Clinical anatomy, physiologs of the pharynx. Pharyngeal spaces. Acute diseases of the pharynx (primary and secondary angina). Peritonsillar abscess.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Now I have all the material needed for a comprehensive response. Let me compile it.
Clinical Anatomy & Physiology of the Pharynx, Pharyngeal Spaces, and Acute Pharyngeal Diseases
1. CLINICAL ANATOMY OF THE PHARYNX
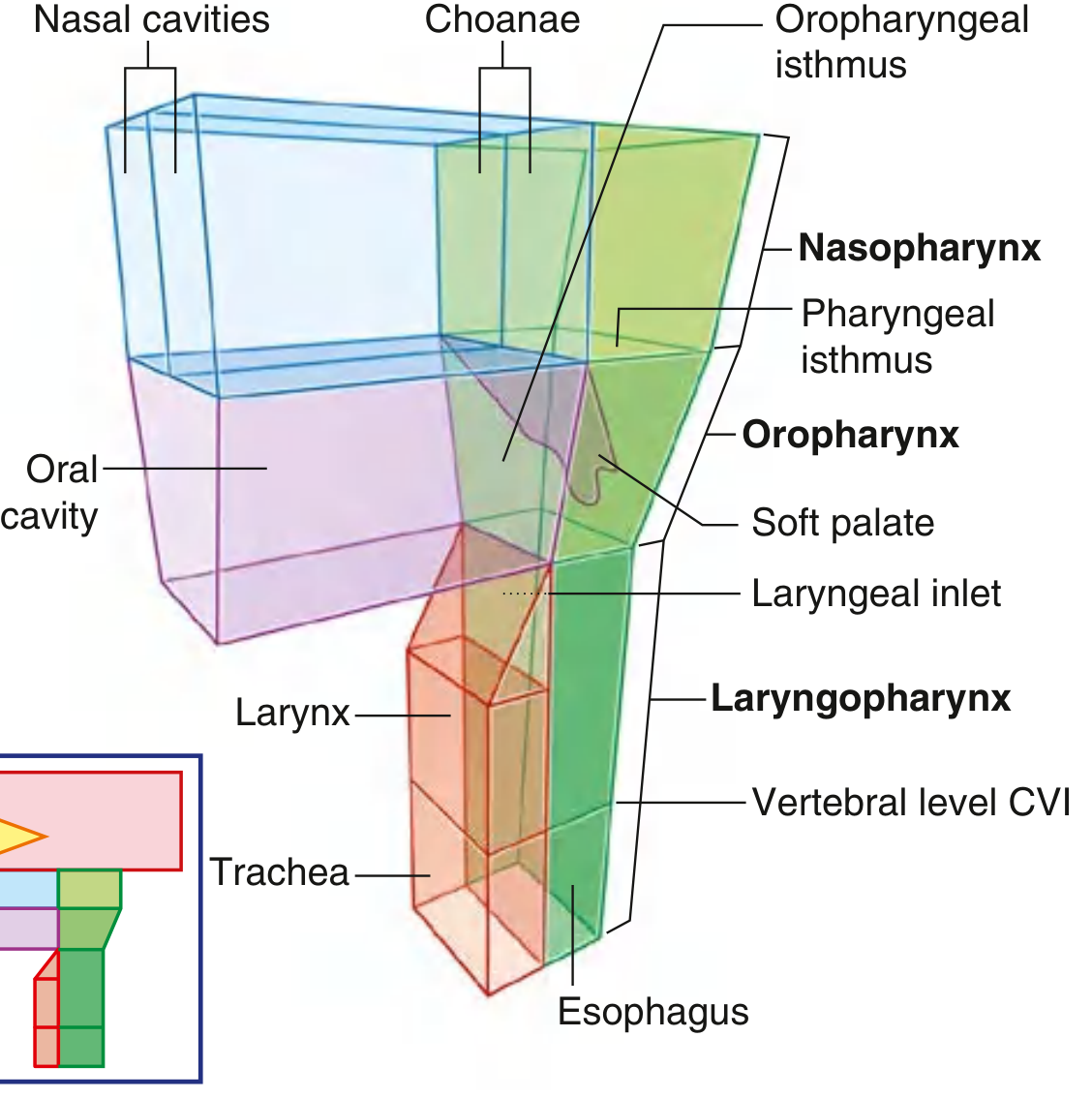
Fig. 8.201 — Pharynx. Gray's Anatomy for Students
The pharynx is a musculofascial half-cylinder that links the oral and nasal cavities to the larynx and esophagus. It is attached above to the base of the skull and is continuous below (at approximately vertebral level C6) with the esophagus. The pharyngeal cavity is a common pathway for both air and food. — Gray's Anatomy for Students
Subdivisions
| Region | Anterior relationship | Key opening |
|---|---|---|
| Nasopharynx | Posterior apertures of nasal cavities (choanae) | Pharyngotympanic (Eustachian) tubes on lateral walls |
| Oropharynx | Posterior wall of oral cavity | Oropharyngeal isthmus (palatoglossal arches) |
| Laryngopharynx (Hypopharynx) | Posterior aspect of larynx | Laryngeal inlet; continuous with esophagus inferiorly |
Skeletal Framework & Muscles
- Superior margin attaches to the skull base (pharyngeal tubercle of occiput, petrous temporal, medial pterygoid plates, pterygomandibular raphe, mandible, and hyoid).
