Explain renal tubular acidosisfor neet pg
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have very rich data from multiple authoritative textbooks. Let me compile the comprehensive NEET PG-focused answer.
Renal Tubular Acidosis (RTA) - Complete NEET PG Guide
Definition
RTA is a group of disorders characterized by hyperchloremic, normal anion gap (NAGMA) metabolic acidosis resulting from impaired renal tubular H+ secretion or HCO3- reabsorption, despite a normal or near-normal GFR.
Key distinguishing features from acidosis of renal failure:
- Normal anion gap (no retention of phosphate, sulfate)
- GFR is normal or only mildly reduced
- Inappropriately high urine pH for the degree of systemic acidosis
Normal Renal Acid-Base Physiology (Quick Review)
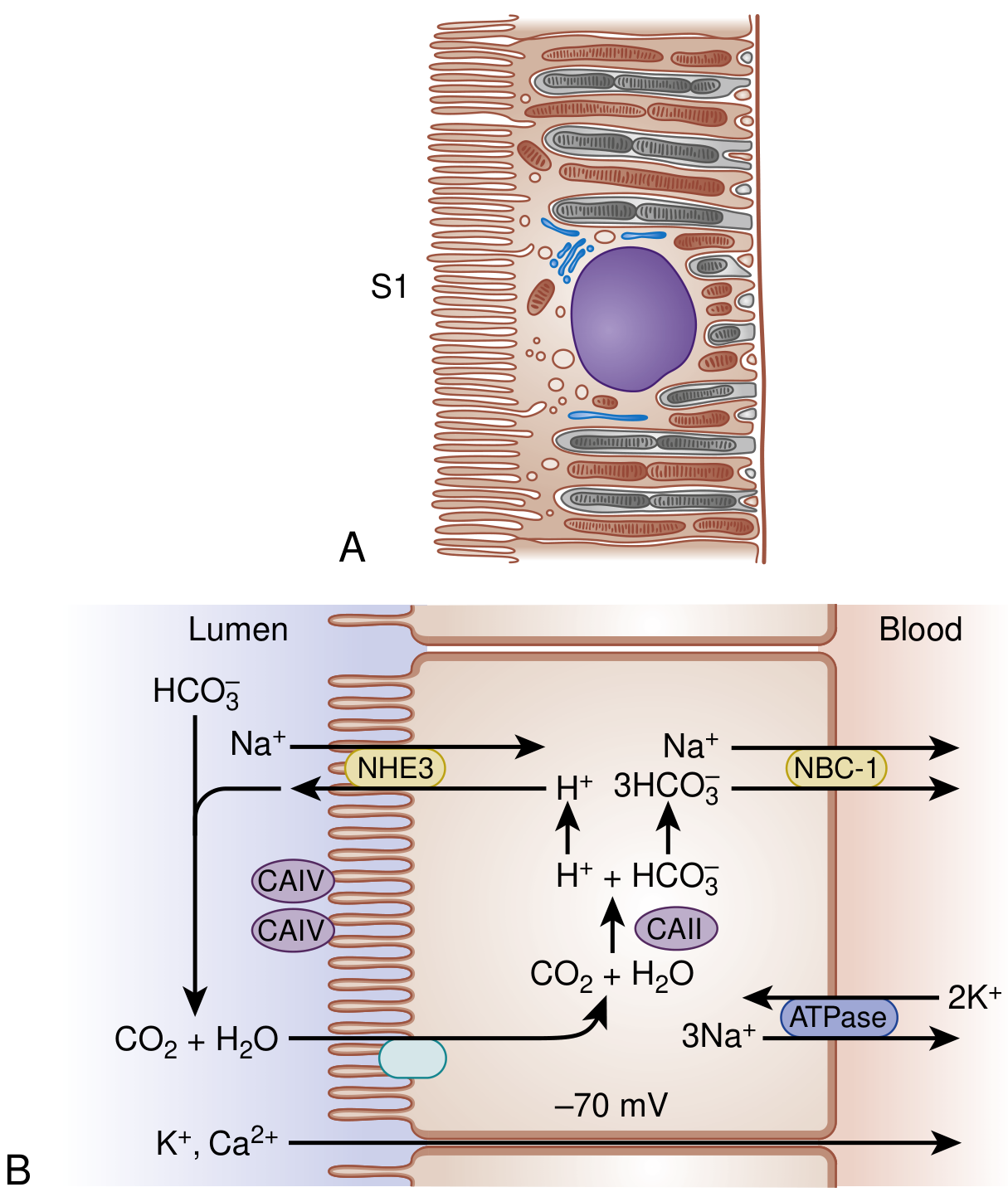
Proximal tubule: Reabsorbs ~85-90% of filtered HCO3- via Na+/H+ exchanger (NHE3) on the apical side and Na+/HCO3- cotransporter (NBC1) on the basolateral side. Carbonic anhydrase (CA) is essential.
Distal tubule / collecting duct: Site of net H+ excretion via H+-ATPase and H+/K+-ATPase on alpha-intercalated cells. Creates up to 1000:1 H+ gradient, lowering urine pH to as low as 4.5. H+ is buffered by NH3 (as NH4+) and titratable acid (HPO4--).
