What are ovarian and uterine changes during menstrual cycle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Ovarian and Uterine Changes During the Menstrual Cycle
The menstrual cycle averages 28 days and is divided into phases that reflect coordinated changes in the ovary and uterus, driven by the hypothalamus-pituitary-gonadal axis. The diagram below shows the relationship between these changes:
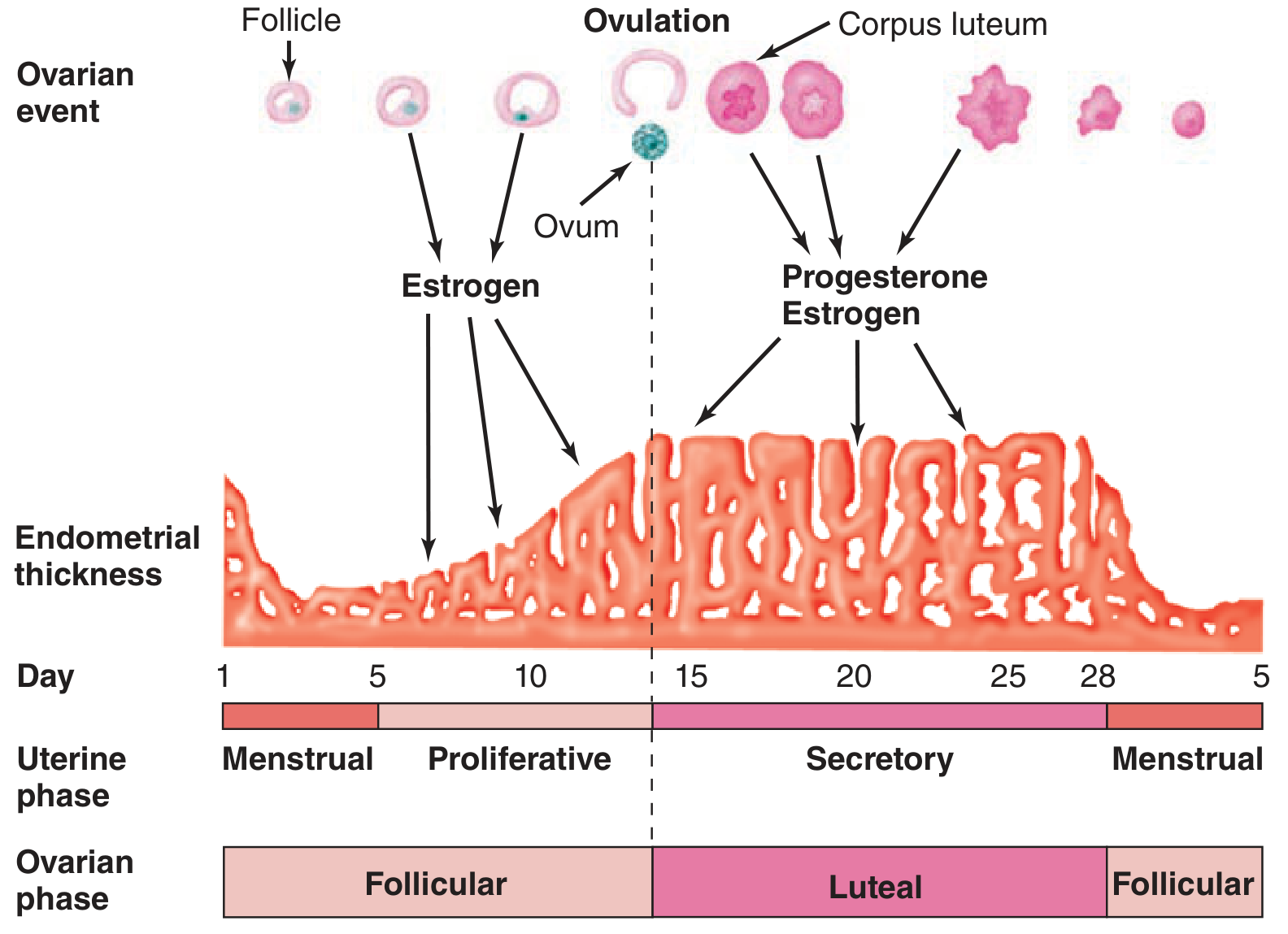
I. Ovarian Changes
1. Follicular Phase (Days 1-14)
At the start of each cycle, FSH from the anterior pituitary stimulates several primordial follicles to enlarge and develop an antrum (fluid-filled cavity). By around day 6, one follicle in one ovary becomes the dominant (Graafian) follicle and grows rapidly; the others undergo atresia (apoptosis).
- The theca interna cells of the follicle secrete androgens, which are then aromatized to estrogen (17β-estradiol) by the granulosa cells - this is the primary source of circulating estrogen.
- Rising estradiol levels exert positive feedback on the pituitary, triggering the LH surge (around day 13-14).
2. Ovulation (Day ~14)
The distended follicle ruptures in response to the LH surge, releasing the ovum into the abdominal cavity. The ovum is picked up by the fimbriated ends of the uterine tube. Minor bleeding from the follicle may cause peritoneal irritation known as mittelschmerz (mid-cycle pain).
3. Luteal Phase (Days 14-28)
After rupture, the follicle promptly fills with blood (corpus hemorrhagicum). The granulosa and theca cells then proliferate, replacing the clot with yellowish lipid-rich cells to form the corpus luteum.
- The corpus luteum secretes both estrogen and progesterone.
- Its growth depends on an adequate blood supply - VEGF is essential for this vascularization.
- If pregnancy does not occur, the corpus luteum regresses (luteolysis) by day 26-28, and progesterone/estrogen levels fall sharply, triggering menstruation.
- If pregnancy occurs, hCG from the trophoblast maintains the corpus luteum, which persists until the placenta takes over steroidogenesis.
II. Uterine (Endometrial) Changes
The endometrium has two functional layers:
- Stratum functionale - the superficial two-thirds, shed during menstruation; supplied by long, coiled spiral arteries
- Stratum basale - the deep layer, never shed; supplied by short, straight basilar arteries; source of endometrial regeneration
1. Menstrual Phase (Days 1-4)
When the corpus luteum regresses, estrogen and progesterone are withdrawn. This causes:
- Spiral artery vasospasm and endometrial ischemia
- Breakdown of lysosomes with release of proteolytic enzymes
- Prostaglandin F2α (PGF2α) plays a key role - it is a potent vasoconstrictor that amplifies vasospasm and stimulates myometrial contractions to expel sloughing tissue
- The stratum functionale is shed as menstrual flow; menstrual blood is ~75% arterial, contains fibrinolysin (which prevents clotting under normal flow) and tissue debris
2. Proliferative Phase (Days 5-14) - "Follicular" / "Pre-ovulatory" Phase
Under the influence of rising estradiol from the developing follicle:
- The endometrium thickens rapidly from day 5 to day 14
- Uterine glands elongate but do not yet secrete
- The stroma and spiral arteries grow
- Cervical mucus becomes copious, watery, elastic - when spread on a slide it produces a characteristic "ferning" pattern, and channels form that allow sperm penetration
3. Secretory Phase (Days 15-28) - "Luteal" Phase
Under the combined influence of progesterone + estrogen from the corpus luteum:
- Proliferation slows; the endometrium becomes highly vascularized and slightly edematous
- Uterine glands become coiled, tortuous, and accumulate glycogen in subnuclear vacuoles (visible by PAS staining); by days 19-20 they secrete fluid into the lumen
- Spiral arteries continue to elongate and coil
- Stromal edema develops progressively
- By around day 22-24, stromal cells develop an eosinophilic pattern resembling decidua (pseudodecidual change)
- Secretory activity is maximal around postovulatory days 6-7, exactly when a fertilized blastocyst would arrive for implantation
- Cervical mucus becomes thick, non-elastic, and scanty - and no longer "ferns" on a slide (sperm cannot penetrate)
- ~2 days before menses, a wave of polymorphonuclear leukocytes infiltrates the stroma, heralding breakdown
Summary Table
| Parameter | Follicular / Proliferative Phase | Luteal / Secretory Phase |
|---|---|---|
| Days | 1-14 | 15-28 |
| Dominant hormone | Estradiol | Progesterone + Estrogen |
| Ovarian event | Follicle development | Corpus luteum |
| Endometrial thickness | Increasing | Stable/slightly decreased |
| Glands | Straight, elongating | Coiled, tortuous, secreting |
| Spiral arteries | Growing | Coiled, elongated |
| Cervical mucus | Copious, watery, ferning | Thick, scanty, no ferning |
| Basal body temperature | Lower | Rises ~0.5°C (thermogenic effect of progesterone) |
Key point on cycle length variation: The secretory phase is remarkably constant at ~14 days. Variations in total cycle length are almost entirely due to variations in the length of the proliferative phase.
