Pedogogy on stab injuries, md FMT practical’s , get me all the data , biomechanics and mechanism , FMT related aspects , healing , shapes of stabs and type of weapons that cause different patterns. Add a note on grievous hurt and BNSS
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching the Web
BNSS Bharatiya Nyaya Sanhita grievous hurt section stab wound forensic medicine 2023
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive data from multiple authoritative sources. Let me compile the complete pedagogical response.
Stab Injuries - Complete FMT Pedagogy
Sources Used
- DiMaio's Forensic Pathology, 3rd Ed (DiMaio)
- P.C. Dikshit Textbook of Forensic Medicine and Toxicology (Dikshit)
- Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology (Parikh)
- Schwartz's Principles of Surgery, 11th Ed
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
1. DEFINITION AND CLASSIFICATION
A stab wound (synonyms: puncture wound, punctured-incised wound) is one where the depth exceeds the surface dimensions. This distinguishes it from an incised wound where length at the surface exceeds depth.
Sharp force injuries are broadly classified as:
- Incised wounds (cuts/slash - length > depth)
- Stab/puncture wounds (depth > length)
- Chop wounds (heavy sharp weapons, e.g., axe)
2. BIOMECHANICS AND MECHANISM
Force Required to Penetrate Skin
The force needed depends on the configuration and sharpness of the tip. The sharper and more needle-like the tip, the more readily it will perforate the skin. Once the tip perforates the skin, the rest of the blade slides into the body with very little additional force - even through viscera, as long as bone is not contacted.
Key biomechanical principle: Even if a knife is driven its complete length into the body, this does not necessarily mean the stab was inflicted with great force.
Factors Affecting Depth and Force Required (Dikshit)
- Nature of weapon - A sharp, slender weapon passes more easily; a blunt-pointed weapon requires more force
- Part of the body stabbed - Soft areas like the anterior abdominal wall are easily pierced; areas with underlying bone (skull) resist penetration
- Age and build of the victim - Healthy muscular adults are less susceptible to deep penetration; children with softer skin sustain deeper injuries with less force
Skin-to-Organ Distances (DiMaio, Connor et al. CT study)
These represent minimum distances a knife must penetrate to reach vital structures. In real life they may be shorter because the abdominal/chest wall can be compressed by the thrust.
