Flexors muscle of hip
Reading File
Finding Sources
Finding Sources
Reading File
Searching Images
hip flexor muscles iliopsoas anatomy
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive overview of the flexor muscles of the hip joint, organized from primary to accessory flexors.
Hip Flexors — Overview
Hip flexion is the movement that brings the anterior thigh toward the trunk. The muscles responsible can be divided into primary (major) flexors and accessory flexors.
Primary Flexors
1. Iliopsoas (Psoas Major + Iliacus)
The iliopsoas is the most powerful hip flexor — it is actually two muscles that share a common insertion.
| Feature | Psoas Major | Iliacus |
|---|---|---|
| Origin | Lumbar transverse processes, intervertebral discs, and adjacent bodies from T12–L5 | Iliac fossa |
| Insertion | Lesser trochanter of femur | Lesser trochanter of femur |
| Innervation | Anterior rami L1, L2, L3 | Femoral nerve (L2, L3) |
| Action | Flexes thigh at hip joint | Flexes thigh at hip joint |
Together they form the iliopsoas as they pass under the inguinal ligament through the muscular lacuna. When the trunk is stabilized, both flex the thigh; when the femur is fixed, they flex the trunk toward the thigh (e.g., sitting up from lying down).
The iliopsoas also contributes to lateral rotation of the thigh and to anterior bending of the trunk and pelvis.
"The lesser trochanter is the insertion for the iliopsoas, which is the strongest hip flexor." — Tintinalli's Emergency Medicine
Secondary / Accessory Flexors
2. Rectus Femoris
- Origin: Anterior inferior iliac spine (straight head); ilium just above the acetabulum (reflected head)
- Insertion: Quadriceps femoris tendon → patella → tibial tuberosity
- Innervation: Femoral nerve (L2, L3, L4)
- Action: Flexes thigh at hip and extends leg at knee
- The only part of the quadriceps group that crosses the hip joint
3. Sartorius
- Origin: Anterior superior iliac spine (ASIS)
- Insertion: Medial surface of proximal tibia (pes anserinus)
- Innervation: Femoral nerve (L2, L3)
- Action: Flexes, abducts, and laterally rotates the thigh at the hip joint; also flexes the knee
- The longest muscle in the body; crosses both hip and knee joints
4. Pectineus
- Origin: Pectineal line (pecten pubis) of the pelvic bone
- Insertion: Oblique line between the lesser trochanter and linea aspera (posterior femur)
- Innervation: Femoral nerve (L2, L3)
- Action: Adducts and flexes the thigh at the hip joint; also assists with internal rotation
- Lies in the floor of the femoral triangle
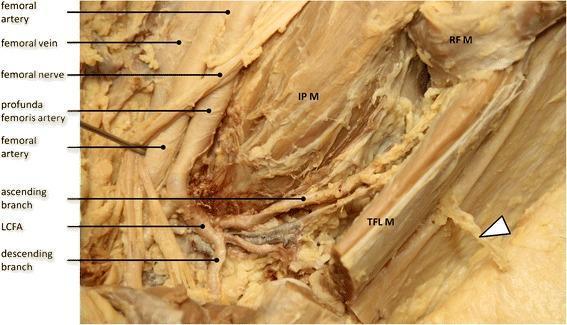
5. Tensor Fasciae Latae (TFL)
- Innervation: Superior gluteal nerve (L4, L5)
- Action: Assists hip flexion (along with abduction and medial rotation); acts via the iliotibial band
6. Adductor Longus & Adductor Brevis (accessory)
- Primarily adductors, but in a position of hip extension they can assist in flexion
Summary Table
| Muscle | Primary Action at Hip | Nerve | Spinal Level |
|---|---|---|---|
| Psoas major | Flexion | Anterior rami | L1, L2, L3 |
| Iliacus | Flexion | Femoral nerve | L2, L3 |
| Rectus femoris | Flexion + knee extension | Femoral nerve | L2, L3, L4 |
| Sartorius | Flexion, abduction, lateral rotation | Femoral nerve | L2, L3 |
| Pectineus | Flexion + adduction | Femoral nerve | L2, L3 |
| Tensor fasciae latae | Flexion + abduction | Superior gluteal | L4, L5 |
Anatomical Relationships
All major hip flexors pass under the inguinal ligament to enter the thigh through the gap between the inguinal ligament and the pelvic bone. The femoral nerve, which supplies most of these muscles, runs in close proximity to the iliopsoas in the femoral triangle.