Sources: Ganong's Review of Medical Physiology, 26th ed.; Costanzo Physiology, 7th ed.; Berek & Novak's Gynecology
Menstrual cycle 1st yr mbbs
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Finding Sources
Reading File
I now have all the content needed for a thorough 1st year MBBS level answer. Let me compile it in an exam-friendly, structured format.
Menstrual Cycle - 1st Year MBBS Physiology
Definition & Basic Facts
The menstrual cycle is a series of regular, cyclic changes in the female reproductive system that prepares the body for pregnancy. Its most obvious feature is periodic vaginal bleeding (menstruation) caused by shedding of the uterine mucosa.
| Feature | Value |
|---|---|
| Average duration | 28 days (range: 21-35 days) |
| Day 1 | First day of menstrual bleeding |
| Duration of bleeding | 3-5 days |
| Blood loss | ~30-80 mL |
| Constant phase | Secretory (always 14 days) |
| Variable phase | Proliferative (determines cycle length) |
I. Hormonal Control - The Axis
The cycle is controlled by the Hypothalamus - Anterior Pituitary - Ovary (HPO) axis.
Hypothalamus → GnRH (pulsatile)
↓
Anterior Pituitary → FSH + LH
↓
Ovary → Estrogen + Progesterone
↓
Feedback to Hypothalamus & Pituitary
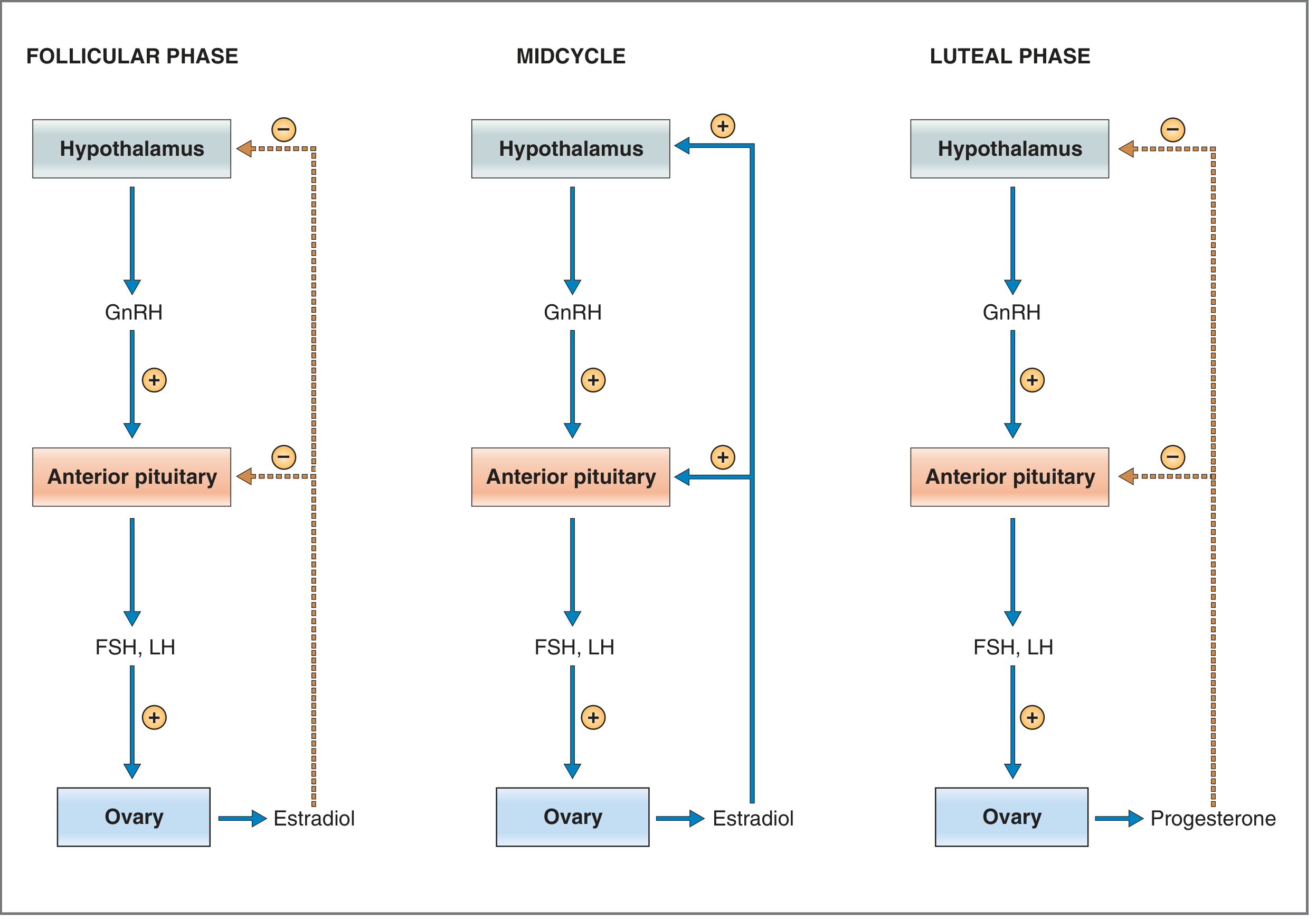
Key feedback rules:
- Follicular phase - Rising estradiol → Negative feedback → suppresses FSH/LH
- Midcycle - When estradiol reaches ≥200 pg/mL → Positive feedback → triggers the LH surge → ovulation
- Luteal phase - Progesterone (from corpus luteum) → Negative feedback → suppresses FSH/LH
Exam tip: Estradiol is unique - it causes negative feedback at low levels and positive feedback at high levels. This is called the "switch" in feedback.
II. Two-Cell Two-Gonadotropin Theory
This explains how estrogen is produced in the ovarian follicle:
- LH acts on Theca interna cells → produces androgens (androstenedione, testosterone)
- Androgens cross to granulosa cells
- FSH acts on Granulosa cells → activates aromatase → converts androgens to estradiol
So both cells + both gonadotropins are needed for estrogen production.