| Organ | Minimum (mm) | Mean (mm) | Maximum (mm) |
|---|---|---|---|
| Pleura | 10 | 22 | 48 |
| Pericardium | 15 | 31 | 45 |
| Liver | 9 | 19 | 36 |
| Spleen | 12 | 23 | 39 |
| Kidney | 19 | 37 | 79 |
| Thoracic Aorta | 31 | 64 | 93 |
| Abdominal Aorta | 65 | 87 | 102 |
| Femoral Artery | 13 | 18 | 25 |
DiMaio's Forensic Pathology, 3rd Ed, p. 184
3. CHARACTERISTICS OF STAB WOUNDS - FMT PRACTICAL EXAMINATION
From examining a stab wound, the forensic expert can determine:
- Dimensions of the weapon
- Type of weapon
- Taper of the blade
- Movement of knife within the wound
- Depth of thrust
- Direction of thrust
- Amount of force used
(Dikshit, p. 183)
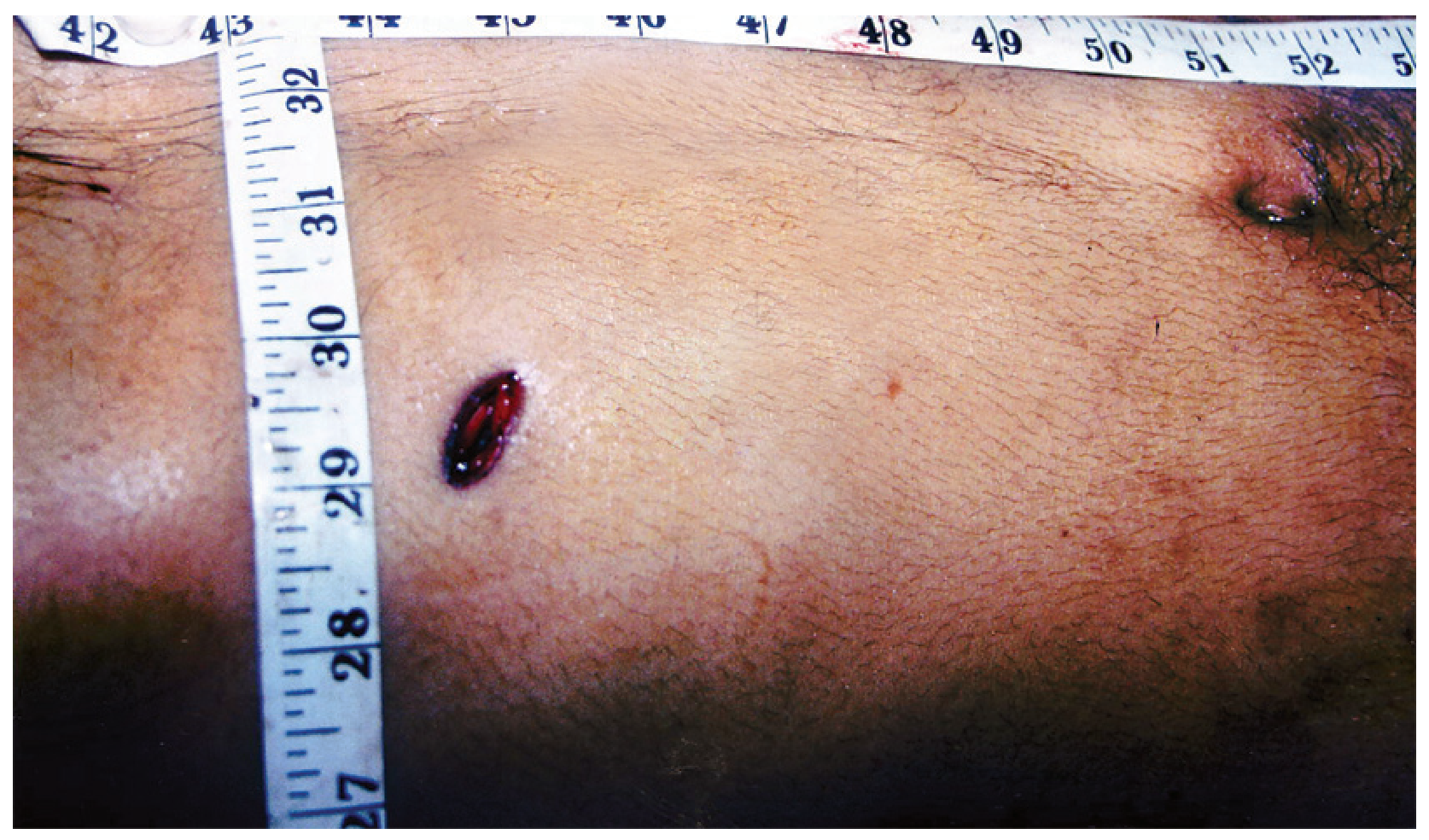
3a. LENGTH
- Length of the wound is usually slightly less than the width of the weapon due to the elasticity of skin
- In most instances, the wound will have gaped across the centre forming a long ellipse
- Extent of gaping depends on anatomical location (over joints, axilla, groin), and whether the axis crosses Langer's lines
- After a stab, edges must be manually apposed to record the true dimension - this is a critical medicolegal step
- The wound appears considerably longer once edges are approximated
- Length is more if lateral movement of the weapon or body occurs
3b. BREADTH
The second dimension on the surface; the width at widest point.
3c. DEPTH
- Depth is the greatest dimension - the length of the wound track
- Equal to or less than the length of the blade
- May exceed blade length if the knife is plunged with sufficient force to indent the abdominal/chest wall
- Do NOT probe a stab wound in a living patient with a metal probe - risk of dislodging clots and causing hemorrhage. Use a pliant rubber tube or radiopaque dye injection followed by X-ray
3d. MARGINS
- Sharp and clean with a sharp weapon
- Irregular and abraded with a blunt-pointed weapon (screwdriver, broken glass)
- A hilt mark (technically "guard mark") may be seen at the angles of the wound if the full length of the blade entered
3e. ANGLES (Corners) - Most Important FMT Practical Point
| Finding | Inference |
|---|---|
| Both angles acute (pointed) | Double-edged weapon (dagger, stiletto) |
| One acute, one squared/blunted | Single-edged weapon (kitchen knife) |
| One acute, one slightly forked | Single-edged knife; fork = cutting edge slicing skin on withdrawal |
Note: Single-edged knives can occasionally produce bilateral pointed ends because (1) the cutting edge slices skin as the tip perforates; (2) the knife is twisted on withdrawal.