Clinical Notes
- Iliopsoas weakness (L1–L3 lesion or femoral nerve injury) causes difficulty climbing stairs and rising from a chair
- Hip flexor tightness (especially iliopsoas) contributes to anterior pelvic tilt and low back pain — tested with the Thomas test
- Iliopsoas tendinitis/bursitis can cause anterior hip/groin pain, especially with repeated hip flexion (e.g., runners, dancers)
- In femoral nerve injury, loss of hip flexion and knee extension occurs, with loss of sensation over the anterior thigh
— Gray's Anatomy for Students, Table 6.3 & Anterior Compartment section
Extensors of hip
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
gluteus maximus hamstrings hip extensors anatomy posterior thigh
Finding Sources
Loading Image
Reading File
I now have all the information needed. Here is a comprehensive overview:
Extensor Muscles of the Hip Joint
Hip extension is the movement that carries the thigh posteriorly (or the trunk backward when the leg is fixed). There are two main groups: the gluteus maximus (the dominant extensor) and the hamstrings (posterior thigh compartment).
Primary Extensor
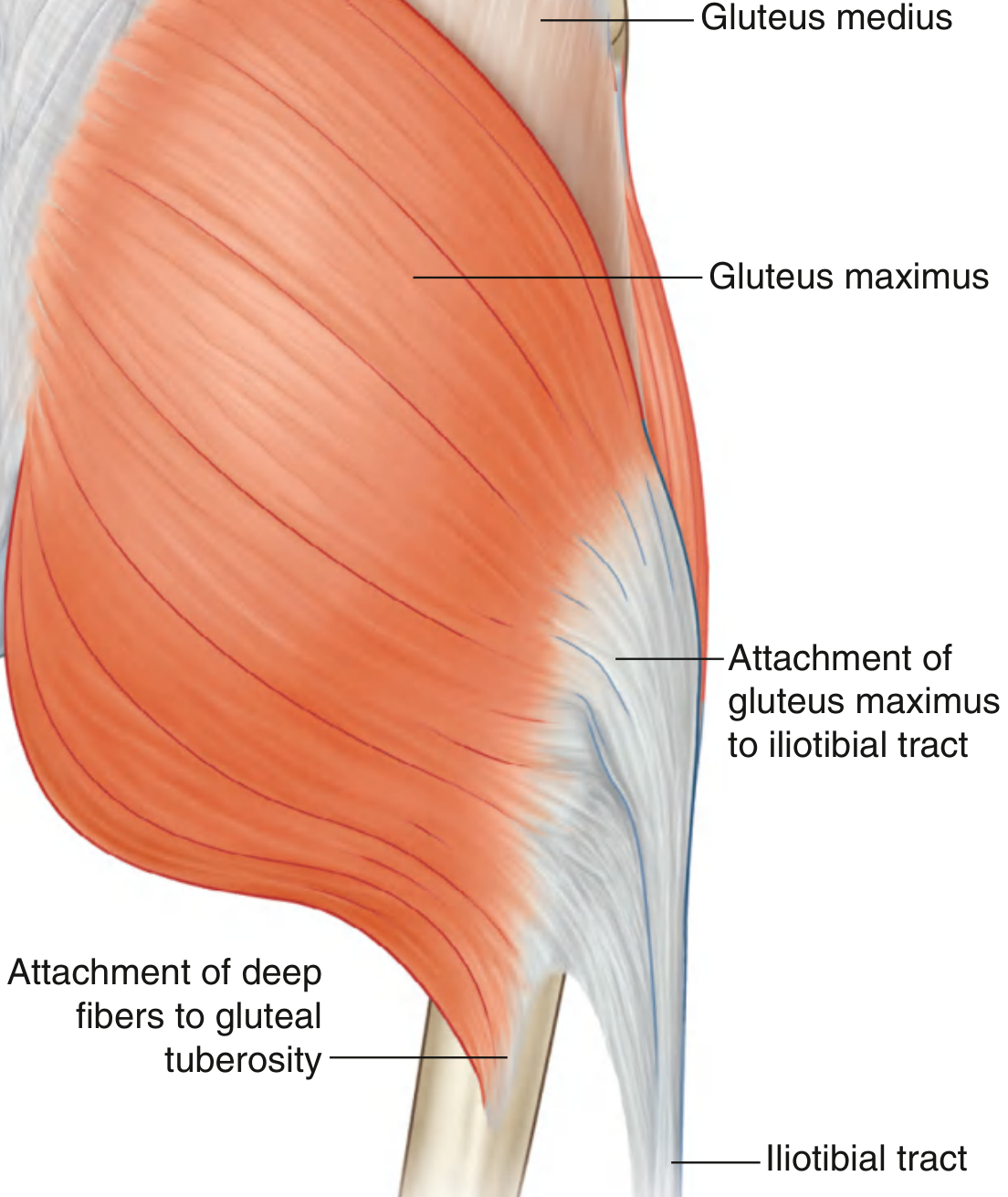
1. Gluteus Maximus
The largest and most powerful muscle in the body — the dominant hip extensor.