III. Ovarian Cycle (What happens in the ovary)
Anatomy of the Ovary:
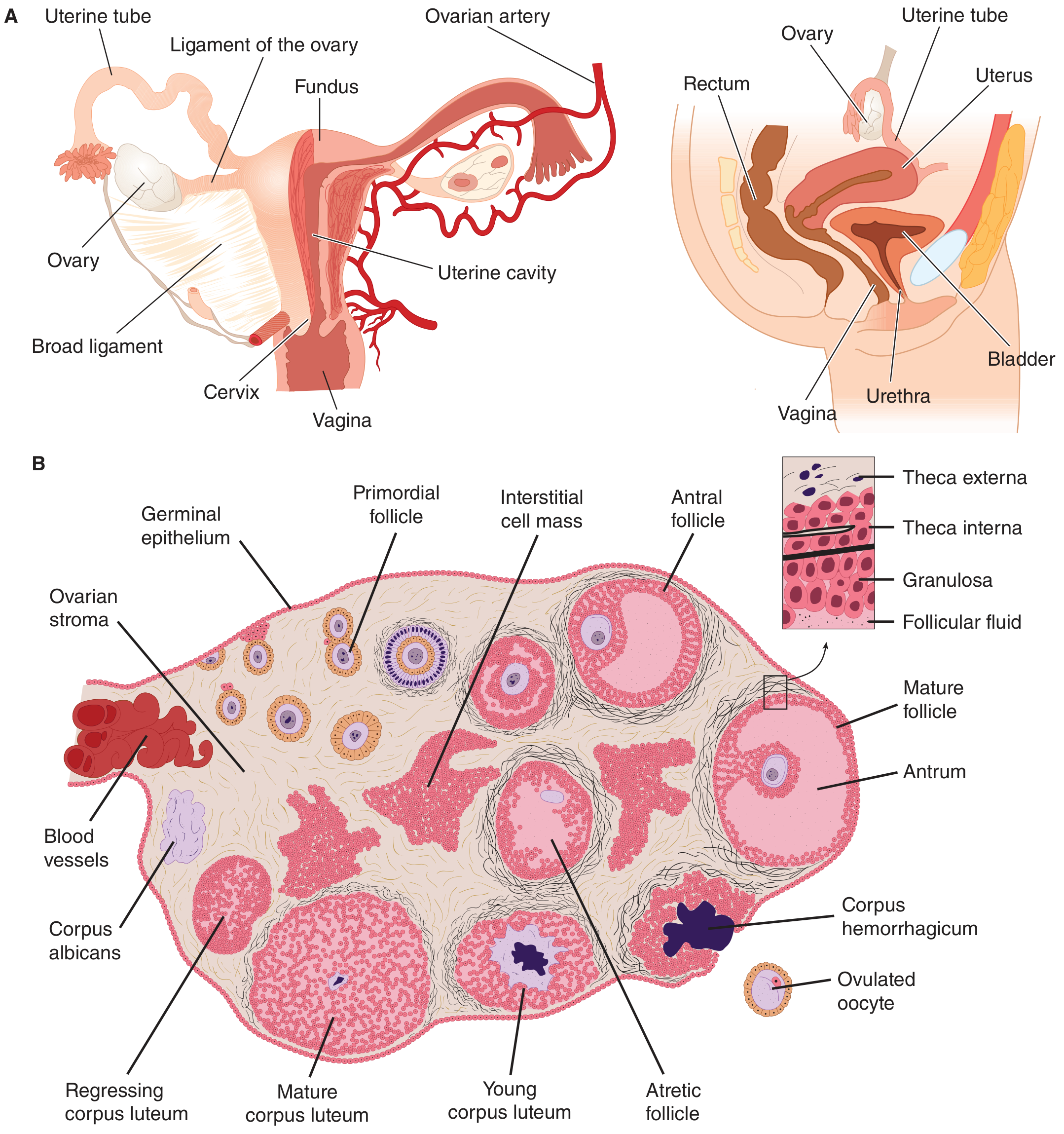
Phase 1: Follicular Phase (Days 1-14)
- At birth, ~2 million primordial follicles exist; by puberty, <300,000 remain
- Each cycle, FSH stimulates several primordial follicles to enlarge and form an antrum (fluid-filled cavity) - these become antral/secondary follicles
- By Day 6, one follicle becomes dominant (Graafian follicle); the rest undergo atresia (apoptosis)
- The Graafian follicle produces increasing amounts of estradiol
- Estradiol levels peak just before day 14
Phase 2: Ovulation (Day ~14)
- Estradiol ≥200 pg/mL triggers the LH surge (positive feedback)
- The distended follicle ruptures within 24-36 hours of the LH surge
- The secondary oocyte (arrested at metaphase II) is released into the peritoneal cavity
- The fimbriae of the fallopian tube pick up the ovum
- Minor peritoneal bleeding may cause mittelschmerz (mid-cycle pain)
Phase 3: Luteal Phase (Days 15-28)
- The ruptured follicle fills with blood → corpus hemorrhagicum
- Granulosa + theca cells proliferate → Corpus luteum (yellowish, lipid-rich)
- Corpus luteum secretes both progesterone + estrogen; progesterone dominates
- VEGF is essential for corpus luteum vascularization and survival
- If no pregnancy: Corpus luteum degenerates by Day 25-26 → becomes corpus albicans (white scar tissue) → estrogen/progesterone fall → menstruation begins
- If pregnancy occurs: hCG from trophoblast maintains corpus luteum → no menstruation
IV. Uterine Cycle (What happens in the endometrium)
The endometrium has two layers:
- Stratum functionale (superficial 2/3) - shed each month; supplied by spiral arteries
- Stratum basale (deep 1/3) - never shed; source of regeneration; supplied by basilar arteries
Phase 1: Menstrual Phase (Days 1-4)
- Corpus luteum regresses → estrogen and progesterone withdrawal
- Spiral artery vasospasm → ischemia of stratum functionale
- Prostaglandin F2α (PGF2α) - potent vasoconstrictor; amplifies vasospasm; drives myometrial contractions to expel tissue (responsible for menstrual cramps/dysmenorrhea)
- Stratum functionale is shed as menstrual flow (~30-80 mL)
- Menstrual blood: 75% arterial, 25% venous; contains fibrinolysin (prevents clot formation under normal flow)
Phase 2: Proliferative Phase (Days 5-14)
Driven by estrogen from the growing follicle:
- Endometrium regenerates and thickens rapidly (days 5 to 14)
- Uterine glands: straight and elongating (not secreting)
- Spiral arteries grow
- Cervical mucus: copious, watery, elastic → shows "ferning" pattern on a glass slide → forms channels that allow sperm penetration
Phase 3: Secretory Phase (Days 15-28)
Driven by progesterone + estrogen from the corpus luteum:
- Endometrial growth slows; becomes edematous and highly vascular