4. SHAPES OF STAB WOUNDS AND LANGER'S LINES
This is the most important concept for practical exams.
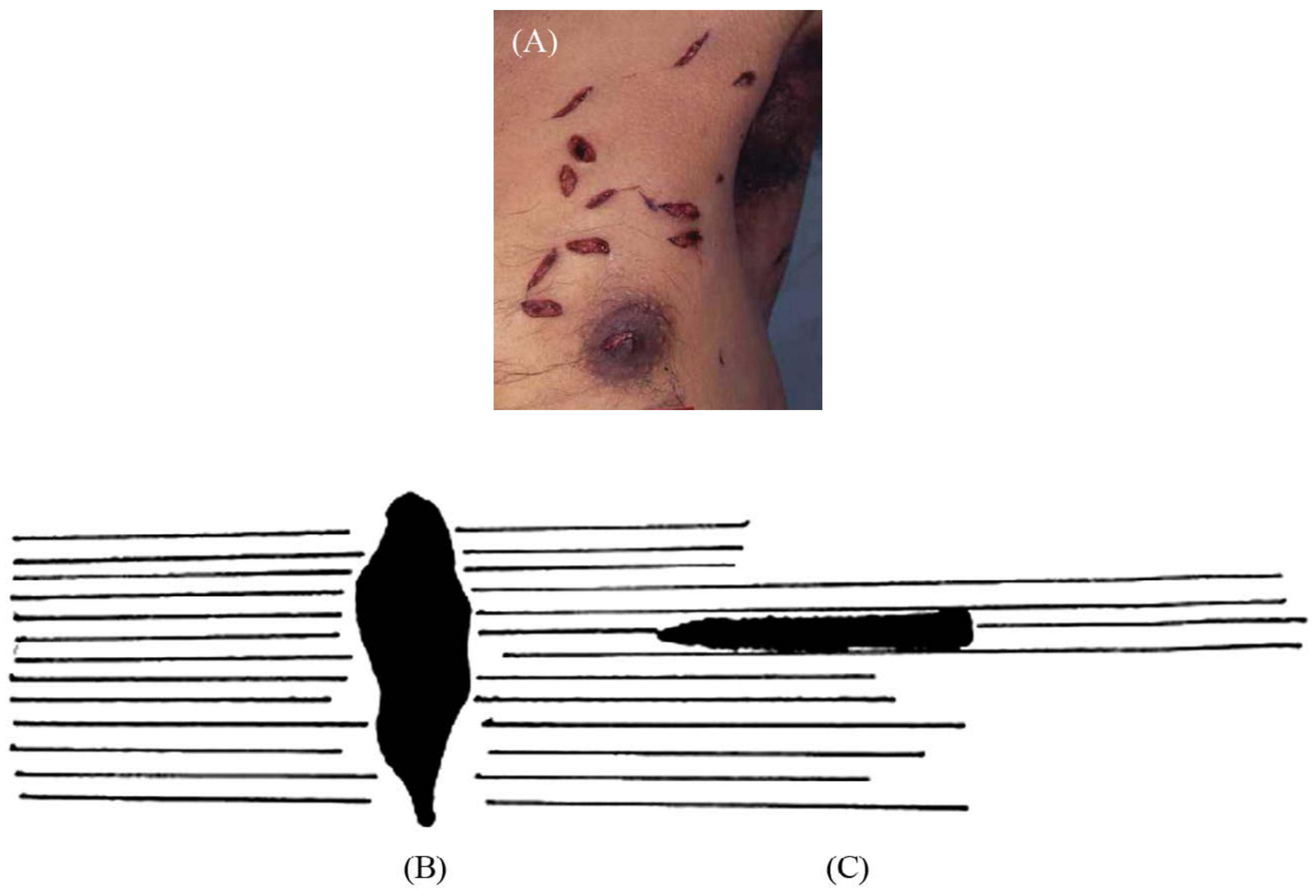
Figure: Effect of Langer's lines on stab wound shape - DiMaio's Forensic Pathology, 3rd Ed, p.185
Langer's Lines (Cleavage Lines) and Wound Shape
| Orientation of Stab Relative to Langer's Lines | Wound Shape |
|---|---|
| Perpendicular (across the lines) | Wide, oval/elliptical, gaping wound |
| Parallel (along the lines) | Narrow, slit-like wound |
| Oblique | Asymmetrical or semicircular |
Practical importance: A slit-like wound may look smaller than the knife blade. Always appose the edges to get the true dimension.