- The posterior midline is formed by the pharyngeal raphe — a vertical fibrous cord to which the bilateral constrictor muscles attach.
Constrictor muscles (all insert into the pharyngeal raphe posteriorly):
- Superior constrictor — arises from the pterygomandibular raphe and nearby bone
- Middle constrictor — arises from the hyoid bone and stylohyoid ligament
- Inferior constrictor — arises from the oblique line of the thyroid cartilage and cricoid cartilage; its lower fibers (cricopharyngeus) act as the upper esophageal sphincter
Longitudinal (elevator) muscles — salpingopharyngeus, stylopharyngeus, palatopharyngeus — all pass inside the constrictors and act to elevate and widen the pharynx during swallowing.
Nerve Supply
- Motor: Pharyngeal plexus (CN X + CN IX + sympathetics)
- Sensory: CN IX (oropharynx & nasopharynx), CN X (laryngopharynx), CN V2 (roof of nasopharynx)
Lymphoid Tissue — Waldeyer's Ring
A ring of lymphoid tissue guards the pharyngeal entrance:
- Pharyngeal tonsil (adenoids) — roof of nasopharynx
- Tubal tonsils — around pharyngotympanic tube openings
- Palatine tonsils — in tonsillar fossae of oropharynx, between palatoglossal and palatopharyngeal arches
- Lingual tonsil — posterior tongue base
Palatine tonsil vasculature (important for tonsillectomy): chief arterial supply is the tonsillar artery (branch of the facial artery); additional supply from ascending pharyngeal, lingual, greater palatine, and ascending palatine arteries. The external palatine (paratonsillar) vein passes between the tonsil and superior constrictor — injury during tonsillectomy causes hemorrhage. — Gray's Anatomy for Students
2. PHYSIOLOGY OF THE PHARYNX
The pharynx serves three major functions:
Respiration
The pharynx is part of the upper airway. The soft palate functions as a "flutter valve":
- Elevates to close the pharyngeal isthmus → seals nasopharynx from oropharynx (during swallowing/speaking)
- Depresses to close the oropharyngeal isthmus → seals oral cavity from oropharynx
The cricopharyngeus muscle (lower inferior constrictor) acts as the upper esophageal sphincter, normally closed at rest to prevent air entry into the esophagus.
Deglutition (Swallowing) — Pharyngeal Phase
The pharyngeal phase of swallowing involves:
- Soft palate elevation closes the nasopharynx (prevents nasal regurgitation)
- Sequential contraction of pharyngeal constrictors (peristaltic wave)
- Larynx elevation and epiglottic deflection protects the airway
- Cricopharyngeus relaxation allows the bolus to pass into the esophagus
Phonation
The pharynx acts as a resonating chamber. The nasopharynx contributes to nasal resonance; its exclusion by soft palate elevation produces oral resonance.
3. PHARYNGEAL SPACES
Detailed understanding of the fascial spaces surrounding the pharynx is essential for understanding the spread of infection, abscesses, and tumors. — Cummings Otolaryngology
Parapharyngeal Space (PPS)
The anatomic epicenter of suprahyoid neck anatomy. A fibrofatty fascial space extending from the skull base to the hyoid bone.
