Explain me 10 common heart diseases with explain of ecg changes
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Loading Image
I now have rich textbook content from Guyton & Hall, Goldman-Cecil, Braunwald's, Tintinalli's, Fuster & Hurst's, and Harrison's. Let me compile the comprehensive answer with ECG images.
10 Common Heart Diseases and Their ECG Changes
1. ST-Elevation Myocardial Infarction (STEMI)
Disease overview: STEMI results from complete occlusion of a coronary artery, causing full-thickness (transmural) myocardial ischemia and necrosis. The most common culprit vessels are the left anterior descending (LAD), right coronary artery (RCA), and left circumflex artery.
ECG changes:
- Hyperacute phase (minutes): Tall, peaked (hyperacute) T waves - the earliest change
- Acute phase: ST-segment elevation ≥1 mm in two or more contiguous leads in the territory of the affected artery; reciprocal ST depression in opposite leads
- Evolving phase: ST elevation begins to resolve; pathological Q waves develop (>40 ms wide, >25% depth of the following R wave)
- Chronic phase: Q waves persist; T-wave inversion
Anatomic localization by leads:
| Territory | Culprit vessel | Leads with ST elevation |
|---|---|---|
| Anterior | LAD (proximal) | V1-V4 |
| Anterolateral | LAD / LCx | V1-V6, I, aVL |
| Inferior | RCA / LCx | II, III, aVF |
| Right ventricular | RCA | V1, V3R-V4R (right-sided leads) |
| Posterior | RCA / LCx | ST depression V1-V3 (mirror) |
