Infective endocarditis
Reading File
Finding Sources
Searching PubMed
"infective endocarditis"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive content from multiple authoritative textbooks. Let me compile the complete answer:
Infective Endocarditis (IE)
Definition
Infective endocarditis is a microbial infection (predominantly bacterial) of the endocardial surface of the heart - primarily the cardiac valves - leading to formation of vegetations composed of thrombotic debris, fibrin, inflammatory cells, and organisms, often with destruction of the underlying cardiac tissue. The aorta, aneurysmal sacs, prosthetic devices, and cardiovascular implantable electronic devices (CIEDs) can also be involved. - Robbins & Kumar Basic Pathology, p. 368
Classification
| Type | Features |
|---|---|
| Acute IE | Rapidly progressing, destructive infection; substantial morbidity/mortality even with therapy; typically caused by virulent organisms (e.g., S. aureus) on previously normal valves |
| Subacute IE | Insidious onset; protracted course of weeks to months; usually caused by less virulent organisms (e.g., viridans streptococci) on previously damaged valves; most patients recover with antibiotics |
Epidemiology
- US incidence: 10,000 to 20,000 new cases per year (~1 case per 1,000 hospital admissions) - Goldman-Cecil Medicine
- In developing countries: younger adults with rheumatic heart disease; viridans streptococci dominant; subacute course
- In developed countries/healthcare settings: S. aureus is now the most common cause overall, driven by healthcare exposure and the opioid epidemic (IV drug use)
- More than one valve is infected in ~20% of cases; some are polymicrobial - Goldman-Cecil Medicine
Pathogenesis
The sequence is predictable (from Goldman-Cecil and Robbins):
- Endothelial damage - turbulent flow from valve abnormalities, catheters, or pacemaker leads
- Sterile vegetation forms - platelet-fibrin thrombus (nonbacterial thrombotic endocarditis, NBTE) deposits at the damaged site
- Transient bacteremia seeds the vegetation
- Microbial proliferation - organisms reach 10⁹-10¹¹ CFU per gram of tissue; surface is avascular (difficult antibiotic penetration)
- Metastatic infection - septic emboli seed organs with high blood flow (kidneys, spleen, brain); mycotic aneurysms form from bacterial infection of arterial walls
Predisposing Conditions
More common:
- Mitral valve prolapse (especially with regurgitation) - now the leading preexistent risk factor in developed countries
- Degenerative valvular disease
- Injection drug use
- Prosthetic heart valves (account for 10-20% of all IE cases)
- Previous IE
- Congenital heart disease
Less common:
- Rheumatic heart disease (still important in developing countries)
- Bicuspid aortic valve, calcific valvular stenosis
- CIEDs (pacemakers, defibrillators, ventricular assist devices)
- Indwelling vascular catheters
Host risk factors: HIV infection, neutropenia, immunodeficiency, malignancy, diabetes, end-stage renal disease on hemodialysis, alcohol use - Goldman-Cecil Medicine, Robbins & Kumar
Microbiology
| Organism | Setting | Valve | Course |
|---|---|---|---|
| Viridans streptococci | Community-acquired; dental/oral procedures | Damaged valves | Subacute |
| S. aureus | Healthcare-associated; IV drug use | Normal or damaged | Acute |
| Enterococcus spp. | GI/GU procedures; elderly | Any | Variable |
| HACEK group (Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella) | Oral commensal flora | Any | Subacute |
| Fungi, gram-negative bacilli | Immunocompromised, IV drug users | Any | Aggressive |
| Culture-negative (~10%) | Prior antibiotics, fastidious organisms | - | - |
Morphology (Pathology)
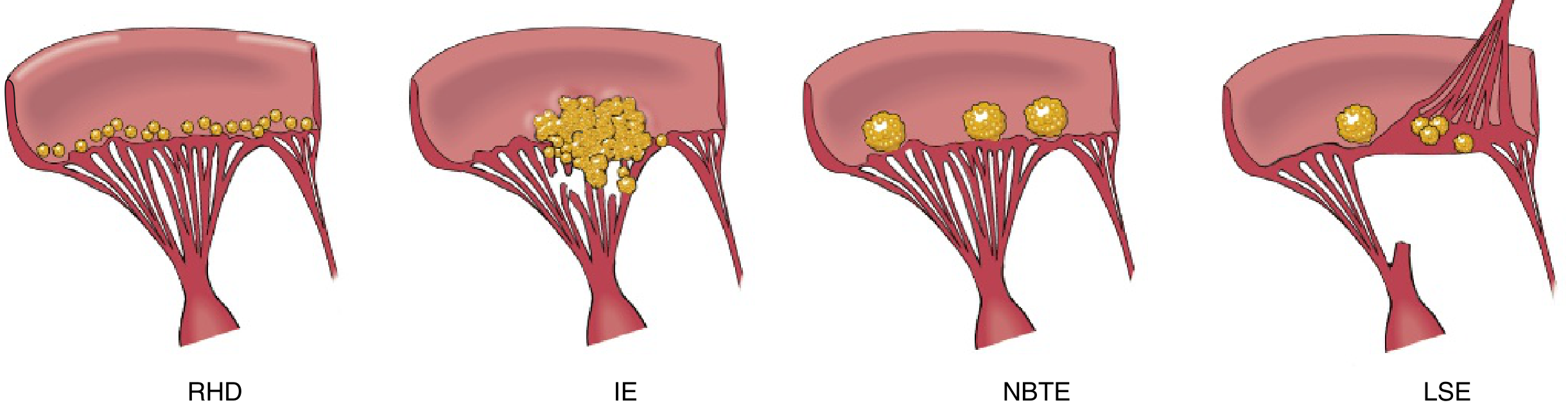
Diagram comparing vegetations in Rheumatic Heart Disease (RHD - small, beaded along line of closure), Infective Endocarditis (IE - large, bulky, destructive), Nonbacterial Thrombotic Endocarditis (NBTE - small, sterile), and Libman-Sacks Endocarditis (LSE - on both surfaces of valve).