Figure: Classic single-edged knife stab wound - squared top, V-shaped lower end. DiMaio, p.183
Shape is Also Influenced By:
- State of skin tension/relaxation at time of stabbing
- Movement of the blade or the victim
- Whether the flat surface of the blade entered obliquely (beveled margin on one side, undermining on the other)
- Depth of insertion (whether guard/ricasso contacted skin)
5. TYPES OF WEAPONS AND WOUND PATTERNS
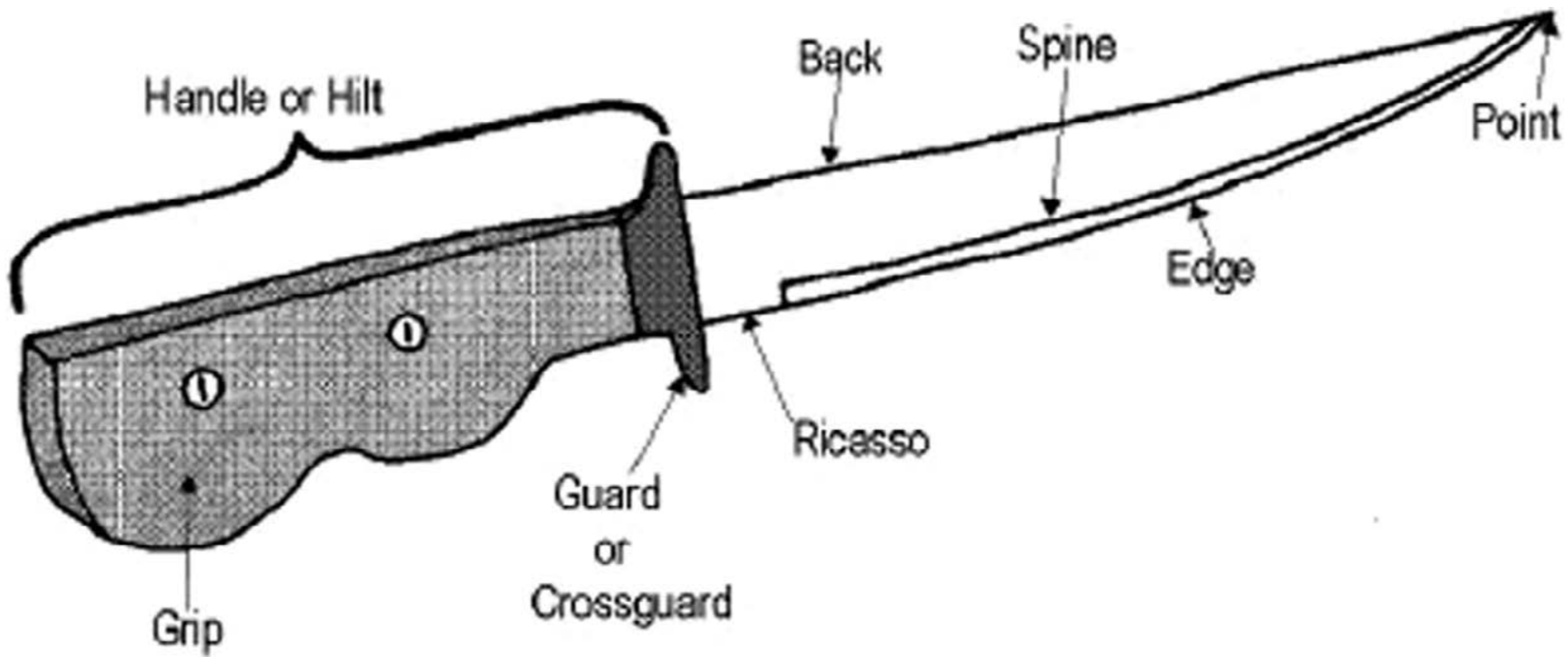
Figure: Anatomy of a single-edged knife - DiMaio, p.185
A. Single-Edged Knife (Kitchen/Pocket/Folding Knife)
- Most common weapon; typical blade 4-5 inches
- Wound: one acute angle, one squared/blunted angle
- If blade inserted up to ricasso: wound can be squared at both ends
- If guard (crossguard) contacts skin: patterned guard abrasion visible around the wound entry
- Symmetrical = knife driven straight in
- Prominent above wound = knife angled downward at entry
B. Double-Edged Weapon (Dagger, Stiletto, Bayonet)
- Wound: both angles acute/pointed
- Hilt mark may be seen if blade driven to full length
- Parikh case illustration: double-edged wound with prominent hilt mark
C. Ice Pick / Awl / Stiletto
- Small, inconspicuous circular or oval puncture
- May resemble insect bites or small lacerations
- Can be easily missed at autopsy - require careful examination
D. Scissors
- Closed scissors: Linear stab wound with abraded margins (tip splits rather than cuts)
- If screw protrudes, may produce an angular laceration in mid-portion of one skin margin
- Open scissors (blades separated): Produce two parallel stab wounds per thrust
E. Screwdriver (Flat-Head)
- Produces a linear or slightly angular wound
F. Phillips Screwdriver
- X-shaped point produces a circular or cruciform wound - highly characteristic
G. Fork
- Barbecue fork: Multiple penetrating wounds corresponding to number of prongs
- Kitchen fork: Superficial, small parallel punctures
H. Broken Glass / Porcelain
- Cutting ability can equal or exceed a surgical scalpel
- Produces incised or stab wounds depending on mechanism
- Margins may be irregular depending on nature of glass