ECG image - Anterolateral STEMI (Rosen's Emergency Medicine):
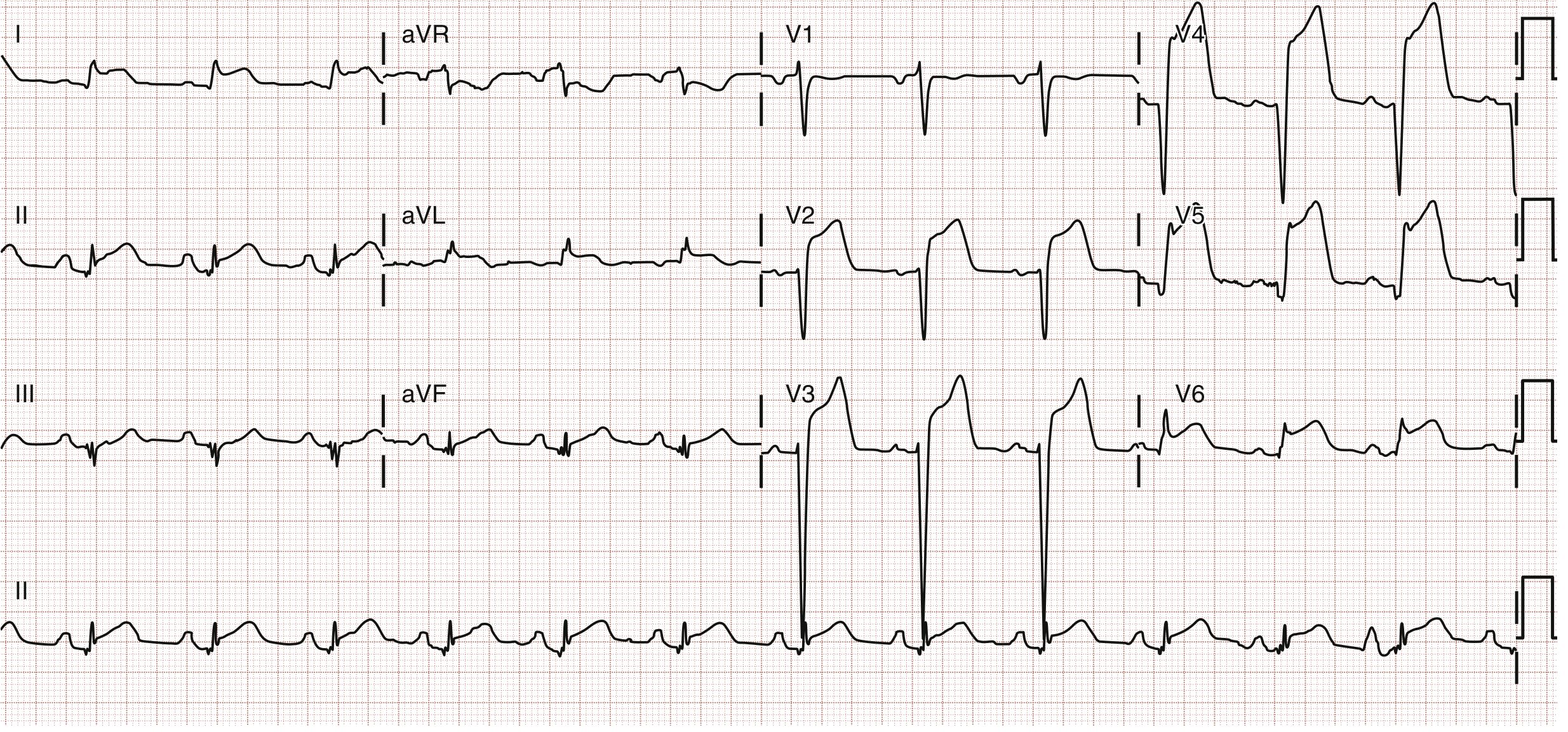
12-lead ECG: Anterolateral ST-segment elevation MI with broad ST elevation across precordial leads
ECG image - Right ventricular infarction (note: inferior STEMI + right-sided ST elevation):
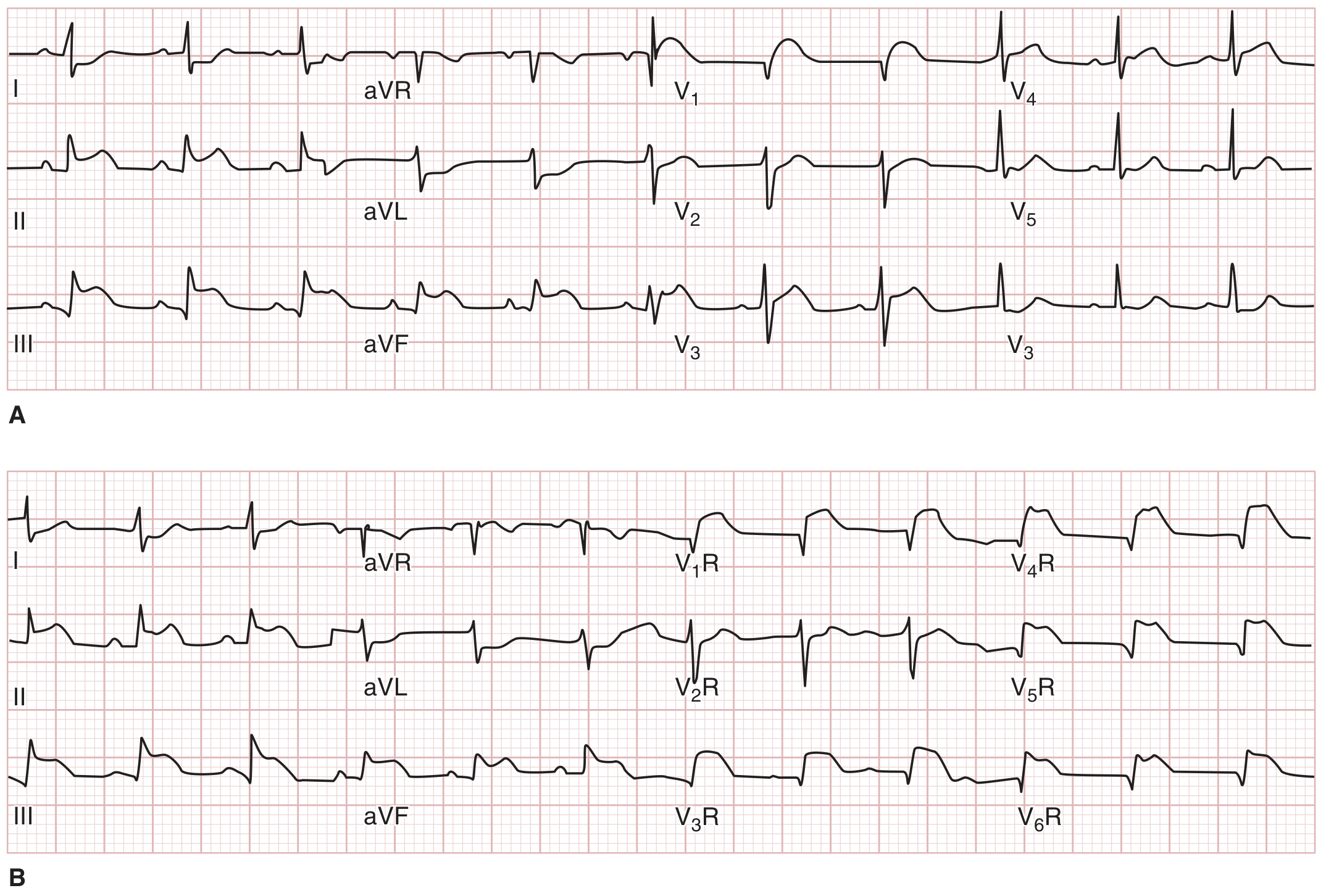
Panel A (top): Standard 12-lead showing inferior ST elevation. Panel B (bottom): Right-sided leads confirming RV infarction
- Goldman-Cecil Medicine; Rosen's Emergency Medicine; Tintinalli's Emergency Medicine
2. Non-ST-Elevation Myocardial Infarction (NSTEMI) / Unstable Angina
Disease overview: NSTEMI results from partial or transient coronary occlusion, causing subendocardial ischemia without full-thickness infarction. Biomarkers (troponin) are elevated in NSTEMI but not in unstable angina.
ECG changes:
- ST depression: Horizontal or downsloping ST depression ≥0.5 mm in two or more contiguous leads - the hallmark finding
- T-wave inversion: Deep, symmetric T-wave inversions, particularly in precordial leads (V1-V4 for anterior ischemia)
- No pathological Q waves (distinguishes from STEMI evolution)
- Transient ST elevation may occur during episodes (Prinzmetal/vasospastic angina)
- In 30-50% of cases, the ECG may be entirely normal at presentation
Key TIMI risk scoring uses ECG: ST deviation ≥0.5 mm counts as a risk point. Harrison's notes the ECG is used alongside cardiac biomarkers to risk-stratify NSTE-ACS patients.