- IE vegetations: friable, bulky, potentially destructive; contain fibrin, inflammatory cells, and organisms
- Aortic and mitral valves most commonly affected; tricuspid valve frequently targeted in IV drug users
- Can erode into myocardium to produce a ring abscess
- Shedding of emboli is common, leading to septic infarcts at distant sites - Robbins & Kumar Basic Pathology, p. 368-369
Clinical Features
Symptoms:
- Fever - the most consistent sign (absent in subacute IE in elderly)
- Chills, night sweats, fatigue, weight loss, malaise
- Myalgias, arthralgias, back pain
Signs of IE (the classic peripheral stigmata):
| Sign | Description |
|---|---|
| Osler nodes | Painful, raised erythematous nodules on fingertips/toes (immune complex-mediated) |
| Janeway lesions | Painless, flat erythematous lesions on palm or sole (embolic, septic) |
| Roth spots | Retinal hemorrhages with pale centers |
| Splinter hemorrhages | Linear dark streaks under nails |
| Petechiae | Conjunctival or mucosal |
| New or changing murmur | Present in 90% with left-sided lesions |
| Splenomegaly | Common in subacute IE |
Complications:
- Glomerulonephritis (immune complex trapping) - hematuria, albuminuria, renal failure
- Systemic embolization - stroke, splenic/renal infarcts, cerebral abscess
- Septicemia, arrhythmias (extension to conduction system), ring abscess
- Mycotic aneurysms
- Acute heart failure from valve destruction - Robbins & Kumar
Diagnosis: Duke Criteria
Diagnosis requires satisfaction of modified Duke criteria (2000 modification; updated to 2023 Duke-ISCVID criteria):
Major Criteria
1. Microbiological Evidence:
- Typical organism (viridans streptococci, S. aureus, S. bovis, HACEK, enterococci) from 2 separate blood cultures
- Persistently positive blood cultures drawn >12 hours apart
- Single positive culture for Coxiella burnetii
2. Evidence of Endocardial Involvement (Echocardiographic):
- Oscillating intracardiac mass on valve/supporting structure or regurgitant jet path
- Abscess
- New partial dehiscence of a prosthetic valve
- New valvular regurgitation
3. Imaging (2023 update):
- CT evidence of vegetation, abscess, or valve perforation
- ¹⁸F-FDG PET/CT showing abnormal metabolic activity (≥3 months after prosthetic valve implantation)
- Nuclear medicine SPECT/CT
4. Surgical Major Criterion (2023 update):
- Direct inspection during cardiac surgery confirming IE (in absence of other major criteria)
Minor Criteria (Modified Duke)
- Predisposing heart condition or IV drug use
- Fever ≥38°C (100.4°F)
- Vascular phenomena: arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial/conjunctival hemorrhage, Janeway lesions
- Immunologic phenomena: glomerulonephritis, Osler nodes, Roth spots, positive rheumatoid factor
- Microbiologic evidence: positive blood culture not meeting major criteria
Classification
| Class | Criteria |
|---|---|
| Definite IE | 2 major, OR 1 major + 3 minor, OR 5 minor (clinical); OR pathologic criteria (organism on culture/histology of vegetation) |
| Possible IE | 1 major + 1 minor, OR 3 minor |
| Rejected | Firm alternative diagnosis, OR resolution with ≤4 days of antibiotics |
- Washington Manual of Medical Therapeutics, Textbook of Clinical Echocardiography (2023 Duke Criteria)
Investigations
- Blood cultures: 3 sets from different sites before starting antibiotics; most important test
- Echocardiography:
- TTE (transthoracic): First line; sensitivity ~60-70% for vegetations
- TEE (transesophageal): Superior sensitivity (~90-95%); mandatory when TTE negative but high suspicion, prosthetic valve involved, or staphylococcal bacteremia
- CBC: anemia (normochromic normocytic), leukocytosis
- ESR, CRP: elevated
- Urinalysis: hematuria, proteinuria (immune complex nephritis)
- RF, ANA: positive in subacute IE (immune complex formation)
- CT scan: evaluate for embolic complications (brain, spleen, kidneys)