| Feature | Detail |
|---|---|
| Origin | Posterior gluteal surface of ilium (behind posterior gluteal line), dorsal sacrum, lateral coccyx, sacrotuberous ligament, thoracolumbar fascia |
| Insertion | Upper/superficial fibres → iliotibial tract; Deep distal fibres → gluteal tuberosity of femur |
| Innervation | Inferior gluteal nerve (L5, S1, S2) |
| Action | Extends and externally rotates the thigh; stabilizes the hip and knee (via iliotibial tract) in both the sagittal and coronal planes |
The gluteus maximus is most active when rising from a chair, climbing stairs, and running — activities that require forceful hip extension from a flexed position. It is relatively inactive during level walking.
"The gluteus maximus mainly extends the flexed thigh at the hip joint. Through its insertion into the iliotibial tract, it also stabilizes the knee and hip joints." — Gray's Anatomy for Students
Secondary Extensors — The Hamstrings
The posterior compartment of the thigh contains three long muscles collectively called the hamstrings: biceps femoris, semitendinosus, and semimembranosus. All (except the short head of biceps femoris) cross both the hip and knee joints, extending the hip and flexing the knee.
Table 6.5 from Gray's Anatomy for Students:
| Muscle | Origin | Insertion | Innervation | Action at Hip |
|---|---|---|---|---|
| Biceps femoris (long head) | Inferomedial ischial tuberosity | Head of fibula | Tibial division of sciatic nerve (L5–S2) | Extension + lateral rotation |
| Biceps femoris (short head) | Lateral lip of linea aspera | Head of fibula | Common fibular division of sciatic (L5–S2) | No hip action (crosses knee only) |
| Semitendinosus | Inferomedial ischial tuberosity (common head with long head of biceps) | Pes anserinus (medial tibia) | Tibial division of sciatic nerve (L5–S2) | Extension + medial rotation |
| Semimembranosus | Superolateral impression, ischial tuberosity | Medial tibial condyle, oblique popliteal ligament | Tibial division of sciatic nerve (L5–S2) | Extension + medial rotation |
Biceps Femoris
- Lateral in the posterior compartment
- Long head: extends and laterally rotates the hip
- Both heads: flex and laterally rotate the knee
Semitendinosus
- Medial to biceps femoris; long cord-like tendon inserts via pes anserinus
- Extends hip, medially rotates thigh; flexes and medially rotates knee
Semimembranosus
- Deepest hamstring; lies deep to semitendinosus
- Extends hip, medially rotates thigh; flexes and medially rotates knee
- Contributes to oblique popliteal ligament (stabilizes knee)
Summary Table
| Muscle | Primary Action at Hip | Nerve | Spinal Level |
|---|---|---|---|
| Gluteus maximus | Extension + external rotation | Inferior gluteal nerve | L5, S1, S2 |
| Biceps femoris (long head) | Extension + lateral rotation | Sciatic (tibial division) | L5, S1, S2 |
| Semitendinosus | Extension + medial rotation | Sciatic (tibial division) | L5, S1, S2 |
| Semimembranosus | Extension + medial rotation | Sciatic (tibial division) | L5, S1, S2 |
| Gluteus medius (post. fibres) | Accessory extension + ext. rotation | Superior gluteal nerve | L4, S1 |
| Adductor magnus (hamstring part) | Accessory extension | Sciatic (tibial division) | L4 |
Key Anatomical Points
- All hamstrings originate from the ischial tuberosity — hence avulsion injuries at this site are a classic hamstring injury in sprinters
- The sciatic nerve descends between the hamstrings, supplying them
- Gluteal tuberosity and the iliotibial tract are the two insertion points of gluteus maximus
- The pes anserinus (semitendinosus, gracilis, sartorius) inserts on the medial tibia
Clinical Notes
- Gluteus maximus weakness (inferior gluteal nerve injury or L5/S1 lesion) causes difficulty rising from a chair, climbing stairs, and a characteristic extension lurch of the trunk during walking
- Hamstring injuries (strains/tears) are among the most common sports injuries; the myotendinous junction near the ischial tuberosity is the typical site
- Hamstring tightness limits straight-leg raising and contributes to posterior pelvic tilt and low back pain
- The straight-leg raise test (Lasègue's sign) stretches the hamstrings and sciatic nerve — limited ROM or pain suggests L4/L5/S1 nerve root irritation
— Gray's Anatomy for Students, Table 6.5 & Posterior Compartment; THIEME Atlas of Anatomy
This is a shared conversation. Sign in to Orris to start your own chat.