- Contents: fat, CN V3, internal maxillary artery, ascending pharyngeal artery, venous plexus
- Shape: triangular in axial plane; hourglass in coronal plane
- Significance: serves as a marker — displacement of the PPS indicates the fascial space of origin of a lesion. Because few lesions arise from the PPS itself, most lesions found there have spread secondarily from an adjacent space.
- The fascial spaces arranged around the PPS: Pharyngeal Mucosal Space, Carotid Space, Parotid Space, Masticator Space, Retropharyngeal Space, Prevertebral Space
Pharyngeal Mucosal Space (PMS)
- Lies medial to the PPS, anterior to the prevertebral space
- Encompasses mucosal surfaces of nasopharynx and oropharynx, lymphoid (adenoidal) tissue, minor salivary glands, portions of constrictor muscles, and muscles of deglutition
- Extends from skull base to lower margin of cricoid cartilage
- Lesions here displace the PPS laterally
Retropharyngeal Space
- Located between the posterior pharyngeal wall and the prevertebral fascia
- Contains loose connective tissue and lymph nodes (particularly important in children — retropharyngeal lymphadenitis and abscess)
- Extends from the skull base to approximately T3 (where the alar and visceral fascia fuse)
- Clinically crucial: infection here can spread inferiorly into the posterior mediastinum ("danger space" route)
Danger Space
- Lies between the alar and prevertebral fascia
- Potential pathway for spread of infection from the neck directly into the posterior mediastinum — a life-threatening complication
Infrahyoid Retropharyngeal Space
- The infrahyoid portion of the retropharyngeal space is clinically relevant for spread of hypopharyngeal infections and post-cricoid carcinoma invasion
Prevertebral Space
- Between the prevertebral fascia and the vertebral column
- Infections here (e.g., Pott's disease) can bulge anteriorly to displace the pharynx
4. ACUTE DISEASES OF THE PHARYNX
4A. Primary Angina (Acute Pharyngitis / Tonsillitis)
"Angina" (from Latin angere, to strangle) in this context refers to inflammatory disease of the tonsils and pharynx. Primary angina arises directly from pharyngeal infection, as opposed to secondary angina which is a manifestation of systemic disease.
Etiology
Viruses account for most cases of acute pharyngitis.
| Pathogen | Disease | Estimated % |
|---|---|---|
| Rhinovirus | Common cold | 15–20% |
| Adenovirus | Pharyngoconjunctival fever | 6% |
| Herpes simplex virus | Gingivitis/stomatitis/pharyngitis | 4% |
| Epstein-Barr virus | Infectious mononucleosis | <1% |
| Streptococcus pyogenes (GABHS) | Pharyngitis, tonsillitis, scarlet fever | 10–23% |
| Fusobacterium necrophorum | Pharyngitis, Lemierre's syndrome | 5–10% |
| Group C Streptococcus | Pharyngitis, tonsillitis | 3–6% |
| Corynebacterium diphtheriae | Diphtheria | <1% |
— Tintinalli's Emergency Medicine
Viral Pharyngitis
Features: vesicular or petechial pattern on soft palate and tonsils, cough, rhinorrhea, conjunctivitis, hoarseness. Generally self-limited. Treatment is supportive.
Bacterial Pharyngitis / Acute Tonsillitis
The most important bacterial cause is Group A beta-hemolytic Streptococcus (GABHS, S. pyogenes) — accounting for 10–23% of cases.
Classic features of GABHS pharyngitis (Centor criteria):
- Tonsillar exudate
- Tender anterior cervical lymphadenopathy
- Fever
- Absence of cough
Treatment: Penicillin (10-day course) remains first-line. Amoxicillin is an alternative (note: causes rash in EBV mononucleosis). For penicillin-allergic patients: clindamycin or azithromycin. — K.J. Lee's Essential Otolaryngology
Bacteriology of acute bacterial tonsillitis: S. pneumoniae, Group A beta-hemolytic Streptococcus (S. pyogenes), H. influenzae.