I. Pen / Pencil / Unconventional Objects
- Can penetrate deeply into soft tissue and vital structures
- DiMaio case: ballpoint pen perforated the skin, muscle, and ligaments, penetrated the atlanto-occipital junction and perforated the spinal cord
Summary Table: Weapon vs. Wound Pattern
| Weapon | Shape | Margins | Key Feature |
|---|---|---|---|
| Single-edged knife | Slit/ellipse, one acute/one blunt end | Sharp and clean | Guard abrasion if full force |
| Double-edged knife/dagger | Both ends acute | Sharp and clean | Hilt mark |
| Ice pick | Small round/oval | Sharp | Often inconspicuous |
| Phillips screwdriver | Cruciform/circular | Abraded | X-pattern |
| Scissors (closed) | Linear | Abraded margins | Mid-margin laceration if screw protrudes |
| Fork | Multiple parallel punctures | Variable | Corresponds to prong number |
| Broken glass | Variable incised/stab | May be irregular | No pattern |
6. WOUND TRACK AND DIRECTION
From a careful examination, one can determine:
- Nature of weapon
- Approximate dimensions
- Thrusting force (from depth)
- Position of assailant and victim at time of assault
- Whether suicidal, homicidal, or accidental
Key points on wound track:
- Track is evenly cut with no tissue bridging (unlike lacerated wounds)
- Direction of track gives information about relative positions
- Track should not be probed with a metallic probe in the living - use pliant rubber tube or contrast X-ray
- Wound of exit (if present): smaller, with everted edges when a tapering weapon is used
Suicidal vs. Homicidal Stab Wounds
| Feature | Suicidal | Homicidal |
|---|---|---|
| Location | Over heart (left chest) | Abdomen, trunk, limbs, back |
| Number | Usually single or few | Often multiple |
| Hesitation wounds | Present (multiple superficial, tentative) | Absent |
| Defence wounds | Absent | Present (hands, forearms) |
| Clothes | May be lifted or parted | May be cut through |
| Accessibility | Site accessible to victim | Any site, including back |
| Area | Exposed skin (clothes removed) | Through clothing |
Back stab wounds are almost always homicidal (Parikh).