- Uterine glands: coiled, tortuous, fill with glycogen vacuoles (PAS-positive) and begin secreting
- Spiral arteries: elongated and coiled
- Around Day 22-24: stromal cells take on a decidua-like appearance (pseudodecidual change)
- Secretory activity is maximal at postovulatory days 6-7 - optimal window for blastocyst implantation
- Cervical mucus: thick, scanty, non-elastic → no ferning → blocks sperm penetration
- 2 days before menses: polymorphonuclear leukocyte infiltration signals imminent endometrial breakdown
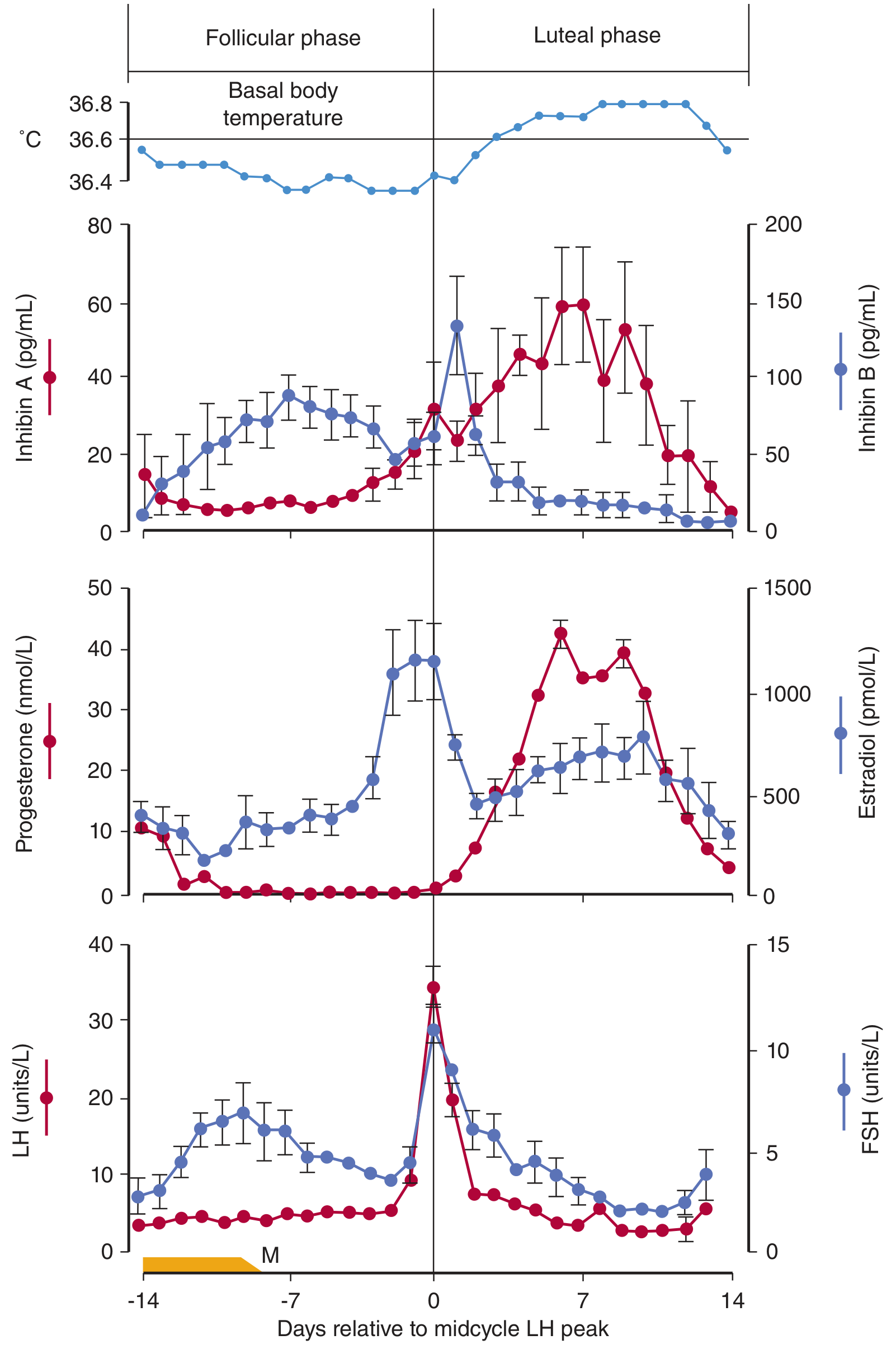
V. Hormonal Changes Summary (The Classic Diagram Pattern)
| Hormone | Early Follicular | Late Follicular | Midcycle | Luteal |
|---|---|---|---|---|
| FSH | Rises (stimulates follicle) | Falls (negative feedback) | Small surge | Low |
| LH | Low | Rises | LH surge (ovulation trigger) | Low |
| Estradiol | Low → rising | Peak | Slight dip | Second smaller peak |
| Progesterone | Very low | Very low | Slight rise | Peak |
VI. Other Cyclic Changes
| Structure | Follicular Phase | Luteal Phase |
|---|---|---|
| Cervical mucus | Watery, elastic, ferning | Thick, scanty, no ferning |
| Vaginal epithelium | Proliferates | Desquamates |
| Basal body temperature | Lower | Rises ~0.5°C (thermogenic effect of progesterone) |
| Breast | Minimal change | Slight swelling/tenderness |
VII. Key Points for Exam (MBBS Must-Know)
- Day 1 = First day of bleeding (not day of ovulation)
- Ovulation always occurs 14 days before the next period, regardless of cycle length
- LH surge triggers ovulation; occurs ~24-36 h before rupture
- Secretory phase = constant 14 days; Proliferative phase = variable (determines cycle length)
- Ferning of cervical mucus = follicular phase (estrogen effect); absent in luteal phase (progesterone)
- PGF2α = key mediator of menstruation and dysmenorrhea (NSAIDs work by blocking prostaglandin synthesis)
- Corpus luteum lifespan = 14 days without pregnancy; maintained by hCG in pregnancy
- Inhibin (from granulosa cells) selectively inhibits FSH - ensures only one dominant follicle
- Estrogen up-regulates progesterone receptors; without prior estrogen, progesterone has minimal effect
- Mittelschmerz = mid-cycle pain from minor peritoneal bleeding at ovulation
Sources: Ganong's Review of Medical Physiology, 26th ed.; Costanzo Physiology, 7th ed.; Berek & Novak's Gynecology
Spermatogenesis add note on blood testis barrier
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have all the content needed. Here is the complete, exam-ready answer:
Spermatogenesis
Definition
Spermatogenesis is the process by which primordial germ cells (spermatogonia) in the seminiferous tubules of the testes are transformed into mature spermatozoa. It begins at puberty and continues throughout adult life.