Secondary Angina
Secondary angina refers to tonsillopharyngeal inflammation as a manifestation of systemic disease:
- Infectious mononucleosis (EBV) — exudative tonsillitis + splenomegaly + lymphadenopathy; ampicillin/amoxicillin causes characteristic maculopapular rash
- Agranulocytosis / leukemia — ulcerative tonsillitis with necrosis in immunocompromised states
- Diphtheria (C. diphtheriae) — grayish-white pseudomembrane on tonsils that bleeds when removed; risk of myocarditis and neuropathy
- Herpangina (Coxsackievirus A) — gray-white vesicles/ulcers on soft palate, uvula, tonsillar pillars
- Scarlet fever — GABHS-related; strawberry tongue, "sandpaper" rash, pharyngeal exudate
4B. Peritonsillar Abscess (Quinsy)
A peritonsillar abscess (PTA) is a collection of purulent material between the tonsillar capsule, the superior constrictor muscle, and the palatopharyngeus muscle. It is the most common deep space infection of the head and neck. — Tintinalli's Emergency Medicine
Pathogenesis
Develops primarily as a complication of acute tonsillitis, with pus accumulating in the loose areolar tissue of the peritonsillar space (between the tonsil and its bed). Risk factors include:
- Chronic tonsillitis
- Periodontal disease
- Smoking
- Multiple courses of antibiotics
- Previous peritonsillar abscess
Epidemiology
- Primarily affects adolescents and young adults (no clear seasonal variation)
- Although typically polymicrobial, in patients aged 15–24 years Fusobacterium necrophorum is the most common organism in many communities
- Other organisms: GABHS, Staphylococcus, oral anaerobes
Clinical Features
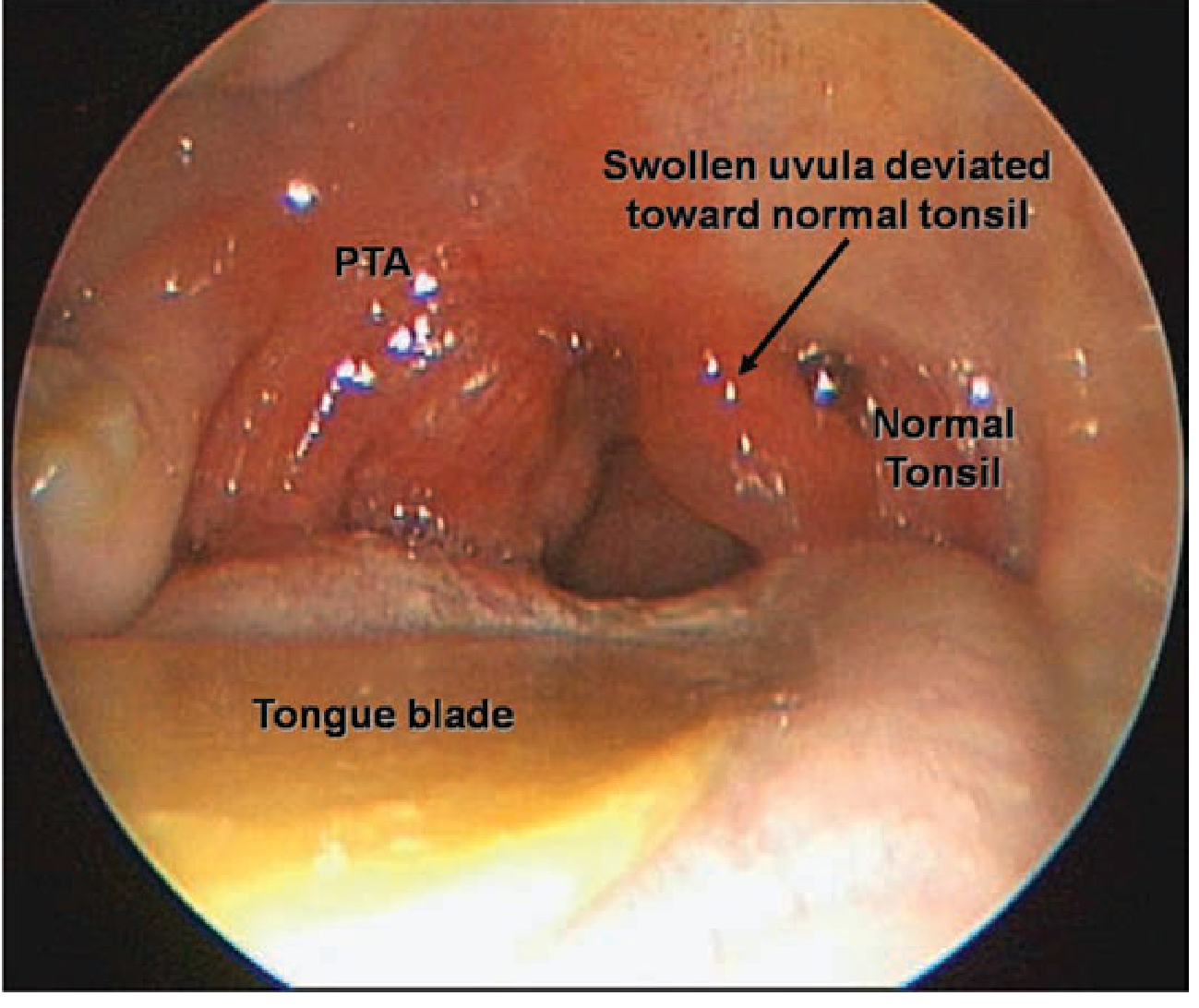
Right peritonsillar abscess (PTA): the infected right tonsil is displaced medially; the uvula is deviated toward the normal left tonsil. — Tintinalli's Emergency Medicine
| Symptom/Sign | Frequency |
|---|---|
| Sore throat | 99% |
| Fever | 54% |
| Inferior and medial displacement of tonsil | 46% |
| Contralateral deflection of uvula | 43% |
| Tender cervical lymphadenopathy | 41% |
| Trismus | 32% |
| "Hot potato voice" (muffled voice) | Common |
| Otalgia, odynophagia, dehydration | Variable |
Differential Diagnosis
- Peritonsillar cellulitis (no pus formed yet — edema and erythema of tonsillar pillar without fluctuance)
- Retropharyngeal abscess
- Infectious mononucleosis
- Lymphoma
- Internal carotid artery aneurysm
- Neoplasm