Harakiri (Japanese ritual suicide): Single large stab wound to abdomen with a short sword, resulting in evisceration and sudden fall in intra-abdominal pressure, collapse, and death.
7. WOUND HEALING - PHASES
Understanding wound healing is important both clinically and medico-legally (for estimating age of injury).
(Roberts & Hedges; Schwartz's Principles of Surgery)
Phase 1: Hemostasis (Immediate - Hours)
- Platelet degranulation, clot formation
- Release of PDGF, TGF-β, VEGF
- Vasoconstriction via sympathetic and cytokine pathways
- Sets the stage for inflammation
Phase 2: Inflammation (Days 1-5)
- PMNs (neutrophils) arrive first (24-48 hrs)
- Macrophages dominate by day 3-5 - coordinate debridement and growth factor release
- Histamine, prostaglandins increase capillary permeability
- Keratinocytes begin migration across wound surface within 24-48 hours (re-epithelialization)
- Surface becomes impermeable to water within 24-48 hours in sutured wounds
Phase 3: Proliferation / Fibroplasia (Days 4-21)
- By day 4-5: fibroblasts begin synthesizing collagen (predominantly Type III initially, then Type I)
- Significant tensile strength gain begins around day 5
- Tensile strength increases rapidly for days 6-17, more slowly for a further 10-14 days
- Granulation tissue forms; angiogenesis occurs
Phase 4: Remodeling / Resolution (Weeks to Months - up to 1 year)
- Type III collagen replaced by Type I
- Scar tissue remodels and strengthens for up to 1 year
- Maximum scar strength = ~80% of original unwounded skin - never fully restored
- Collagen formation essentially complete in 21-28 days but scar widens for another month
Healing by Intention
- First intention (primary): Wound edges approximated (sutured) within 24 hours; heals with minimal scar
- Second intention (secondary): Open wound; heals by contraction, collagen formation, and epithelialization; more scar tissue
Age Estimation of Wound (FMT relevance)
| Wound Age | Appearance |
|---|---|
| Fresh (0-6 hrs) | Bleeding, edges gaping, red |
| 6-24 hrs | Inflammatory swelling, edges begin to stick |
| 24-48 hrs | Scab forms, early epithelialization |
| 3-5 days | Granulation tissue visible, swelling reducing |
| 7-10 days | Fibroplasia, scar forming |
| >3 weeks | Remodeling, pale scar |
8. WRITING A STAB WOUND - PRACTICAL REPORT FORMAT
Based on Parikh's examples:
Example: Stab wound of the thorax (entry wound)
The entry wound is a punctured-incised wound, elliptical in shape. It is located in the left upper thorax above and lateral to the nipple, 15 inches below the top of the head, and 7 inches to the left of the midline. It is 1 inch long (1.25 inches when the edges are apposed) and 1/4 inch wide at the skin surface. It is horizontally oriented. The lateral corner is blunted and the medial corner is acutely angulated. There is no abrasion or bruising at the wound margin. The track is 5 inches deep, evenly cut, directed from left to right, front to back, and angulated slightly downward. No tissue bridging is noted. The track perforates the chest wall through the third intercostal space, perforates the lingula of the upper lobe of the left lung, the pericardial sac, and penetrates the heart perforating the left ventricular wall. The entire wound track is infiltrated with blood and 1000 ml of liquid and clotted blood is found in the left chest cavity. There is no exit wound.