3. Atrial Fibrillation (AF)
Disease overview: AF is the most common sustained cardiac arrhythmia. Chaotic electrical activity originates from multiple re-entrant circuits and ectopic foci, predominantly around the pulmonary vein ostia. Risk factors include hypertension, valvular disease, heart failure, thyrotoxicosis, and aging.
ECG changes:
- Absent P waves - replaced by irregular fibrillatory baseline (f-waves), best seen in V1 and lead II; "fine" fibrillation waves at 350-600/min that nearly cancel out electrically
- Irregularly irregular RR intervals - the defining hallmark; interval varies from ~0.35 to ~0.95 seconds
- Uncontrolled ventricular rate 125-150 bpm (through the AV node as a rate-limiting gatekeeper)
- Normal QRS morphology unless aberrant conduction or pre-existing bundle branch block is present

Atrial fibrillation (Lead II) - Note the complete absence of P waves; only irregularly irregular ventricular QRS and T waves are visible (Guyton & Hall Textbook of Medical Physiology)
- Guyton & Hall Textbook of Medical Physiology; Tintinalli's Emergency Medicine; Katzung's Basic and Clinical Pharmacology
4. Heart Failure (with Reduced Ejection Fraction - HFrEF)
Disease overview: Heart failure results when the heart cannot pump enough blood to meet the body's demands. HFrEF (EF <40%) is commonly caused by ischemic cardiomyopathy, hypertension, or dilated cardiomyopathy. The ECG in heart failure is non-specific but reveals structural changes.