Classification of RTA
| Type | Name | Defect | Serum K+ | Urine pH | Urine AG |
|---|---|---|---|---|---|
| Type 1 | Distal RTA | Failure of H+ secretion in collecting duct | Low (hypokalemia) | >5.5 (always) | Positive |
| Type 2 | Proximal RTA | Impaired HCO3- reabsorption in proximal tubule | Low (hypokalemia) | Variable (<5.5 at baseline, >5.5 with alkali) | Positive |
| Type 3 | Mixed (rare) | Carbonic anhydrase II deficiency | - | - | - |
| Type 4 | Hypoaldosteronism | Aldosterone deficiency/resistance | High (hyperkalemia) | <5.5 | Positive |
TYPE 1 RTA - Distal RTA (Most Common, Most Important for NEET PG)
Mechanism
- Failure of alpha-intercalated cells to secrete H+ into the collecting duct
- Subtypes:
- Proton secretion defect (most common) - H+-ATPase mutation or damage
- Back-leak defect - H+ secreted but leaks back through damaged apical membrane (classic with amphotericin B)
- Voltage-dependent (hyperkalemic) - reduced ENaC activity impairs both H+ and K+ secretion
Key Features
- Hypokalemia + hyperchloremic NAGMA
- Urine pH persistently >5.5 even in systemic acidosis (hallmark)
- Nephrocalcinosis and nephrolithiasis (calcium phosphate/oxalate stones) in up to 70% - caused by:
- Hypercalciuria (bone buffering releases calcium)
- Hypocitraturia (citrate reabsorption increased due to intracellular acidosis)
- Alkaline urine favors calcium phosphate precipitation
- Bone disease (osteomalacia, rickets in children)
- Urine anion gap (UAG) = positive (Na+ + K+ - Cl- is positive, indicating low NH4+)
Causes
Inherited:
- ATP6V1B1 mutations (H+-ATPase B1 subunit) - autosomal recessive with sensorineural deafness
- SLC4A1 mutations (anion exchanger AE1, Cl-/HCO3-) - autosomal dominant or recessive
- Medullary sponge kidney
Acquired:
- Autoimmune: Sjögren syndrome (most common cause in adults), SLE, rheumatoid arthritis, primary biliary cirrhosis
- Drugs: Amphotericin B (back-leak), lithium, ifosfamide, topiramate, acetazolamide
- Hypergammaglobulinemia
Key Points for NEET PG
- Most common cause of RTA associated with stone formation
- Classic association: Sjögren syndrome + distal RTA
- Amphotericin B = classic drug causing type 1 RTA (back-leak mechanism)
- Bone disease is common; nephrocalcinosis is a hallmark
- Hypokalemia worsens with treatment (alkali increases distal K+ loss)
Treatment
- Oral NaHCO3 or potassium citrate (preferred - also corrects hypokalemia and hypocitraturia)
- Modest doses ~1-3 mEq/kg/day
- Potassium supplementation required
TYPE 2 RTA - Proximal RTA
Mechanism
- Reduced bicarbonate reabsorption in the proximal tubule (threshold lowered from normal 22 mmol/L to ~15 mmol/L)
- Once plasma HCO3- falls below the new threshold, what's filtered is fully reabsorbed and urine acidifies normally
- Isolated proximal RTA is rare; most often occurs as part of Fanconi syndrome
Fanconi Syndrome
Generalized proximal tubular dysfunction causing loss of:
- HCO3- (RTA)
- Glucose (glycosuria with normal plasma glucose)
- Amino acids (aminoaciduria)
- Phosphate (hypophosphatemia, rickets)
- Uric acid (hypouricemia)
- Low-molecular-weight proteins
- Potassium, sodium
Key Features
- Hypokalemia + NAGMA
- Urine pH < 5.5 at baseline (distal acidification intact), but > 5.5 after alkali therapy (HCO3- spills into distal tubule)
- Fractional excretion of HCO3- > 10-15% when serum HCO3- > 20 mmol/L (diagnostic)
- Nephrocalcinosis is rare (unlike type 1)
- Metabolic bone disease (hypophosphatemia driven rickets/osteomalacia) is common
Causes
- Genetic: Cystinosis (most common in children), Wilson disease, tyrosinemia, galactosemia, hereditary fructose intolerance, Lowe syndrome
- Drugs: Tenofovir (HIV treatment), ifosfamide, cidofovir, adefovir, aristolochic acid, heavy metals (lead, mercury, cadmium)
- Multiple myeloma (light chain deposits)
- Sjögren syndrome, renal transplant rejection
Key Points for NEET PG
- Cystinosis is the most common cause in children
- Multiple myeloma is a key cause in adults
- Tenofovir (nucleoside reverse transcriptase inhibitor) = important drug cause
- Paradox: Alkali treatment worsens hypokalemia (enhanced HCO3- delivery to distal nephron increases K+ secretion)
- High doses of NaHCO3 required (up to 10-15 mEq/kg/day in children) + K+ supplementation
Treatment
- High-dose oral NaHCO3 or K-citrate (requires large amounts because HCO3- is rapidly lost in urine)
- Treat underlying cause
- Phosphate supplementation + vitamin D for rickets
TYPE 4 RTA - Hyperkalemic RTA (Most Common Type Overall)
Mechanism
- Aldosterone deficiency or resistance → failure of distal K+ and H+ secretion
- Aldosterone normally promotes Na+ reabsorption (via ENaC), creating a lumen-negative potential that drives both K+ and H+ secretion
- Without aldosterone effect: Hyperkalemia + mild metabolic acidosis
- Hyperkalemia itself impairs renal ammonia synthesis, further worsening acid excretion
Key Features
- Hyperkalemia (hallmark, distinguishes from types 1 and 2)
- Mild NAGMA (HCO3- usually 15-20 mEq/L, less severe than types 1/2)
- Urine pH < 5.5 (distal H+-ATPase intact, but NH4+ excretion low due to hyperkalemia)
- Urine AG positive
- Most common in diabetic nephropathy (hyporeninemic hypoaldosteronism)
Causes
Aldosterone Deficiency:
- Hyporeninemic hypoaldosteronism (most common) - diabetic nephropathy, tubulointerstitial disease, NSAIDs, chronic urinary obstruction
- Adrenal insufficiency (Addison's disease)
- Heparin (inhibits aldosterone synthesis)
Aldosterone Resistance (Pseudohypoaldosteronism):
- PHA Type I (autosomal dominant - mineralocorticoid receptor mutation; autosomal recessive - ENaC mutation)
- PHA Type II / Gordon syndrome (WNK kinase mutations)
Drugs:
- Spironolactone, eplerenone (aldosterone antagonists)
- Amiloride, triamterene (ENaC blockers)
- ACE inhibitors, ARBs
- Trimethoprim (blocks ENaC)
- Calcineurin inhibitors (cyclosporine, tacrolimus)
Key Points for NEET PG
- Most common cause: Diabetic nephropathy (hyporeninemic hypoaldosteronism)
- Urine pH is usually < 5.5 (acid urine - intact H+-ATPase, just reduced NH4+ buffer)
- This is the most common type of RTA overall
- Mild acidosis compared to types 1 and 2
Treatment
- Treat underlying cause
- Fludrocortisone if true aldosterone deficiency
- Loop diuretics (furosemide) to promote K+ excretion and stimulate aldosterone
- Low potassium diet, cation exchange resins
- Avoid drugs that worsen hyperkalemia
TYPE 3 RTA (Rare - Know for Completion)
- Mixed proximal + distal defect
- Caused by carbonic anhydrase II (CA II) deficiency (recessive mutation)
- Triad: Osteopetrosis + cerebral calcification + mental retardation
- "Type 3" label is sometimes abandoned; considered a variant
Urine Anion Gap (UAG) - Key Diagnostic Tool
UAG = (Urine Na+ + Urine K+) - Urine Cl-
- Positive UAG → low urine NH4+ → renal tubular cause of acidosis (all types of RTA)
- Negative UAG → high urine NH4+ → extrarenal cause (e.g., diarrhea)
Why does UAG estimate NH4+?
NH4+ is excreted with Cl- (as NH4Cl), so when NH4+ excretion is high, urine Cl- is high, making UAG negative.