(Parikh's Textbook, p.261)
9. KEY FMT PRACTICAL EXAM POINTS (MCQ/Short Answers)
| Question | Answer |
|---|---|
| Depth vs. length relationship in stab wound | Depth > surface length |
| One acute + one blunt end | Single-edged weapon |
| Both ends acute | Double-edged weapon |
| Wound smaller than blade width | Elasticity of skin retracts wound after withdrawal |
| Langer's lines parallel to wound | Slit-like, narrow |
| Langer's lines perpendicular to wound | Gaping, oval |
| Hilt/guard mark at wound | Blade driven to full length |
| Forking at one end | Cutting edge of knife slicing on withdrawal |
| Phillips screwdriver wound | Cruciform/circular |
| Scissors (closed) wound | Linear with abraded margins |
| Wounds on back | Almost always homicidal |
| Hesitation wounds | Suicidal |
| Defence wounds | Homicidal |
| Probing stab wound in living patient | Contraindicated - use pliant tube or contrast X-ray |
| Maximum scar tensile strength | ~80% of original skin |
10. NOTE ON GRIEVOUS HURT: IPC Section 320 and BNS Section 116
Under IPC Section 320 (now replaced by BNS Section 116)
The Bharatiya Nyaya Sanhita 2023 (BNS) replaces the Indian Penal Code, 1860. Section 116 of the BNS corresponds to Section 320 IPC and defines grievous hurt in identical spirit - the same 8 categories.
The 8 kinds of Grievous Hurt (BNS S.116 = IPC S.320):
-
Emasculation - Loss of masculine power due to direct trauma to genitalia or indirect (lumbosacral trauma); applicable only to males; both testes must be affected
-
Permanent privation of sight of either eye - Corneal scarring, retinal detachment, any permanent visual impairment of either eye
-
Permanent privation of hearing of either ear - Rupture of tympanic membrane causing even partial permanent hearing loss in either ear
-
Privation of any member or joint - Loss of function or anatomical separation of any body part capable of performing a distinct function
-
Destruction or permanent impairing of power of any member or joint - Permanent functional loss of any joint or organ; injury must be permanent
-
Permanent disfiguration of head or face - Context-dependent: a small scar on a young woman's face may qualify; a large scar on an elderly man's face may not. The impact on the person matters.
-
Fracture or dislocation of a bone or tooth - All fractures including hairline fractures, even outer table of skull fractures; even tooth dislocation qualifies
-
Any hurt that endangers life, or causes severe bodily pain or inability to follow ordinary pursuits for 20 days - "Ordinary pursuits" = daily activities (eating, bathing, toileting); inability to go to office alone for >20 days is not sufficient; the attending physician must evaluate nature/site of injury, treatment, and presence of infection
BNS vs. IPC - Key Changes Relevant to FMT
| Aspect | IPC (1860) | BNS (2023) |
|---|---|---|
| Grievous Hurt | Section 320 | Section 116 |
| Voluntarily causing grievous hurt | Section 325 | Section 117(2) |
| Dangerous weapons/means | Section 326 | Section 118(2) |
| Procedural law | CrPC | BNSS (Bharatiya Nagarik Suraksha Sanhita) |
Note for FMT practitioners: The substantive definition of grievous hurt is unchanged between IPC and BNS. The section numbers have changed. The BNSS governs criminal procedure; the BNS governs substantive criminal law. In injury reports and court testimony, cite BNS Section 116 (not IPC 320) for cases arising after July 1, 2024 (when the new acts came into force).
FMT Relevance of Grievous Hurt in Stab Injuries
A stab wound can constitute grievous hurt under one or more categories:
- Category 7 if it causes a bone fracture (e.g., stab wound with rib fracture)
- Category 8 if it endangers life (pneumothorax, hemopericardium, organ perforation) or causes severe pain/disability for >20 days
- Category 4/5 if it results in permanent loss of function (e.g., nerve injury, tendon severance)
The medical officer must opine specifically which clause of Section 116 BNS applies in the injury report.
Sources: DiMaio's Forensic Pathology 3rd Ed, p.183-191 | P.C. Dikshit FMT, p.183-186 | Parikh's Textbook of Medical Jurisprudence FMT, p.261-262 | Schwartz's Principles of Surgery 11th Ed, p.1999 | Roberts & Hedges Clinical Procedures in Emergency Medicine, p.739 | BNS 2023 Section 116, UP Police BNS-IPC Comparative Table
Refer krogman and tell me important aspects discussed for forensic anthropology and anthropometry
Finding Sources
Finding Sources
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
Generate a comprehensive PDF guide on Krogman's forensic anthropology methods
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.