Duration: ~64-74 days (varies 42-76 days between individuals)
Daily output: ~128 million sperm/day (2 million spermatogonia each give rise to 64 spermatozoa)
Site: Seminiferous tubules (95% of testicular volume)
Site of Spermatogenesis - Seminiferous Tubule
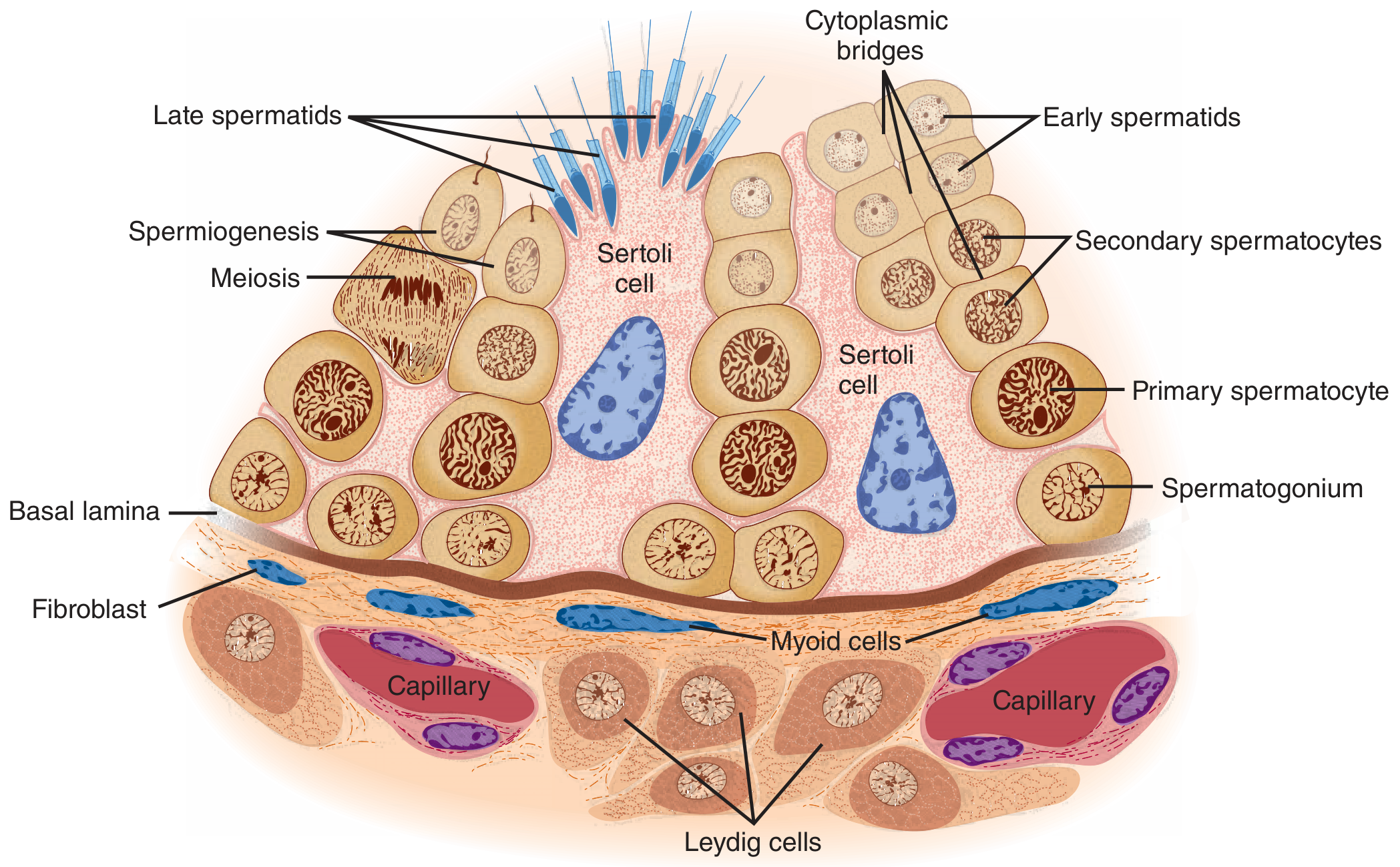
The tubule wall contains:
- Sertoli cells - large columnar cells extending from basal lamina to the lumen; nurse cells that support germ cell development
- Germ cells - arranged in layers from basal (least mature) to luminal (most mature)
- Leydig cells - in the interstitium between tubules; produce testosterone in response to LH
Three Phases of Spermatogenesis
Phase 1: Proliferative (Mitotic) Phase
- Spermatogonia (diploid, 2n) lie on the basal lamina
- They undergo mitotic divisions to produce:
- Type A spermatogonia - self-renewing stem cells (maintain the germ cell pool)
- Type B spermatogonia - committed progenitors that differentiate further
- Type B spermatogonia divide mitotically to produce primary spermatocytes (2n, 4C after DNA replication)
- Descendant cells remain connected by cytoplasmic bridges - ensures synchronized development of each clone
Phase 2: Meiotic Phase
Meiosis I (Reduction Division)
- Primary spermatocytes (2n, 4C) → Secondary spermatocytes (n, 2C)
- This is the longest step (primary spermatocytes stay in prophase I for weeks)
- Homologous chromosomes separate; crossing over occurs → genetic diversity
Meiosis II (Equational Division)
- Secondary spermatocytes (n, 2C) → Spermatids (n, 1C = haploid)
- Sister chromatids separate
- Each primary spermatocyte ultimately yields 4 spermatids
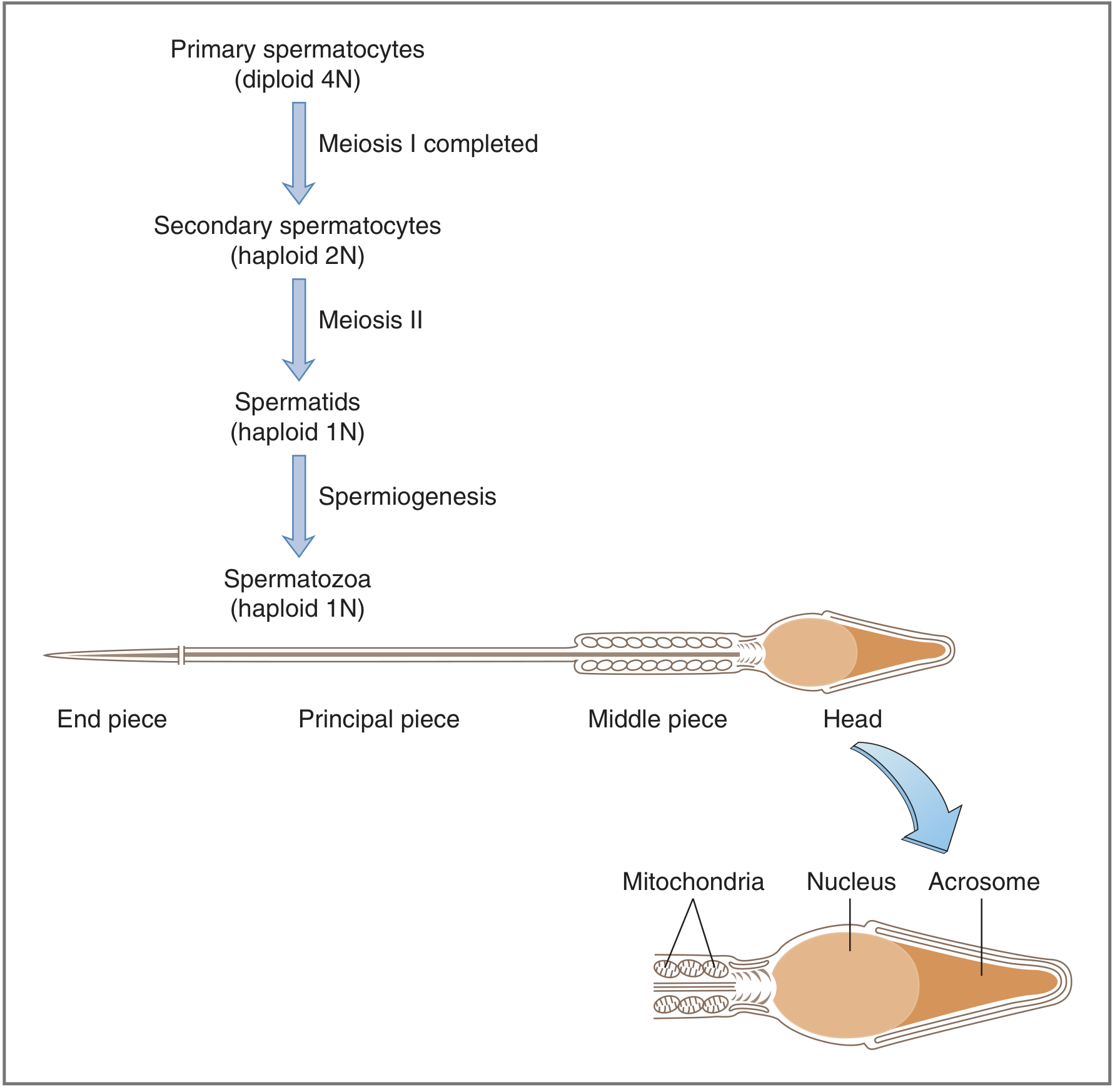
Phase 3: Spermiogenesis (Metamorphosis)
The haploid spermatids undergo morphological transformation into mature spermatozoa (no further cell division occurs):
| Change | Detail |
|---|---|
| Acrosome formation | Golgi apparatus forms the acrosome cap over the anterior nucleus |
| Nuclear condensation | Chromatin condenses; nucleus elongates |
| Tail (flagellum) formation | Axoneme (9+2 microtubule arrangement) grows from centriole |
| Mitochondrial sheath | Mitochondria arrange around the middle piece for energy (ATP) |
| Cytoplasm loss | Excess cytoplasm shed as residual body (phagocytosed by Sertoli cells) |
Structure of the Mature Spermatozoon
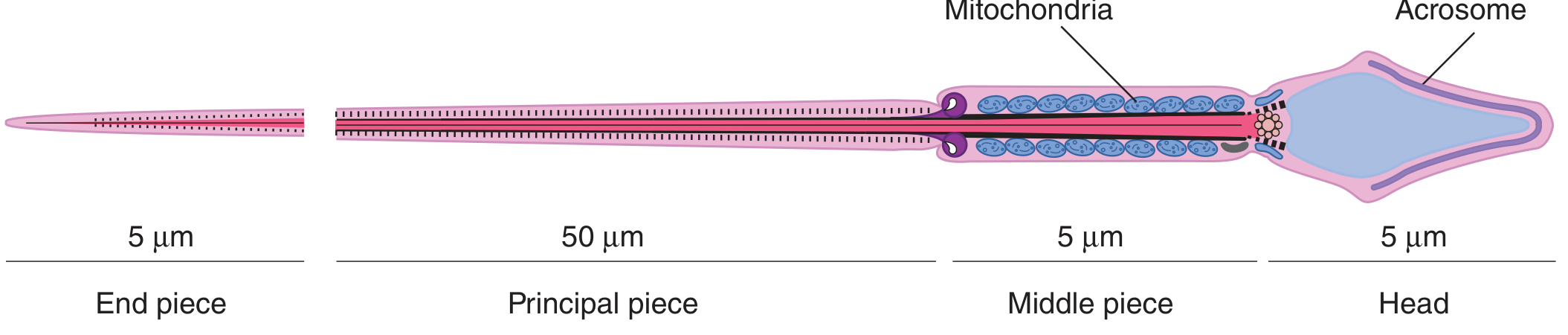
| Part | Length | Contents | Function |
|---|---|---|---|
| Head | ~5 µm | Nucleus (condensed DNA) + Acrosome cap | Genetic material; acrosome releases enzymes for zona penetration |
| Middle piece | ~5 µm | Mitochondrial sheath around axoneme | Energy (ATP) production for motility |
| Principal piece | ~50 µm | Axoneme + fibrous sheath | Main motility-generating segment |
| End piece | ~5 µm | Axoneme only | Terminal tail |
- Acrosome = lysosome-like organelle; contains hyaluronidase, acrosin, proteases → released during acrosomal reaction to penetrate zona pellucida of ovum
Hormonal Control of Spermatogenesis
Hypothalamus → GnRH (pulsatile)
↓
Anterior Pituitary → FSH + LH
↓ ↓
Sertoli cells Leydig cells
(FSH) (LH)
↓ ↓
ABP, Inhibin Testosterone
↓
Supports spermatid maturation
- FSH acts on Sertoli cells → produces Androgen Binding Protein (ABP), inhibin; facilitates last stages of spermatid maturation
- LH acts on Leydig cells → produces testosterone → essential for spermatogenesis (especially maturation of spermatids to spermatozoa)
- Inhibin (from Sertoli cells) → selectively inhibits FSH (negative feedback)
- Stages from spermatogonia → spermatids are androgen-independent; maturation of spermatids → spermatozoa requires androgens acting via Sertoli cells
Temperature requirement
Spermatogenesis requires ~32°C (3°C below body temperature). This is achieved by:
- Scrotal position outside the body
- Countercurrent heat exchange between spermatic arteries and veins
- Cryptorchidism (undescended testis) → infertility due to elevated temperature
Further Maturation After Spermatogenesis
- Spermatozoa leave the tubules non-motile