Summary Comparison Table (High-Yield NEET PG)
| Feature | Type 1 (Distal) | Type 2 (Proximal) | Type 4 (Hyperkalemic) |
|---|---|---|---|
| Defect site | Collecting duct | Proximal tubule | Collecting duct |
| Primary defect | H+ secretion failure | HCO3- reabsorption failure | Aldosterone def/resistance |
| Serum K+ | Low | Low | High |
| Urine pH | Always >5.5 | <5.5 at baseline, >5.5 with alkali | <5.5 |
| FE-HCO3- | <5% | >10-15% | <5% |
| Nephrocalcinosis | Yes (common) | Rare | Absent |
| Nephrolithiasis | Yes (70%) | Rare | Absent |
| Bone disease | Yes (osteomalacia) | Yes (rickets) | Mild |
| Serum HCO3- | Very low | Low-moderate | Mild reduction |
| Key association | Sjögren, ampho B | Fanconi, cystinosis, tenofovir | Diabetic nephropathy |
| Treatment | Low-dose alkali | High-dose alkali + K+ | Fludrocortisone/furosemide |
High-Yield NEET PG One-Liners
- Type 1 RTA = distal, hypokalemia, urine pH always >5.5, nephrocalcinosis, Sjögren syndrome
- Amphotericin B = type 1 RTA (back-leak proton gradient defect)
- Type 2 RTA = proximal, Fanconi syndrome, urine pH <5.5 at baseline but >5.5 with treatment
- Cystinosis = most common genetic cause of Fanconi syndrome/type 2 RTA in children
- Tenofovir = type 2 RTA / Fanconi syndrome (used in HIV treatment)
- Type 4 RTA = hyperkalemic, urine pH <5.5, most common cause = diabetic nephropathy (hyporeninemia)
- UAG positive = RTA; UAG negative = diarrhea (extrarenal HCO3- loss)
- Type 3 RTA = carbonic anhydrase II deficiency, osteopetrosis + cerebral calcification
- Nephrocalcinosis: Type 1 > never in type 2 or 4
- Alkali therapy worsens hypokalemia in Type 2 RTA (increased K+ wasting in distal tubule)
- Gordon syndrome (PHA II) = type 4 RTA due to WNK kinase mutations - hyperkalemia, hypertension
Sources: Brenner and Rector's The Kidney; Harrison's Principles of Internal Medicine 22E; Campbell-Walsh-Wein Urology; Tietz Textbook of Laboratory Medicine 7th Ed.
Normal renal physiology regarding nephrons in simolest words
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Great images retrieved. Now I have everything needed for a clear, simple explanation. Let me compose the answer.
Normal Renal Physiology - The Nephron (Simplest Words)
What is a Nephron?
Think of a nephron as a tiny cleaning unit inside the kidney. Each kidney has about 1 million nephrons. Together, they filter your entire blood volume about 60 times a day.
One nephron = one glomerulus + one long tubule
The Big Picture: What a Nephron Does
Blood enters → gets filtered → the filtrate is modified (good stuff kept, bad stuff removed) → final product = urine
There are 3 main processes:
- Filtration - push fluid out of blood into the tubule
- Reabsorption - take back the good stuff from tubule into blood
- Secretion - dump extra waste from blood into tubule
Parts of the Nephron - One by One (Simple)
BLOOD → Glomerulus → Bowman's Capsule → Proximal Tubule
→ Loop of Henle → Distal Convoluted Tubule
→ Collecting Duct → URINE
1. GLOMERULUS + BOWMAN'S CAPSULE (The Filter)
- The glomerulus is a ball of tiny blood vessels (capillaries)
- Blood is pushed under pressure through these capillaries
- Water, salts, glucose, urea, amino acids - everything small - gets squeezed out into Bowman's capsule
- Big things stay in blood: red blood cells, proteins, platelets
- What enters the tubule = glomerular filtrate (~180 L/day!)
- Normal GFR = 125 mL/min (90-120 in women)
Think of it like a coffee filter - water and small particles pass through, big chunks stay behind.
2. PROXIMAL CONVOLUTED TUBULE - PCT (The Workhorse)
- Reabsorbs 60-70% of the filtrate - the bulk of the work
- Has a brush border (lots of tiny finger-like projections = microvilli) to increase surface area
- What gets reabsorbed here:
- All glucose (via SGLT2 cotransporter)
- All amino acids
- ~85-90% of HCO3- (bicarbonate - via NHE3 exchanger + carbonic anhydrase)
- ~67% of Na+, water, Cl- (water follows sodium passively via aquaporin-1)
- Phosphate (regulated by PTH - PTH inhibits reabsorption)
- Uric acid
- Also secretes organic acids, drugs (penicillin, methotrexate), creatinine
The PCT is the "bulk recovery" station - it grabs back almost everything useful before the filtrate moves on.
Key transporters in PCT:
- NHE3 (apical) - Na+ in, H+ out (drives HCO3- reabsorption)
- Na+/K+-ATPase (basolateral) - the master pump that keeps everything moving
- NBC-1 (basolateral) - moves HCO3- back into blood
3. LOOP OF HENLE (The Concentrating Machine)
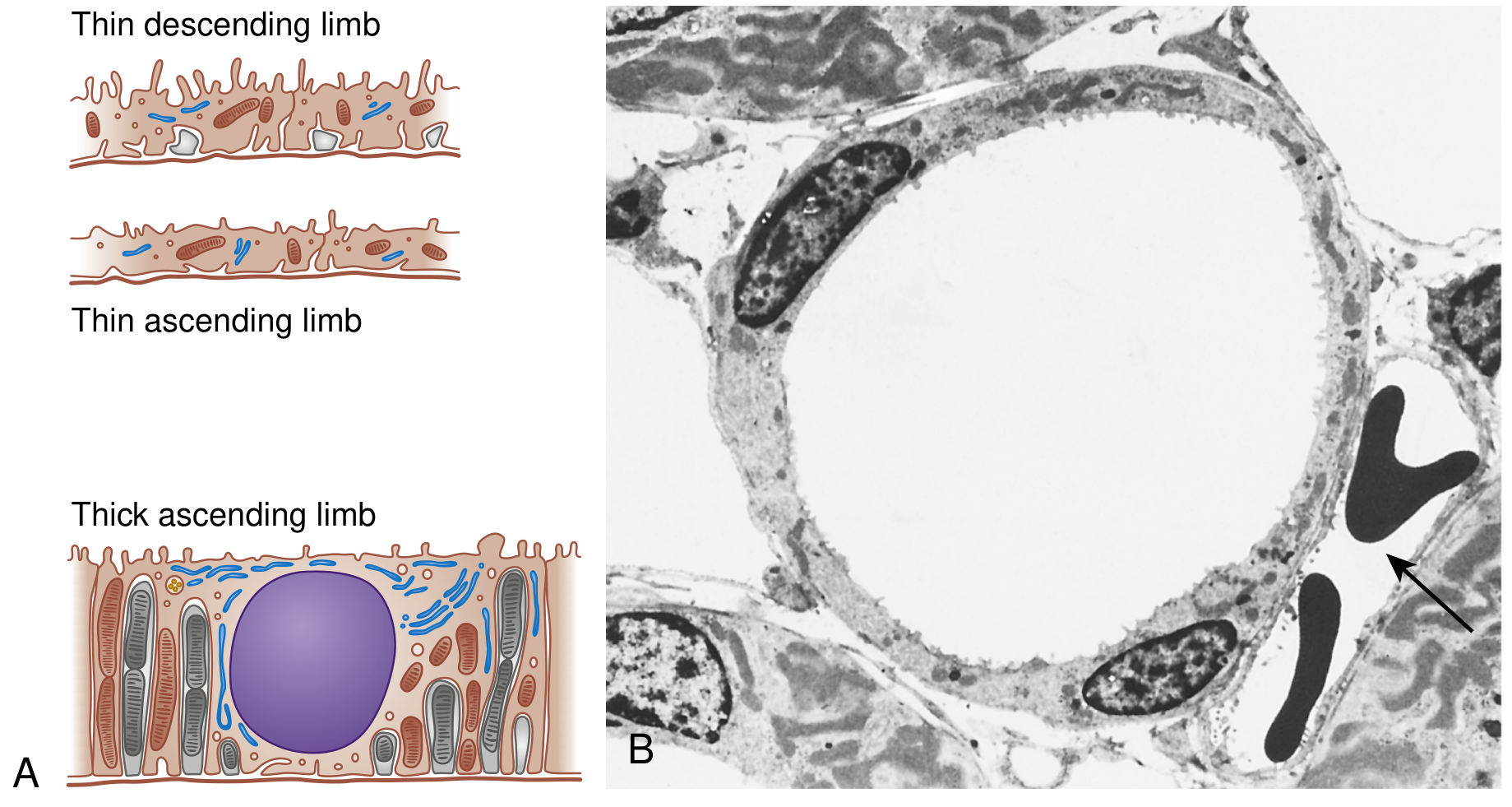
It makes a U-turn deep into the kidney's medulla. This is what allows the kidney to make concentrated urine.