ECG changes:
- Left ventricular hypertrophy (LVH): Tall R waves in V5-V6 (>25 mm) and deep S waves in V1-V2 (Sokolow-Lyon: SV1 + RV5 or RV6 ≥35 mm); or Cornell criteria (R in aVL ≥11 mm)
- Left bundle branch block (LBBB): Common in dilated cardiomyopathy; broad, notched QRS >120 ms with dominant R in V5-V6 and rS pattern in V1
- Left atrial enlargement: Biphasic P wave in V1, with prominent negative terminal component; broad notched P wave ("P mitrale") in lead II
- Sinus tachycardia as compensatory mechanism
- Non-specific ST-T wave changes: ST depression and T-wave inversion in lateral leads (I, aVL, V5-V6) - "strain pattern" with LVH
- Atrial fibrillation may develop secondary to left atrial enlargement
5. Hypertensive Heart Disease
Disease overview: Chronic systemic hypertension causes pressure overload on the left ventricle, leading to concentric LVH, diastolic dysfunction, and eventually systolic heart failure. It is the second most common cause of heart failure after ischemia.
ECG changes (Robbins & Kumar Basic Pathology; Tintinalli's):
- LVH pattern: The most characteristic finding; S in V1 + R in V5 ≥35 mm, or R in aVL ≥11 mm
- LV "strain" pattern: Asymmetric ST depression with T-wave inversion in leads with tall R waves (I, aVL, V5-V6); concave-upward ST depression
- Left axis deviation
- Left atrial abnormality: Broad, bifid P wave (P mitrale) in lead II
- Prolonged QRS-T angle widening
- When heart failure supervenes: LBBB, bundle branch blocks may appear
6. Hypertrophic Cardiomyopathy (HCM)
Disease overview: HCM is a genetic disorder (most commonly mutations in sarcomere proteins like beta-myosin heavy chain) characterized by asymmetric LV hypertrophy, particularly of the interventricular septum. It is the most common cause of sudden cardiac death in young athletes.
ECG changes (Goldman-Cecil Medicine; Tintinalli's Emergency Medicine):
- LVH voltage criteria present in the majority: deep S in V1-V3, tall R in V5-V6
- Narrow (septal) Q waves in leads I, aVL, V5, V6 - a characteristic finding due to the hypertrophied septum depolarizing abnormally; typically narrow (<40 ms) unlike ischemic Q waves
- T-wave upright in leads with septal Q waves (unlike ischemic pattern where T inversion accompanies Q waves)
- Giant negative T waves in mid-precordial leads (V3-V5) in the apical variant (Yamaguchi variant HCM)
- Inferolateral repolarization changes: Q waves or repolarization abnormalities in an athlete favor HCM diagnosis over athlete's heart
- Atrial fibrillation may be present (from left atrial enlargement)
- Voltage criteria for LVH: deep S wave up to 28 mm in V3 has been documented
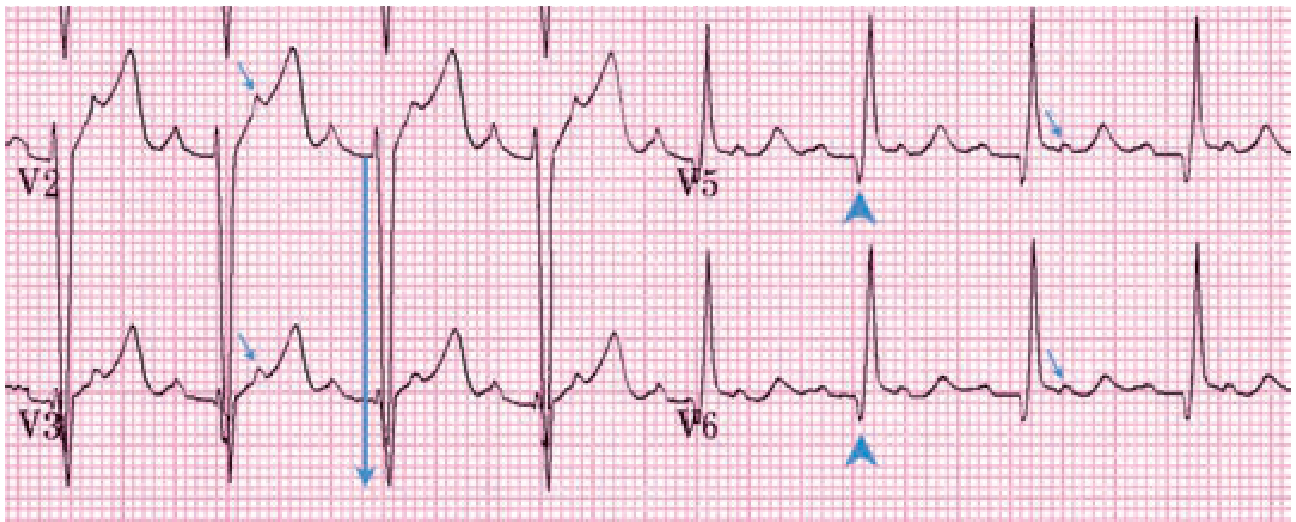