Diagnosis
- Often clinical (history + examination)
- Intraoral ultrasound: sensitivity 89–95%, specificity 79–100%
- CT with contrast: indicated when spread beyond peritonsillar space is suspected (lateral neck space, retropharyngeal space involvement)
Treatment
Drainage is the mainstay:
- Needle aspiration — ~90% effective after a single aspiration; performed at the most fluctuant point (usually superior pole)
- Incision and drainage (I&D) — definitive; some evidence of lower recurrence rate vs. needle aspiration
- Quinsy tonsillectomy (immediate tonsillectomy) — reserved for patients with strong indication for tonsillectomy (sleep apnea, recurrent tonsillitis, recurrent PTA), failure to improve, or airway compromise
Antimicrobials — 10-day course covering GABHS and oral anaerobes (including F. necrophorum):
- First-line: Penicillin VK + metronidazole
- Penicillin-allergic: clindamycin
- Toxic/unable to take PO: piperacillin-tazobactam or equivalent IV
- Adjunct: single IV dose dexamethasone 10 mg — improves severity and duration of pain
Follow-up: within 24–36 hours of aspiration.
Complications (if untreated or delayed)
- Airway obstruction
- Spontaneous rupture with aspiration of abscess contents
- Hemorrhage (erosion of carotid sheath)
- Spread to retropharyngeal or parapharyngeal space
- Mediastinitis (via danger space)
- Lemierre's syndrome (septic thrombophlebitis of internal jugular vein)
- Post-streptococcal sequelae (rheumatic fever, glomerulonephritis)
Summary Table: Key Pharyngeal Spaces
| Space | Location | Contents | Clinical Relevance |
|---|---|---|---|
| Parapharyngeal | Skull base → hyoid | Fat, CN V3, vessels | Epicenter marker; secondary tumor/abscess spread |
| Pharyngeal mucosal | Medial to PPS | Mucosa, tonsils, constrictors | Primary site of tonsillitis, nasopharyngeal carcinoma |
| Retropharyngeal | Post. pharynx wall → prevertebral fascia | Loose CT, lymph nodes | Retropharyngeal abscess, mediastinal spread |
| Danger space | Between alar & prevertebral fascia | Loose CT | Rapid mediastinitis pathway |
| Prevertebral | Anterior to vertebral column | Longus colli/capitis mm. | Pott's disease, cold abscess |
Sources: Gray's Anatomy for Students; Cummings Otolaryngology Head and Neck Surgery; Tintinalli's Emergency Medicine; K.J. Lee's Essential Otolaryngology.
This is a shared conversation. Sign in to Orris to start your own chat.