Thin Descending Limb
- Permeable to water (aquaporin-1), NOT to salt
- Water is sucked out into the salty medulla
- Filtrate becomes concentrated (more salty) as it goes down
Thin Ascending Limb
- Permeable to salt (NaCl diffuses out passively), NOT to water
- Filtrate starts to dilute
Thick Ascending Limb (TAL)
- Impermeable to water - this is the key!
- Actively pumps Na+, K+, 2Cl- out using NKCC2 (the target of furosemide/loop diuretics)
- K+ is recycled back into lumen via ROMK channel
- Creates a very salty medulla (600-1200 mOsm) = the concentration gradient
- Since salt leaves but water can't, the filtrate becomes dilute in the TAL
Think of the Loop of Henle like a salt pump that makes the surrounding tissue very salty. This saltiness is used later to pull water out of urine and concentrate it.
The Macula Densa sits at the end of TAL where it touches the glomerulus. It senses how much NaCl is in the tubule and sends signals back to the glomerulus to adjust filtration rate - this is called tubuloglomerular feedback (TGF).
4. DISTAL CONVOLUTED TUBULE - DCT (Fine Tuning)
- Very short segment (10-12 mm)
- Impermeable to water → more dilution occurs
- Main transporter: NCC (Na+/Cl- cotransporter) - target of thiazide diuretics
- Fine-tunes Na+, Ca2+, Mg2+
- PTH acts here to increase Ca2+ reabsorption (via TRPV5 channel)
- Aldosterone starts acting here (ENaC channels appear in late DCT)
DCT = the "fine adjustment" dial for Na+ and Ca2+.
5. COLLECTING DUCT (Final Decision Maker)
This is where the kidney makes its final decision on how much water and electrolytes to keep or lose. It has two cell types:
Principal Cells (Na+ and Water)
- Under aldosterone → opens ENaC (sodium channel) on luminal side
- Na+ enters → creates a negative charge in the lumen
- This negative charge pulls K+ out via ROMK channel (potassium secretion)
- Under ADH (vasopressin) → inserts aquaporin-2 into the luminal membrane
- Water is reabsorbed along concentration gradient
- Without ADH → water stays in tubule → dilute urine (as in diabetes insipidus)
Alpha-Intercalated Cells (Acid-Base)
- Secrete H+ via H+-ATPase (luminal side)
- Reabsorb HCO3- via Cl-/HCO3- exchanger (basolateral)
- Makes the urine acidic - can lower urine pH to 4.5
Beta-Intercalated Cells (Alkalosis correction)
- Do the opposite: secrete HCO3- into lumen (via pendrin)
- Used when blood is too alkalotic
The collecting duct is the final filter - controlled by hormones (ADH and aldosterone) to produce the exact urine volume and composition the body needs.
Summary Table - Each Segment at a Glance
| Segment | Main Job | What's Reabsorbed | Special Note |
|---|---|---|---|
| Glomerulus | Filter blood | Nothing (filtration only) | GFR = 125 mL/min |
| PCT | Bulk recovery | 65% Na+/water, ALL glucose + amino acids, 85% HCO3- | Brush border; site of Fanconi syndrome |
| Descending Loop | Concentrate filtrate | Water only | Permeable to H2O, not salt |
| Thick Ascending Loop (TAL) | Create medullary gradient | Na/K/2Cl (no water) | NKCC2; furosemide acts here |
| DCT | Fine-tune Na+, Ca2+ | Na+, Cl-, Ca2+ | NCC; thiazides act here |
| Collecting Duct | Final urine concentration | Water (ADH), Na+ (aldosterone) | H+ secretion; acid-base control |
Key Hormones and Their Targets
| Hormone | Acts Where | Does What |
|---|---|---|
| Aldosterone | Late DCT + Collecting duct | ↑ Na+ reabsorption, ↑ K+ secretion, ↑ H+ secretion |
| ADH (Vasopressin) | Collecting duct | ↑ Water reabsorption (AQP-2 insertion) |
| PTH | PCT (↓ phosphate) + DCT (↑ Ca2+) | ↓ Phosphate reabsorption, ↑ Ca2+ reabsorption |
| ANP | Glomerulus + Collecting duct | ↑ GFR, ↓ Na+ reabsorption |
The Final Numbers (Important for Exams)
- Blood filtered per day: ~180 L
- Urine produced per day: ~1.5 L
- So 99% is reabsorbed!
- Normal GFR: 125 mL/min (90-120 in women)
- Renal plasma flow: 650 mL/min
- Filtration fraction = GFR/RPF = 125/650 = ~0.2 (20%)
One-Line Memory Tricks
- PCT = "Please Come Take" glucose, amino acids, bicarb (everything useful)
- Descending loop = "Water leaves" (permeable to water)
- Ascending loop (TAL) = "Salt leaves, water stays" (NKCC2, impermeable to water)
- DCT = "Dial" (fine-tunes Ca, Na)
- Collecting duct = "Final boss" (ADH + Aldosterone control)
- Furosemide = blocks NKCC2 in TAL
- Thiazides = block NCC in DCT
- Spironolactone/Amiloride = block collecting duct (aldosterone pathway)
Sources: National Kidney Foundation Primer on Kidney Diseases 8e; Brenner and Rector's The Kidney
Based on these type of question most frequently asked in neet pg
Based on the two topics we covered (Renal Tubular Acidosis + Normal Nephron Physiology), here are the most frequently asked NEET PG style MCQs with explanations:
NEET PG MCQs - Renal Tubular Acidosis & Nephron Physiology
SECTION A: RENAL TUBULAR ACIDOSIS
Q1. A 35-year-old woman presents with recurrent renal stones and is found to have hypokalemia, hyperchloremic metabolic acidosis, and urine pH of 6.5 despite systemic acidosis. Which condition is most likely associated?