HCM ECG (Tintinalli's Emergency Medicine): Deep S-wave voltage (28 mm in V3, downward arrow), narrow septal Q waves in V5 and V6 (arrowheads), upright T waves in leads with septal Qs. Additional P waves in ST segments (small arrows) indicate coexisting atrial flutter with 2:1 block.
7. Aortic Stenosis (AS)
Disease overview: AS is progressive narrowing of the aortic valve orifice, causing left ventricular outflow obstruction and pressure overload. Causes include calcific degeneration (elderly), bicuspid aortic valve, and rheumatic disease. Classic triad: angina, syncope, heart failure.
ECG changes (Goldman-Cecil Medicine; Grainger & Allison's Radiology):
- LVH: The most consistent ECG finding; present in most symptomatic patients. LVH may be absent even in severe AS if the ventricle has not dilated.
- Left atrial abnormality ("P mitrale"): Broad notched P waves in lead II, reflecting elevated left atrial pressure
- LV strain pattern: Downsloping ST depression with T-wave inversion in V5-V6 and lateral limb leads
- Left axis deviation
- LBBB or left anterior fascicular block may be seen in advanced disease
- When fibrosis progresses: complete AV block (rare but important - suggests severe conduction system disease)
8. Acute Pericarditis
Disease overview: Inflammation of the pericardium, most commonly caused by viral infection (Coxsackievirus, echovirus), autoimmune disease, post-MI (Dressler's syndrome), uremia, or malignancy. Presents with sharp pleuritic chest pain, pericardial friction rub, and characteristic ECG evolution.
ECG changes - 4-stage evolution (Braunwald's Heart Disease; Fuster & Hurst's The Heart; Goldman-Cecil Medicine):
| Stage | Timing | ECG findings |
|---|---|---|
| Stage 1 (acute) | Days 1-2 | Diffuse (non-territory-specific) ST elevation in nearly all leads EXCEPT aVR and V1; PR depression in same leads; PR elevation in aVR - the most specific finding |
| Stage 2 | Days 3-7 | ST segments normalize; PR returns to baseline |
| Stage 3 | Weeks 1-3 | Diffuse T-wave inversion (after ST normalizes) |
| Stage 4 | Weeks-months | ECG normalizes completely |
Key distinguishing features from STEMI:
- Diffuse distribution (not territory-specific)
- PR depression present (absent in STEMI)
- No reciprocal ST depression (except in aVR)
- No pathological Q waves
- Concave ("saddle-shaped") ST elevation vs. the convex (dome-shaped) elevation of STEMI
- Electrical alternans if pericardial effusion develops (alternating QRS amplitude)
9. Complete Heart Block (Third-Degree AV Block)
Disease overview: Complete AV block means no atrial impulses conduct to the ventricles. The ventricles are driven by an escape pacemaker (junctional or ventricular). Causes include ischemia (inferior MI most common - RCA supplies AV node), Lyme disease, digoxin toxicity, sarcoidosis, and degenerative disease (Lenègre disease).
