The term "whole exome" sequencing is slightly misleading - as Goldman-Cecil points out: "neither exome sequencing nor genome sequencing is truly 'whole exome' or 'whole genome'" because no capture or sequencing method achieves 100% coverage of its target. The term is used conventionally to mean the best available approximation.
In modern clinical practice, "exome sequencing (ES)" is now preferred over "whole exome sequencing (WES)", and "genome sequencing (GS)" over "whole genome sequencing (WGS)".
Summary in One Line
NGS is the engine; WES, WGS, and targeted panels are different ways to drive it. WES focuses that engine on the ~1-2% of the genome most likely to harbor disease-causing variants, balancing cost, data volume, and diagnostic yield.
This is a shared conversation. Sign in to Orris to start your own chat.