- A) Sjögren syndrome
- B) Diabetes mellitus
- C) Multiple myeloma
- D) Cystinosis
Answer: A) Sjögren syndrome
Type 1 (distal) RTA - urine pH always >5.5 + hypokalemia + nephrolithiasis. Most common acquired cause in adults = Sjögren syndrome. Diabetes → Type 4 RTA. Multiple myeloma → Type 2 RTA. Cystinosis → Type 2 RTA in children.
Q2. A patient on Amphotericin B develops metabolic acidosis. The mechanism of RTA in this case is:
- A) Decreased HCO3- reabsorption in PCT
- B) Back-leak of H+ through damaged apical membrane
- C) Aldosterone deficiency
- D) Reduced H+/K+-ATPase synthesis
Answer: B) Back-leak of H+ through damaged apical membrane
Amphotericin B increases membrane permeability in the collecting duct → secreted H+ leaks back into the cell → cannot maintain H+ gradient → Type 1 RTA (back-leak subtype).
Q3. Which type of RTA is associated with nephrocalcinosis and nephrolithiasis in up to 70% of patients?
- A) Type 2
- B) Type 4
- C) Type 1
- D) Type 3
Answer: C) Type 1
Distal RTA causes alkaline urine + hypercalciuria + hypocitraturia → ideal conditions for calcium phosphate stone/nephrocalcinosis formation. Type 2 and 4 rarely cause stones.
Q4. A child presents with rickets, glycosuria (normal blood glucose), aminoaciduria, and phosphaturia. The most likely cause is:
- A) Type 1 RTA
- B) Fanconi syndrome (Type 2 RTA)
- C) Type 4 RTA
- D) Bartter syndrome
Answer: B) Fanconi syndrome (Type 2 RTA)
Fanconi syndrome = generalized PCT dysfunction → loses glucose, amino acids, phosphate, uric acid, HCO3-. Classic presentation: rickets + glycosuria with normal blood glucose.
Q5. A patient with HIV on Tenofovir develops metabolic acidosis, glycosuria, phosphaturia, and aminoaciduria. Which type of RTA is this?
- A) Type 1
- B) Type 2
- C) Type 3
- D) Type 4
Answer: B) Type 2
Tenofovir causes Fanconi syndrome/Type 2 (proximal) RTA. Other drugs: ifosfamide, cidofovir, aristolochic acid.
Q6. A diabetic patient on ACE inhibitor has mild metabolic acidosis with serum K+ = 6.2 mEq/L. Urine pH = 5.0. What is the diagnosis?
- A) Type 1 RTA
- B) Type 2 RTA
- C) Type 4 RTA
- D) Diarrhea-induced acidosis
Answer: C) Type 4 RTA
Type 4 RTA = hyperkalemia + mild NAGMA + urine pH <5.5 (H+-ATPase intact but NH4+ low due to hyperkalemia). Most common cause = diabetic nephropathy (hyporeninemic hypoaldosteronism). ACE inhibitor worsens it.
Q7. In Type 2 RTA, alkali therapy with NaHCO3 paradoxically:
- A) Raises serum K+ further
- B) Worsens hypokalemia
- C) Normalizes urine pH permanently
- D) Reduces nephrocalcinosis
Answer: B) Worsens hypokalemia
NaHCO3 delivers more HCO3- to the distal tubule → increased K+ secretion → worsening hypokalemia. That is why K+ supplementation is always co-administered.
Q8. Urine anion gap (UAG) is calculated as:
- A) Serum (Na+ + K+) - Serum Cl-
- B) Urine Na+ - Urine Cl-
- C) Urine (Na+ + K+) - Urine Cl-
- D) Urine Na+ + Urine K+ + Urine Cl-
Answer: C) Urine (Na+ + K+) - Urine Cl-
A positive UAG = low urine NH4+ = renal cause (RTA). A negative UAG = high urine NH4+ = extrarenal cause (diarrhea). NH4+ is excreted with Cl-, so high NH4+ → high Cl- → UAG becomes negative.
Q9. Type 3 RTA is associated with which classic triad?
- A) Deafness + rickets + nephrocalcinosis
- B) Osteopetrosis + cerebral calcification + mental retardation
- C) Polyuria + polydipsia + hyperkalemia
- D) Glycosuria + aminoaciduria + hyperphosphatemia
Answer: B) Osteopetrosis + cerebral calcification + mental retardation
Type 3 RTA = Carbonic anhydrase II (CA-II) deficiency. CA-II is needed in both PCT and DCT + osteoclasts + brain. Deficiency → mixed RTA + osteopetrosis (osteoclasts fail to resorb bone) + cerebral calcification.
Q10. Which drug causes Type 1 RTA by specifically blocking the H+-ATPase?
- A) Amphotericin B
- B) Acetazolamide
- C) Topiramate
- D) Lithium
Answer: C) Topiramate
Topiramate and acetazolamide inhibit carbonic anhydrase → reduce H+ generation → Type 1 (and Type 2) RTA. Amphotericin B → back-leak. Lithium → nephrogenic DI but can also cause Type 1 RTA by damaging collecting duct cells.
SECTION B: NEPHRON PHYSIOLOGY
Q11. The normal Glomerular Filtration Rate (GFR) in an adult male is:
- A) 90 mL/min
- B) 125 mL/min
- C) 180 mL/min
- D) 650 mL/min
Answer: B) 125 mL/min
GFR = 125 mL/min. Total filtrate/day = 180 L. Renal plasma flow = 650 mL/min. Filtration fraction = GFR/RPF = 125/650 = ~20%.
Q12. Furosemide (loop diuretic) acts by blocking which transporter?
- A) NHE3 in PCT
- B) NCC in DCT
- C) NKCC2 in thick ascending limb
- D) ENaC in collecting duct
Answer: C) NKCC2 in thick ascending limb
NKCC2 = Na-K-2Cl cotransporter in TAL. Furosemide blocks it → no salt reabsorption → no concentration gradient → dilute urine + loss of Na, K, Cl. TAL is also impermeable to water → this is where dilution happens.
Q13. Which segment of the nephron is impermeable to water and actively pumps out Na/K/2Cl, thereby creating the medullary concentration gradient?
- A) Thin descending limb
- B) Proximal convoluted tubule
- C) Thick ascending limb of loop of Henle
- D) Collecting duct
Answer: C) Thick ascending limb of loop of Henle
TAL is called the diluting segment - salt leaves, water cannot → filtrate becomes dilute, medulla becomes hypertonic. This gradient is what allows ADH to concentrate urine in the collecting duct.
Q14. ADH (Vasopressin) acts on the collecting duct to insert which water channel?
- A) Aquaporin-1
- B) Aquaporin-2
- C) Aquaporin-4
- D) ROMK
Answer: B) Aquaporin-2
ADH → V2 receptor → cAMP → AQP-2 vesicles inserted into luminal membrane → water reabsorption. AQP-1 is always present in PCT and descending loop (not regulated). Absence of AQP-2 = Nephrogenic Diabetes Insipidus.
Q15. Thiazide diuretics act on which transporter in which segment?