ECG changes:
- Complete AV dissociation: P waves and QRS complexes are entirely independent; no relationship between P and QRS
- Regular P-P intervals (sinus or atrial rate, usually 60-100 bpm)
- Regular but slow RR intervals: Escape rhythm rate depends on escape pacemaker location:
- Junctional escape: 40-60 bpm, narrow QRS (<120 ms)
- Ventricular escape: 20-40 bpm, wide QRS (>120 ms), bizarre morphology
- PR interval varies completely with no consistent relationship
- More P waves than QRS complexes
- In inferior MI-related block: usually junctional escape (narrow QRS, better prognosis)
- In anterior MI-related block: usually ventricular escape (wide QRS, poor prognosis)
10. Pulmonary Embolism (PE)
Disease overview: PE occurs when thrombus (usually from deep vein thrombosis) occludes pulmonary arteries, causing acute right ventricular pressure overload. Massive PE causes acute cor pulmonale and can be rapidly fatal. The ECG reflects acute right heart strain.
ECG changes:
- Sinus tachycardia: The most common ECG finding (>40% of cases); non-specific but often the first sign
- S1Q3T3 pattern: S wave in lead I + Q wave in lead III + T-wave inversion in lead III - the "classic" but insensitive (seen in ~20%) sign of acute right heart strain
- Right bundle branch block (RBBB): New incomplete or complete RBBB reflects acute right ventricular dilation; RSR' pattern in V1
- Right axis deviation
- T-wave inversions in right precordial leads (V1-V4): Reflects RV strain; anterior T-wave inversions extending to V4 are a helpful sign in the right clinical context
- P pulmonale: Peaked P waves in lead II >2.5 mm (right atrial overload)
- Atrial fibrillation or flutter: May be precipitated by PE
- Low voltage or electrical alternans if large effusion coexists
- Note: ECG is normal in up to 30% of PE cases
Quick-Reference Summary Table
| Disease | Rhythm | Key ECG Findings |
|---|---|---|
| STEMI | Usually sinus | ST elevation (territory-specific), Q waves, reciprocal changes |
| NSTEMI / UA | Usually sinus | ST depression, T-wave inversion, no Q waves |
| Atrial Fibrillation | Irregularly irregular | No P waves, irregular RR, f-waves |
| Heart Failure (HFrEF) | Sinus tachy or AF | LVH, LBBB, LAE, ST-T changes |
| Hypertensive HD | Sinus | LVH + strain pattern, LAE |
| HCM | Sinus (or AF/flutter) | LVH, narrow septal Q waves, giant T inversions (apical) |
| Aortic Stenosis | Sinus | LVH, LV strain, LAE, LAD |
| Acute Pericarditis | Sinus | Diffuse saddle ST elevation, PR depression, T inversions (stage 3) |
| Complete Heart Block | Dissociation | P-QRS dissociation, slow escape rhythm |
| Pulmonary Embolism | Sinus tachycardia | S1Q3T3, RBBB, right precordial T inversions, RAD |
Sources: Guyton & Hall Textbook of Medical Physiology (Elsevier); Goldman-Cecil Medicine; Braunwald's Heart Disease; Tintinalli's Emergency Medicine; Fuster & Hurst's The Heart, 15th ed.; Rosen's Emergency Medicine; Harrison's Principles of Internal Medicine 22E; Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.