- They gain progressive motility during passage through the epididymis (stored here for months)
- After ejaculation into the female tract, capacitation occurs over 4-6 hours: inhibitory factors washed away, cholesterol removed from membrane, Ca²⁺ influx → whip-like motility and acrosomal reaction preparedness
- Fertilization occurs in the ampulla of the uterine tube
Note on Blood-Testis Barrier (BTB)
Definition
The blood-testis barrier (more accurately "blood-seminiferous tubule barrier") is a physical and immunological barrier created primarily by tight junctions between adjacent Sertoli cells near the basal lamina of the seminiferous tubule.
Structure / Components
The BTB has two components:
1. Mechanical (Anatomic) Component
- Tight junctions (occluding junctions) between adjacent Sertoli cells - the most important component
- Myoid cells (muscle-like contractile cells) that surround the outer wall of seminiferous tubules
- Capillary endothelial cells also regulate molecular traffic (secondary role)
2. Functional (Immunological) Component
- Restricted lymphocyte populations within the germinal epithelium
- T-suppressor cell tolerance generated by small, continuous leak of sperm antigens from anatomically weaker areas (rete testis, efferent tubule, epididymis)
- Sertoli cells secrete immunosuppressive molecules: galectin-1, TGF-β, interferon-γ, soluble Fc receptor, and androgens - which create a local immunosuppressive environment
What the BTB Creates
The tight junctions divide the seminiferous tubule into two compartments:
| Compartment | Location | Contents |
|---|---|---|
| Basal compartment | Below the Sertoli-Sertoli junction | Spermatogonia, early primary spermatocytes; accessible to blood-borne substances |
| Adluminal compartment | Above the junction, toward lumen | Later primary spermatocytes, secondary spermatocytes, spermatids, spermatozoa; isolated from blood |
Functions of the BTB
-
Immunological protection - Sperm are first produced at puberty, long after the immune system has become competent. Sperm antigens are recognized as "foreign" (non-self). The BTB isolates haploid germ cells (secondary spermatocytes, spermatids, spermatozoa) from the immune system, preventing autoimmune destruction.
-
Creates a specialized microenvironment - The luminal fluid differs markedly from plasma: very low protein and glucose, but rich in androgens, estrogens, K⁺, inositol, glutamic acid, and aspartic acid. ABP (secreted by Sertoli cells) maintains high testosterone concentration in tubular fluid.
-
Protection from noxious agents - Prevents bloodborne toxins, drugs, and pathogens from reaching developing germ cells.
-
Osmotic gradient - Helps maintain fluid movement into the tubular lumen.
Note: Steroids (testosterone) penetrate the BTB with ease. Some proteins also pass between Sertoli and Leydig cells in a paracrine manner.
How Germ Cells Cross the BTB
As spermatocytes move from the basal to the adluminal compartment, they must cross the Sertoli-Sertoli tight junctions. This occurs by a coordinated mechanism:
- New tight junctions form below the migrating cell
- Old tight junctions dissolve above the cell
- The barrier is never actually breached - it moves around the cell
Clinical Significance
| Situation | Consequence |
|---|---|
| Vasectomy | Disrupts the barrier → sperm leak → antisperm antibodies → immunologic infertility |
| Trauma / torsion / biopsy (post-puberty) | May expose sperm antigens → antisperm antibodies → risk of infertility |
| Same insult before puberty | No antibodies produced (no haploid germ cells yet) |
| Chemotherapy | BTB can limit drug access to cancer cells sequestered behind it → isolated testicular cancer recurrence |
| Infertility | Antisperm antibodies cause sperm agglutination → impaired motility → failure to reach/penetrate ovum |
Key exam point: The BTB develops at spermarche (puberty). Before puberty, testicular injury does NOT cause antisperm antibodies. After puberty, it does.