- ¹⁸F-FDG PET/CT: particularly useful for prosthetic valve IE and device infections
Management
A. General Principles
Every patient with IE should be managed in an inpatient setting at a medical center with an IE team - infectious disease, cardiology, and cardiac surgery specialists. This multidisciplinary approach has improved outcomes. - Braunwald's Heart Disease
B. Antibiotic Therapy
Empiric therapy before culture results: cover S. aureus and streptococci
| Organism | Preferred Regimen |
|---|---|
| Viridans streptococci (penicillin-susceptible) | Penicillin G or ceftriaxone × 4 weeks |
| S. aureus (MSSA) | Nafcillin or oxacillin × 6 weeks |
| S. aureus (MRSA) | Vancomycin × 6 weeks |
| Enterococcus (ampicillin-susceptible) | Ampicillin + aminoglycoside or ampicillin + ceftriaxone × 4-6 weeks |
| Enterococcus (ampicillin-resistant, vanco-susceptible) | Vancomycin + aminoglycoside |
| Prosthetic valve (staph) | Vancomycin + rifampin + gentamicin |
- Bactericidal agents at high doses are required
- IV therapy for most IE (oral step-down permitted in selected stable cases per recent evidence)
- Duration: typically 4-6 weeks for native valve; longer for prosthetic valve - Katzung's Pharmacology, Goldman-Cecil Medicine
C. Surgical Indications (Valve Surgery)
Surgery is indicated for:
Class I (emergent/urgent):
- Acute heart failure from valve dysfunction (most common indication - emergent)
- Persistent bacteremia or fever >5-7 days despite appropriate antibiotics
- Abscess (ring/perivalvular), fistula, or heart block
- Infection due to resistant organisms (fungi, Brucella, MRSA on prosthetic valve)
- Large vegetations with embolic events despite antibiotics
Other indications:
- Relapsing prosthetic valve endocarditis
- Large vegetations (>10 mm) especially with high embolic risk
- Prosthetic valve IE (more frequently requires surgery than native valve) - Braunwald's Heart Disease, Washington Manual
D. Complications of Neurologic IE
- Embolic stroke is the most devastating complication
- Neurologic abnormalities usually resolve with appropriate antibiotic therapy
- Timing of cardiac surgery after stroke is debated - generally delayed ≥4 weeks after hemorrhagic stroke - Bradley and Daroff's Neurology
Prevention (Antibiotic Prophylaxis)
The 2021 AHA Scientific Statement updated prophylaxis guidelines:
Who requires prophylaxis before invasive dental procedures:
- Prosthetic cardiac valve (including transcatheter-implanted)
- Previous IE
- Unrepaired cyanotic congenital heart disease
- Surgically repaired CHD with residual defects
- Cardiac transplant recipients with valvulopathy
- Ventricular assist devices and implantable hearts (added in 2021)
Preferred regimen:
- Amoxicillin 2 g orally, 30-60 min before procedure (penicillin allergy screening now recommended; 90% will be skin-test negative)
- Doxycycline added as alternative in truly penicillin-allergic patients (clindamycin removed due to C. difficile risk)
Key principle: Maintaining good oral health is emphasized; routine daily activities may cause VGS bacteremia that prophylaxis cannot fully prevent. - Braunwald's Heart Disease
Prognosis
- Without treatment: IE is uniformly fatal
- With appropriate antibiotics ± surgery: in-hospital mortality ~15-30% (varies by organism and complications)
- S. aureus IE has the worst prognosis; viridans streptococcal IE has a more favorable outcome
- Adverse prognostic factors: S. aureus infection, heart failure, systemic embolization, perivalvular abscess, prosthetic valve involvement, renal failure
Sources: Robbins & Kumar Basic Pathology; Braunwald's Heart Disease, 12th Ed.; Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine, 22E (2025); Washington Manual of Medical Therapeutics; Textbook of Clinical Echocardiography (2023 Duke Criteria); Katzung's Basic and Clinical Pharmacology, 16th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.