- A) NKCC2 in TAL
- B) NCC in DCT
- C) ENaC in collecting duct
- D) NHE3 in PCT
Answer: B) NCC in DCT
NCC = Na-Cl cotransporter in the Distal Convoluted Tubule. Thiazides block NCC → Na+ and water loss. Paradoxically used in nephrogenic DI because they cause mild volume depletion → enhanced PCT reabsorption → less water to collecting duct → less polyuria.
Q16. Parathyroid hormone (PTH) acts on the PCT to:
- A) Increase phosphate reabsorption
- B) Decrease phosphate reabsorption
- C) Increase glucose reabsorption
- D) Decrease calcium reabsorption
Answer: B) Decrease phosphate reabsorption
PTH inhibits Na+/phosphate cotransporter in PCT → phosphaturia → lowers serum phosphate. PTH simultaneously increases Ca2+ reabsorption in DCT. In hyperparathyroidism: ↓ phosphate + ↑ Ca2+.
Q17. Which hormone causes potassium secretion by the principal cells of the collecting duct?
- A) ADH
- B) Aldosterone
- C) PTH
- D) ANP
Answer: B) Aldosterone
Aldosterone → opens ENaC (Na+ enters) → lumen becomes negative → K+ exits via ROMK → K+ secretion. Also promotes H+ secretion from alpha-intercalated cells. Loss of aldosterone → hyperkalemia + metabolic acidosis (Type 4 RTA).
Q18. A patient is found to have glycosuria, aminoaciduria, phosphaturia with hypophosphatemia, hypouricemia, and low-molecular-weight proteinuria. Which segment of the nephron is primarily dysfunctional?
- A) Glomerulus
- B) Proximal convoluted tubule
- C) Loop of Henle
- D) Collecting duct
Answer: B) Proximal convoluted tubule
This is the classic description of Fanconi syndrome - all the substrates normally reabsorbed 100% in the PCT are lost. Glomerular disease → proteinuria (large proteins), not these findings.
Q19. The macula densa is located at which anatomical junction?
- A) Where PCT meets the loop of Henle
- B) Where the thick ascending limb returns to its own glomerulus
- C) Where the collecting duct opens into the renal pelvis
- D) At the tip of the loop of Henle
Answer: B) Where the thick ascending limb returns to its own glomerulus
Macula densa = specialized cells at the end of TAL that lie adjacent to the afferent arteriole of the same nephron's glomerulus. They sense NaCl concentration in tubular fluid and regulate GFR via tubuloglomerular feedback (TGF). Also stimulate renin secretion when NaCl is low.
Q20. In which condition does the thick ascending limb fail to reabsorb NaCl due to a genetic mutation in NKCC2 or ROMK, leading to hypokalemic metabolic alkalosis?
- A) Gitelman syndrome
- B) Bartter syndrome
- C) Liddle syndrome
- D) Gordon syndrome
Answer: B) Bartter syndrome
Bartter syndrome = genetic defect in TAL transporters (NKCC2, ROMK, ClC-Kb, Barttin) → mimics chronic furosemide use → hypokalemia + metabolic alkalosis + hypercalciuria + normal/low BP. Gitelman = DCT defect (NCC mutation) → hypokalemia + alkalosis + hypomagnesemia + hypocalciuria. Liddle = gain of function ENaC → hypertension + hypokalemia.
Quick Exam Cheat Sheet
| Diuretic | Site | Transporter blocked |
|---|---|---|
| Furosemide | TAL | NKCC2 |
| Thiazide | DCT | NCC |
| Amiloride/Triamterene | Collecting duct | ENaC |
| Spironolactone | Collecting duct | Aldosterone receptor |
| Acetazolamide | PCT | Carbonic anhydrase |
| RTA Type | K+ | Urine pH | Key association |
|---|---|---|---|
| Type 1 | Low | >5.5 always | Sjögren, Ampho B, nephrocalcinosis |
| Type 2 | Low | <5.5 baseline | Fanconi, cystinosis, tenofovir |
| Type 4 | High | <5.5 | Diabetic nephropathy, ACEi |
Not able to grasp RTA concepts
Let me rebuild RTA from scratch using pure logic and simple analogies. No jargon first - just the concept.
RTA - Built From Zero, Step by Step
STEP 1: Understand the ONE Problem in RTA
Your blood is becoming too acidic (metabolic acidosis).
Normally, the kidney fixes this by:
- Throwing acid (H+) out into urine
- Keeping alkali (HCO3-) in the blood
In RTA, the kidney fails to do this job - NOT because the kidneys are destroyed (GFR is normal), but because specific tubule parts are broken.
One sentence: RTA = kidney tubules can't handle acid properly, so blood becomes acidic even though the kidney is otherwise working fine.
STEP 2: The Simple Analogy
Think of your kidney tubule as a drain pipe with workers at different sections:
BLOOD → [Filter] → [Section A: PCT] → [Section B: Loop] → [Section C: DCT/Collecting duct] → URINE
- Section A workers (PCT) job = collect all the good alkali (HCO3-) and send it back to blood
- Section C workers (Collecting duct) job = dump acid (H+) into the urine drain
RTA happens when one of these worker teams fails.
STEP 3: Now Understand Each Type as a Story
🔴 TYPE 1 RTA - "The Acid Dumper is Broken"
Who broke down? = Workers at the collecting duct (distal nephron)
Their job: Pump H+ (acid) OUT into urine
What happens when they fail?
- H+ cannot be dumped into urine
- H+ builds up in blood → blood becomes acidic
- Urine NEVER becomes acidic → urine pH stays >5.5 always (this is the hallmark)
Think of it like:
The toilet flush is broken. No matter how much waste there is, nothing gets flushed. The waste (acid) stays in the house (blood).
What happens to K+?
- Normally, when H+ is pumped OUT into urine, K+ stays IN
- When H+ pump is broken, the body still tries to maintain electrochemical balance → K+ gets thrown out instead
- Result: Hypokalemia
What happens to bones and kidneys?
- Acidic blood → body borrows calcium from bones to neutralize acid → hypercalciuria
- Less citrate in urine (citrate is used up to buffer acid in cells) → hypocitraturia
- Alkaline urine + excess calcium + no citrate (citrate normally prevents stones) = STONES + NEPHROCALCINOSIS
Remember Type 1 as: Distal, Dump failure, pH always high (>5.5), hypoKalemia, Kidney stones
🟡 TYPE 2 RTA - "The HCO3- Collector is Broken"
Who broke down? = Workers at the proximal tubule (PCT)
Their job: Collect HCO3- (alkali/base) from the filtrate and return it to blood
What happens when they fail?
- HCO3- leaks into urine instead of going back to blood
- Blood loses alkali → blood becomes acidic
BUT here's the trick:
The collecting duct workers (Section C) are still perfectly fine. So when urine reaches them, they CAN acidify it.
Result: Urine pH is low (<5.5) at baseline because collecting duct still works
- BUT if you give alkali treatment (NaHCO3), so much HCO3- floods the tubule that even the collecting duct can't handle it → urine pH goes >5.5
Think of it like:
The bucket has a hole at the top (PCT). Water (HCO3-) keeps leaking before it reaches the tap. But the tap itself (collecting duct) works fine.