Sources: Ganong's Review of Medical Physiology, 26th ed.; Costanzo Physiology, 7th ed.; Campbell-Walsh-Wein Urology; Histology: A Text and Atlas (Pawlina)
Effects of estrogen on reproductive organs, indicators of ovulation, precocious puberty mbbs 1st yr
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Excellent - I now have comprehensive content from multiple authoritative sources. Let me compile the complete answer.
1. Effects of Estrogen on Reproductive Organs
Estrogen (primarily 17β-estradiol) is produced mainly by ovarian granulosa cells. Its effects on each reproductive organ are:
A. Uterus
| Effect | Detail |
|---|---|
| Endometrium | Stimulates proliferation - cell growth, gland elongation, spiral artery development (proliferative phase) |
| Myometrium | Stimulates cell growth; lowers uterine threshold to contractile stimuli (makes uterus more sensitive to oxytocin) |
| Cervix | Makes cervical mucus thin, watery, alkaline, elastic → promotes sperm survival and transport; causes ferning pattern when dried on a glass slide |
| Receptor upregulation | Upregulates progesterone receptors in uterus - without prior estrogen, progesterone has little effect |
B. Fallopian Tubes
- Stimulates ciliary activity (aids ovum transport)
- Increases peristaltic contractility to move sperm toward the ovum
- Stimulates secretory activity of tubal epithelium
C. Vagina
- Stimulates proliferation and cornification of vaginal epithelium (protective stratified squamous lining)
- Cornified cells can be identified in vaginal smear (used as an indirect indicator of estrogen activity)
- Makes vaginal secretion more acidic (protective against infection)
D. Ovary
- Promotes proliferation and development of granulosa cells
- Upregulates FSH receptors on granulosa cells (amplifies response to FSH)
- Upregulates LH receptors on granulosa cells (prepares for LH surge response)
E. External Genitalia & Female Secondary Sex Characteristics (at Puberty)
- Growth of labia majora, labia minora, and clitoris
- Development of the mons pubis and characteristic fat distribution
- Pubic and axillary hair growth (androgenic component, but estrogen contributes)
- Pigmentation of labia
F. Breasts
- Essential for breast development
- Stimulates proliferation of mammary ducts and growth of nipple/areola
- Increases fat deposition giving breasts their female shape
- Stimulates prolactin secretion from the anterior pituitary
- Blocks prolactin's action on breast tissue (so lactation doesn't occur before delivery despite high prolactin)
G. Bone
- Stimulates pubertal growth spurt
- Causes closure of epiphyseal plates (limits final height)
- Anti-osteoporotic - maintains bone mineral density
H. HPO Axis Feedback
- Low levels - negative feedback on hypothalamus and anterior pituitary (suppresses FSH/LH)
- High levels (≥200 pg/mL) - positive feedback → triggers the midcycle LH surge → ovulation
I. Metabolic Effects
- Decreases LDL cholesterol (cardioprotective before menopause)
- Increases HDL cholesterol
- Promotes subcutaneous fat deposition (female body contour)
Summary Table: Estrogen vs Progesterone on Reproductive Organs
| Organ | Estrogen | Progesterone |
|---|---|---|
| Uterus | Proliferation; ↑ contractility | Secretory activity; ↓ contractility |
| Cervical mucus | Thin, watery, elastic, ferning | Thick, scanty, non-elastic, no ferning |
| Fallopian tube | ↑ Ciliary activity; ↑ contractility | ↑ Secretion; ↓ contractility |
| Vagina | Proliferation, cornification | Differentiation; ↓ proliferation |
| Breasts | Duct proliferation | Lobule and alveolar growth |
| BBT | No significant effect | Raises by ~0.5°C (thermogenic) |
2. Indicators of Ovulation
Knowing when ovulation occurs is clinically important for fertility planning, contraception, and infertility evaluation.
A. Basal Body Temperature (BBT) Chart
- A rise of ~0.5°C (>0.5°F) in basal body temperature occurs 1-2 days after ovulation
- Sustained elevation throughout the luteal phase
- Caused by the thermogenic effect of progesterone from the corpus luteum
- Method: measure oral/rectal temperature with digital thermometer before getting out of bed each morning
- Limitation: tells you ovulation has already occurred (retrospective); not useful for timing intercourse prospectively
B. Cervical Mucus Changes (Billings/Ovulation Method)
- Around ovulation: mucus becomes copious, clear, slippery, and elastic (like raw egg white)
- Spinnbarkeit - can be stretched 8-12 cm into a long thread without breaking
- Ferning pattern - when dried on a glass slide, forms a fern-like arborizing pattern due to high estrogen (seen in anovulatory cycle with estrogen also)
- After ovulation (progesterone dominance): mucus becomes thick, scanty, cellular - ferning disappears
C. LH Surge Detection (Ovulation Predictor Kit)
- A surge in LH triggers ovulation; ovulation occurs ~9-36 hours after the LH peak
- Urinary LH can be detected by over-the-counter ovulation predictor kits
- Most useful for timing intercourse - most fertile period is 48 h before ovulation
- Limitation: presence of LH surge does not guarantee ovulation will actually occur
D. Serum Progesterone Level
- A serum progesterone >3 ng/mL (~10 nmol/L) measured approximately 7 days after expected ovulation (mid-luteal phase, Day 21 in a 28-day cycle) confirms that ovulation occurred
- Most reliable laboratory confirmation of ovulation
E. Mittelschmerz
- Mid-cycle pelvic/lower abdominal pain caused by rapid expansion of the dominant follicle and/or minor peritoneal bleeding at follicle rupture
- Unilateral, brief, occurring ~Day 14
- Clinical sign of impending ovulation
F. Premenstrual Symptoms (Moliminal Symptoms)
- Bloating, breast tenderness, mood changes, food cravings in the 7-10 days before menses suggest an ovulatory cycle (due to progesterone)
- Absence is not conclusive for anovulation
G. Ultrasound (Gold Standard for Clinical Use)
- Pre-ovulation: growth of fluid-filled dominant follicle (>18 mm = mature)
- Post-ovulation: collapse of dominant follicle, appearance of corpus luteum, characteristic echogenicity of secretory endometrium
- Most accurate non-invasive method
H. Endometrial Biopsy (Historical)
- Secretory endometrium on biopsy confirms progesterone action and therefore ovulation
- No longer used routinely to assess fertility
Summary of Indicators
| Indicator | Timing | What it shows |
|---|---|---|
| BBT rise | 1-2 days after ovulation | Retrospective; progesterone effect |
| Ferning of cervical mucus | Around ovulation | Estrogen peak |
| Spinnbarkeit | Around ovulation | Estrogen effect |
| LH surge (urine kit) | ~24-36 h before ovulation | Prospective timing aid |
| Serum progesterone >3 ng/mL | Day 21 (mid-luteal) | Best lab confirmation |
| Mittelschmerz | Day 14 | Clinical sign at ovulation |
| Ultrasound | Pre- and post-ovulation | Gold standard imaging |
3. Precocious Puberty
Definition
Onset of secondary sexual characteristics at an abnormally early age:
- Girls: before 8 years (some guidelines: <7 years in white girls, <6 years in black girls)
- Boys: before 9 years
Incidence: 1 in 5000-10,000 children; ~10x more common in girls than boys
Classification
Type 1: Central (True) Precocious Puberty = GnRH-Dependent
- Due to premature activation of the HPO axis (hypothalamus begins pulsatile GnRH secretion early)
- Gonadotropins (FSH and LH) are elevated
- Complete puberty with all secondary characteristics
- Isosexual (appropriate to genetic sex)
Causes:
| Cause | Notes |
|---|---|
| Idiopathic (constitutional) | Most common in girls (>75% of cases); no identifiable cause |
| CNS lesions | Hamartoma of the tuber cinereum (most common CNS cause), gliomas, astrocytomas, meningitis, encephalitis, hydrocephalus, radiation, trauma |
| Primary hypothyroidism | Severe hypothyroidism - elevated TRH stimulates gonadotropins |
| Silver-Russell syndrome | Rare |
| Genetic mutations | MKRN3 loss-of-function (most common genetic cause), kisspeptin/GPR54 gain-of-function, DLK1 mutations |
Key concept: Kisspeptin (KISS1) and its receptor GPR54 are essential regulators of GnRH secretion. Activating mutations cause precocious puberty; loss-of-function causes hypogonadotropic hypogonadism.
Type 2: Peripheral (Precocious Pseudopuberty) = GnRH-Independent
- Sex steroid secretion occurs independent of LH/FSH (gonadotropins are suppressed)
- Due to autonomous production of sex steroids
Causes:
| Cause | Sex steroids produced |
|---|---|
| Ovarian tumors (granulosa cell, thecoma) | Estrogen (isosexual precocity) |
| Adrenal tumors | Androgens or estrogens |
| Congenital adrenal hyperplasia (CAH) | Androgens → heterosexual precocity in girls |
| McCune-Albright syndrome | Estrogens; autonomous follicle activation (GNAS1 mutation in Gα subunit) |
| hCG-secreting tumors | Stimulates steroidogenesis |
| Exogenous estrogens | Estrogen creams, medications |
Type 3: Incomplete (Benign Variants) - Not True Precocious Puberty
| Condition | Features |
|---|---|
| Premature thelarche | Isolated breast development (<2 yrs) with no other signs; usually self-limited |
| Premature pubarche/adrenarche | Isolated pubic/axillary hair; due to early adrenal androgen production |
| Isolated menarche | Rare |
Tanner Stages of Puberty in Girls (for reference)
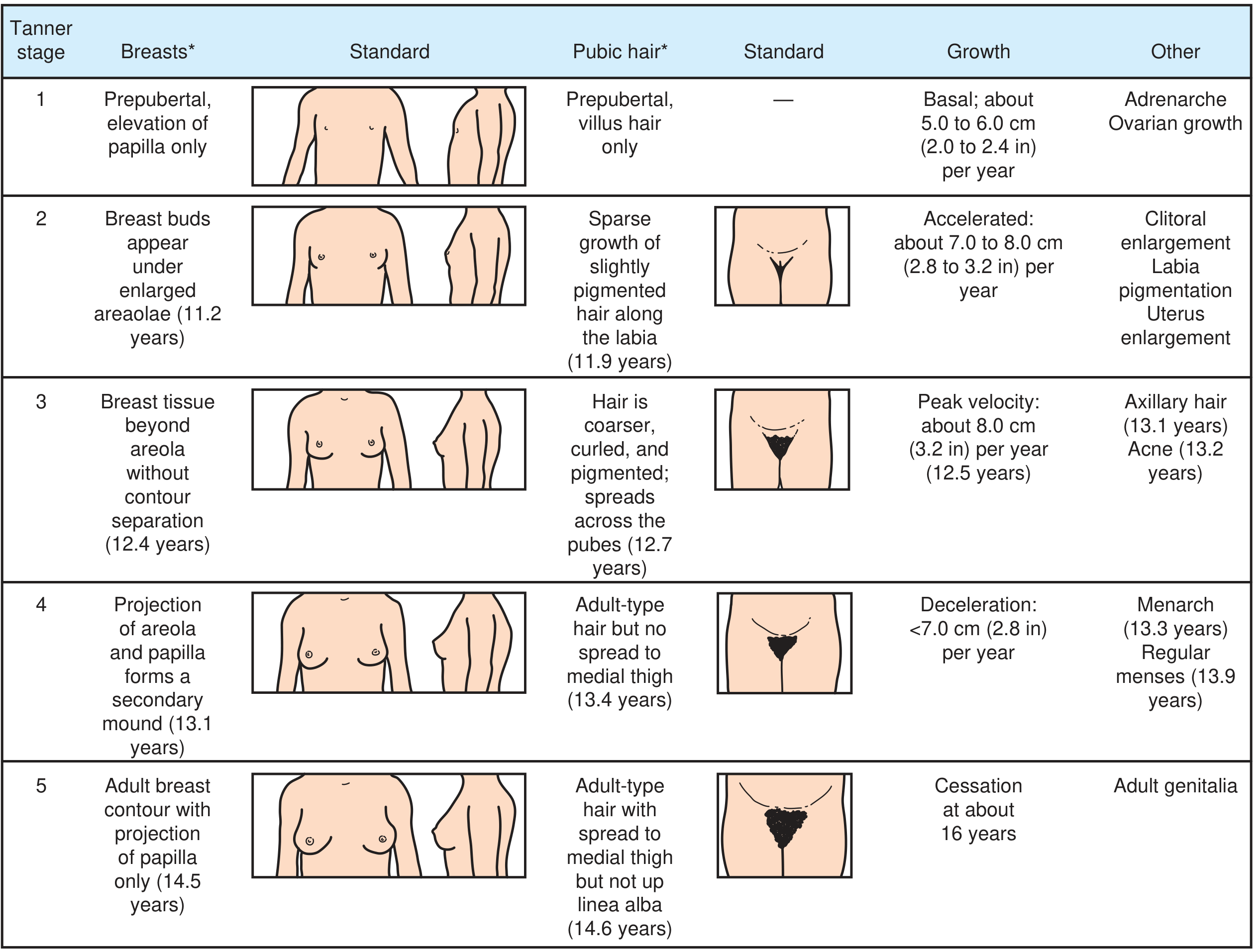
Clinical Features of Precocious Puberty
- Early development of secondary sex characteristics (breast, pubic/axillary hair, menarche)
- Accelerated linear growth (tall initially for age)
- Early epiphyseal fusion → premature growth arrest → short final adult height
- Psychological and psychosocial disturbances
- Bone age advanced beyond chronological age
Investigations
- Bone age (wrist X-ray) - advanced in true precocious puberty
- Serum FSH, LH, estradiol/testosterone - elevated in central; suppressed in peripheral
- GnRH stimulation test - pubertal LH response confirms central (GnRH-dependent) precocity
- MRI brain - mandatory to rule out CNS lesions in central precocious puberty
- Pelvic/adrenal ultrasound - to detect ovarian/adrenal tumors
- 17α-hydroxyprogesterone, DHEAS - to rule out CAH
Treatment
| Type | Treatment |
|---|---|
| Central (idiopathic) | Long-acting GnRH analogues (leuprolide) - downregulate GnRH receptors → suppress FSH/LH → halt puberty; discontinue at age 11; puberty resumes normally |
| CNS lesion | Treat underlying lesion |
| McCune-Albright syndrome | Aromatase inhibitors (testolactone, letrozole), antiestrogens |
| CAH | Glucocorticoid replacement |
| Gonadal/adrenal tumor | Surgery |
| Benign variants | Observation; reassurance |
Key exam points:
- GnRH analogues used continuously (not pulsatile) → downregulation of receptors → suppress axis
- Treatment is most effective for final height if started before age 6
- After stopping GnRH analogue, normal puberty resumes
- A testicular insult before puberty does NOT cause antisperm antibodies (no haploid cells yet)
Sources: Ganong's Review of Medical Physiology, 26th ed.; Costanzo Physiology, 7th ed.; Harrison's Principles of Internal Medicine, 22nd ed.; Goldman-Cecil Medicine; Textbook of Family Medicine, 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.