Why is it usually Fanconi syndrome?
- The PCT does EVERYTHING - glucose, amino acids, phosphate, HCO3- reabsorption
- If PCT workers go on strike (Fanconi), ALL of these are lost → glycosuria + aminoaciduria + phosphaturia + RTA
What happens to K+?
- Normally: mild hypokalemia (aldosterone goes up to compensate Na+ loss)
- With alkali treatment: K+ drops dramatically - extra HCO3- reaching distal tubule pulls K+ out with it
Remember Type 2 as: Proximal, PCT problem, pH variable (low at baseline, high with treatment), Fanconi, Phosphate loss (rickets), No stones
🟢 TYPE 4 RTA - "The Manager is Missing"
Who broke down? = Not the workers themselves, but the manager (Aldosterone)
Aldosterone normally tells collecting duct workers to:
- Absorb Na+
- Secrete K+
- Secrete H+
When aldosterone is absent or ignored:
- K+ stays in blood → Hyperkalemia
- H+ stays in blood → mild metabolic acidosis
- The workers (pumps) are physically fine but have no instructions
The twist about urine pH:
- The H+-ATPase pump is NOT broken - just under-stimulated
- So urine CAN be acidified → urine pH <5.5
- BUT the total amount of H+ excreted is low because hyperkalemia blocks ammonia (NH3) production - NH3 is the buffer that carries H+ out as NH4+
- Less buffer = less H+ can be excreted = acidosis
Think of it like:
The factory (collecting duct) is functional, but the manager (aldosterone) didn't show up. Workers are sitting idle. A little work happens (urine acidifies), but not enough to clear all the acid.
Most common cause: Diabetic nephropathy → damages juxtaglomerular apparatus → less renin → less angiotensin → less aldosterone = hyporeninemic hypoaldosteronism
Remember Type 4 as: hyperKalemia, Kidney (diabetic nephropathy), pH <5.5, mild acidosis, aldosterone problem
STEP 4: The ONE KEY DIFFERENCE Chart
Draw this in your mind:
TYPE 1 TYPE 2 TYPE 4
Problem: Distal pump Proximal Aldosterone
broken leaking missing
K+: LOW ↓ LOW ↓ HIGH ↑
Urine pH: ALWAYS >5.5 <5.5 baseline <5.5
>5.5 with Rx
Stones?: YES ✓ NO ✗ NO ✗
Fanconi?: NO ✗ YES ✓ NO ✗
STEP 5: The Urine pH Trick (Most Confusing Part - Simplified)
"Why is urine pH high in Type 1 but LOW in Type 4, even though both are RTAs?"
-
Type 1: The H+ pump (H+-ATPase) is physically broken → can't push H+ into urine → urine stays alkaline (>5.5)
-
Type 4: The H+ pump is fine, but the body has no buffer (NH3) to carry H+ out because hyperkalemia blocks ammonia production. So a little H+ goes in → urine is mildly acidic (<5.5) - but NOT ENOUGH to clear all the acid load from blood.
Simple version:
- Type 1 = pump broken → zero acid in urine → pH high
- Type 4 = pump works but bucket (NH3 buffer) is missing → little acid in urine → pH low, but still not enough
STEP 6: Drug Causes - Logic Based
| Drug | Type of RTA | Why? |
|---|---|---|
| Amphotericin B | Type 1 | Pokes holes in collecting duct membrane → H+ leaks back in |
| Topiramate / Acetazolamide | Type 1 & 2 | Blocks carbonic anhydrase → can't make H+ to secrete |
| Tenofovir / Ifosfamide | Type 2 | Damages PCT mitochondria → PCT stops working → Fanconi |
| ACE inhibitors / ARBs / Spironolactone / Amiloride | Type 4 | Reduce aldosterone effect |
| Heparin | Type 4 | Blocks aldosterone synthesis in adrenal gland |
STEP 7: Causes - One Word Association
Type 1 causes = think "Autoimmune + Ampho B"
- Sjögren syndrome (most common adult cause)
- Amphotericin B
- SLE, rheumatoid arthritis
- Hereditary (H+-ATPase gene mutations)
Type 2 causes = think "Cystinosis + Chemo drugs"
- Cystinosis (children - #1 genetic cause)
- Multiple myeloma (adults)
- Tenofovir, ifosfamide
- Wilson disease, galactosemia, fructose intolerance
Type 4 causes = think "Diabetes + Drugs that block aldosterone"
- Diabetic nephropathy (#1 cause)
- Addison's disease
- ACE inhibitors, ARBs, heparin, trimethoprim, spironolactone
STEP 8: The Final Anchor - One Story Per Type
Type 1: "A woman with dry mouth and dry eyes (Sjögren) keeps forming kidney stones. Her urine is always alkaline even though her blood is acidic. Her K+ is low."
→ Collecting duct H+ pump broken → can't dump acid → alkaline urine → stones
Type 2: "An HIV patient on Tenofovir has glucose in urine (but normal blood sugar), bone pain, and mild acidosis. K+ drops badly when given sodium bicarbonate."
→ PCT broken (Fanconi) → loses everything → HCO3- leaks → alkali makes hypokalemia worse
Type 4: "A diabetic on ACE inhibitor has high K+ and mild acidosis. Urine pH is 5.0."
→ No aldosterone → K+ high → blocks NH3 production → can't excrete enough H+ → mild acidosis, but urine pH still low
FINAL SUMMARY IN 3 LINES EACH
TYPE 1 (Distal): Collecting duct H+ pump is broken. Urine is always alkaline (>5.5). K+ is low. Causes nephrocalcinosis and stones. Caused by Sjögren, Ampho B.
TYPE 2 (Proximal): PCT leaks HCO3-. Usually Fanconi syndrome. Urine pH is low normally, rises with treatment. K+ drops badly with alkali. Caused by cystinosis (child), myeloma, tenofovir (adult).
TYPE 4 (Hyperkalemic): Aldosterone missing or ignored. K+ is HIGH (the key difference). Urine pH is low (<5.5) but acidosis persists because NH3 buffer is absent. Most common cause = diabetic nephropathy.
How i K+ related to HCI3 AND NH3
Great question - this is the core of understanding RTA deeply. Let me build this step by step with pure logic.
How K+ Links to HCO3- and NH3
First: Understand What the Kidney Is Trying to Do
The kidney has one acid-base goal:
Remove excess H+ (acid) from the body through urine
It does this in two ways:
- Keep HCO3- (alkali) - don't let it spill into urine
- Excrete H+ as NH4+ (using NH3 as a carrier)
K+ interferes with BOTH of these.
PART 1: K+ and HCO3- Relationship
The Basic Rule:
K+ and H+ compete to move in and out of cells
They are both positively charged ions and the body tries to keep electrical balance everywhere.
When K+ is LOW (Hypokalemia):
Blood K+ is low → body needs to get K+ from somewhere
→ K+ moves OUT of cells into blood
→ To maintain electrical neutrality inside the cell,
H+ moves IN to the cell (to replace K+)
→ Blood loses H+ → Blood becomes ALKALINE
→ But inside the KIDNEY tubule cells, H+ is now HIGH
→ More H+ inside tubule cells = more H+ pumped into urine
→ More HCO3- regenerated and sent to blood
→ Blood HCO3- goes UP
Result of Hypokalemia:
- Blood = alkalosis (high pH, high HCO3-)
- Urine = paradoxically acidic (more H+ being pumped out)
- This is called "paradoxical aciduria" - seen in hypokalemic alkalosis (e.g., vomiting)
When K+ is HIGH (Hyperkalemia):
Blood K+ is high → K+ moves INTO cells
→ To maintain electrical neutrality,
H+ moves OUT of cells into blood
→ Blood gains H+ → Blood becomes ACIDIC
→ Inside kidney tubule cells, H+ is now LOW
→ Less H+ available to pump into urine
→ Less HCO3- regenerated
→ Blood HCO3- goes DOWN
Result of Hyperkalemia:
- Blood = acidosis (low pH, low HCO3-)
- This is exactly what happens in Type 4 RTA
Simple Visual:
CELL BLOOD
High K+ in blood:
K+ ────────────→ enters cell
H+ ←──────────── exits cell → Blood becomes ACID
HCO3- falls
Low K+ in blood:
K+ ←──────────── exits cell
H+ ────────────→ enters cell → Blood becomes ALKALINE
HCO3- rises
One line rule: K+ and H+ always move in OPPOSITE directions across cell membranes.
PART 2: K+ and NH3 Relationship
First, What is NH3 and Why Does It Matter?
The kidney excretes most H+ not as free H+ (that would make urine dangerously acidic) but bound to ammonia (NH3):
NH3 + H+ → NH4+ (ammonium)
NH4+ is then excreted in urine. This is the main way the kidney gets rid of acid load.
~70% of daily acid excretion depends on NH3 production.
So if NH3 production drops → less H+ can be excreted → blood stays acidic.
Where Does NH3 Come From?
NH3 is made in proximal tubule cells from the amino acid glutamine:
Glutamine → (enzyme: glutaminase)
→ NH3 + HCO3- (both produced together)
- NH3 → goes into tubule lumen → picks up H+ → becomes NH4+ → excreted
- HCO3- → goes into blood → helps correct acidosis
This is brilliant: one reaction both removes acid (NH3 carries H+) AND generates alkali (HCO3- to blood).
Now: How Does High K+ Kill This System?
High K+ in blood
→ K+ enters cells (including PCT cells)
→ H+ exits cells into blood (K+/H+ exchange)
→ Inside PCT cells: H+ is now LOW
→ Low intracellular H+ = ALKALINE inside the cell
→ Alkaline environment SUPPRESSES glutaminase enzyme
→ Less glutamine is broken down
→ Less NH3 produced
→ Less NH4+ excreted in urine
→ Less H+ removed from body
→ Acidosis worsens
Reverse - Low K+ stimulates NH3:
Low K+ in blood
→ K+ exits cells
→ H+ enters cells (PCT becomes acidic inside)
→ Acidic intracellular environment STIMULATES glutaminase
→ More NH3 produced
→ More H+ excreted as NH4+
→ Acidosis corrected
Simple Visual:
HIGH K+ → cell interior becomes ALKALINE
→ glutaminase SUPPRESSED
→ less NH3
→ less H+ excreted
→ MORE ACIDOSIS ← despite urine pH being <5.5
LOW K+ → cell interior becomes ACIDIC
→ glutaminase STIMULATED
→ more NH3
→ more H+ excreted
→ CORRECTS ACIDOSIS
PART 3: Tying It All Together - Why Type 4 RTA Makes Sense Now
Diabetic nephropathy
→ Less RENIN
→ Less Angiotensin
→ Less ALDOSTERONE
→ Collecting duct: less Na+ absorption, less K+ secretion
→ K+ stays in blood = HYPERKALEMIA
Now two things happen simultaneously:
① K+ HIGH → H+ exits cells → blood acidosis (↓HCO3-)
② K+ HIGH → PCT cells become alkaline
→ glutaminase suppressed
→ less NH3 made
→ less NH4+ in urine
→ less H+ excreted
Both effects together → METABOLIC ACIDOSIS
And the confusing part - urine pH is still <5.5 because:
- The H+-ATPase pump in collecting duct is physically working
- It pumps whatever little H+ there is into urine
- But there's not enough NH3 buffer to carry the acid load
- So urine is "acidic" but total acid excretion is insufficient
Analogy: The toilet flushes normally (pH <5.5), but the sewer pipe is tiny (no NH3 buffer). You can flush small amounts, but a big load (normal acid production) won't clear.
PART 4: Why Hypokalemia in Type 1 and Type 2 RTA?
Type 1 RTA + Hypokalemia:
Multiple reasons:
Reason 1 - Electrochemical:
- H+ pump in collecting duct is broken → H+ cannot go into urine
- The lumen needs to be electrically balanced
- To maintain luminal negativity, K+ is secreted instead (via ROMK)
- H+ and K+ compete for secretion → less H+ secretion = more K+ secretion → K+ loss
Reason 2 - Aldosterone:
- Acidosis triggers aldosterone release
- Aldosterone increases K+ secretion in collecting duct → more K+ lost in urine
H+ pump broken → K+ secreted in its place → Hypokalemia
Type 2 RTA + Hypokalemia (and why alkali worsens it):
At baseline:
- PCT leaks HCO3- → Na+ follows (because Na+ is linked to HCO3- transport)
- Na+ delivery to distal tubule increases
- Aldosterone responds → more Na+ reabsorbed, more K+ secreted → mild hypokalemia
With NaHCO3 treatment:
- Even more HCO3- arrives at collecting duct
- HCO3- in the lumen creates a stronger negative charge
- This pulls K+ out MORE aggressively via ROMK
- K+ drops dramatically → this is why you MUST give K+ supplements with alkali in Type 2
FINAL SUMMARY TABLE
| Situation | K+ moves | H+ moves | Blood pH | HCO3- | NH3 production |
|---|---|---|---|---|---|
| Hyperkalemia | Into cells | Out of cells | Acidic ↓ | Low ↓ | Suppressed ↓ |
| Hypokalemia | Out of cells | Into cells | Alkaline ↑ | High ↑ | Stimulated ↑ |
| Type 4 RTA | High K+ | Out of cells | Acidic | Low | Suppressed (main mechanism) |
| Type 1 RTA | Low K+ | Pump broken | Acidic | Low | Normal/increased |
| Type 2 RTA | Low K+ | Leaks as HCO3- | Acidic | Low | Normal |
The 3 Rules to Remember Forever
Rule 1: K+ and H+ always move in opposite directions across membranes
Rule 2: High K+ → alkaline inside cells → suppresses NH3 (glutaminase) → less acid excreted
Rule 3: Low K+ → acidic inside cells → stimulates NH3 → more acid excreted
These 3 rules explain every acid-base + potassium interaction in the entire kidney.
This is a shared conversation. Sign in to Orris to start your own chat.