Broncho- constrictors
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Here is a comprehensive overview of bronchoconstrictors — agents and mechanisms that narrow the airways by contracting bronchial smooth muscle.
Bronchoconstrictors
Bronchoconstrictors can be broadly categorized as endogenous mediators, exogenous/pharmacological agents, and physiological stimuli.
1. Endogenous Chemical Mediators
Histamine
- Released primarily from mast cells during allergic reactions
- Acts on H1 receptors on bronchial smooth muscle (BSM), activating phospholipase C and protein kinase C (PKC), releasing Ca²⁺ from intracellular stores
- Leads to Ca²⁺ entry through calcium channels → sustained smooth muscle contraction
- Attenuated by atropine (cholinergic antagonist), indicating a reflex cholinergic component
- In humans with normal airways, small doses produce only modest bronchoconstriction; in asthmatic airways, much more potent — Miller's Anesthesia, 10e, p. 2065; Katzung's Basic and Clinical Pharmacology, 16e
Leukotrienes (Cysteinyl Leukotrienes: LTC₄, LTD₄, LTE₄)
- Produced via the lipoxygenase pathway from arachidonic acid
- Released by mast cells, eosinophils, basophils
- Up to 1,000× more potent than histamine as bronchoconstrictors
- Also increase mucus secretion, vascular permeability, and tissue fibrosis
- Major mediators in asthma and anaphylaxis
- Blocked by leukotriene receptor antagonists (montelukast, zafirlukast) and 5-LOX inhibitors (zileuton) — Henry's Clinical Diagnosis, p. 1757; Katzung's, p. 1529; Fishman's Pulmonary Diseases
Prostaglandins
- PGD₂, PGF₂α, and TXA₂ are potent bronchoconstrictors produced by eosinophils and mast cells
- PGF₂α and TXA₂ were once thought to be primary asthma mediators; polymorphisms in their receptor genes are linked with asthma
- PGE₂, in contrast, is a bronchodilator — Katzung's, p. 1924–1926; Fishman's Pulmonary Diseases
Acetylcholine (Parasympathetic/Vagal Tone)
- Postganglionic parasympathetic fibers release ACh → acts on M3 muscarinic receptors on airway smooth muscle → contraction
- M2 receptors on nerve endings act as autoreceptors (limit further ACh release)
- M1 receptors at ganglia facilitate neurotransmission
- The dominant neural bronchoconstrictor pathway; basis for anticholinergic bronchodilators (ipratropium, tiotropium) — Katzung's, p. 2553–2566; Miller's Anesthesia
Substance P and Tachykinins
- Released from C-fiber afferents in response to inhaled irritants
- Directly stimulate smooth muscle contraction (non-adrenergic, non-cholinergic mechanism) — Katzung's, p. 2553
Bradykinin
- Generated in allergic/inflammatory states
- Stimulates rapidly adapting airway receptors and provokes bronchoconstriction
- A significant trigger in asthma and in ACE-inhibitor-induced cough/bronchospasm
Serotonin (5-HT)
- Relevant in carcinoid syndrome — circulating serotonin + bradykinin + histamine cause flushing and bronchoconstriction; carcinoid crisis can cause life-threatening bronchospasm — Miller's Anesthesia
2. Physiological/Reflexive Stimuli
| Stimulus | Mechanism |
|---|---|
| Hypocapnia (↓ PCO₂) | Low CO₂ in embolized lung segments → local bronchoconstriction (normalizes V/Q ratio) |
| Inhaled irritants (smoke, dust, cold air) | Trigger mast cell mediator release AND stimulate afferent receptors → reflex cholinergic bronchoconstriction |
| Gastroesophageal reflux | Acid reflux → vagal stimulation → bronchoconstriction |
| Exercise/hyperventilation | Airway cooling/drying → mediator release |
— Fishman's Pulmonary Diseases, p. 1932–1936
3. Pharmacological / Drug-Induced Bronchoconstrictors
| Drug/Class | Mechanism |
|---|---|
| Beta-blockers (non-selective) | Block β₂ receptors on airway smooth muscle → loss of sympathetic bronchodilator tone |
| NSAIDs / Aspirin | Shunt arachidonic acid toward lipoxygenase pathway → ↑ LTC₄/LTD₄ (aspirin-exacerbated respiratory disease) |
| Neostigmine / Pyridostigmine (anticholinesterases) | Increase ACh at muscarinic receptors → bronchospasm via M3 receptors |
| Carbachol / Methacholine | Direct muscarinic agonists; used in bronchial provocation testing |
| Histamine | Used clinically to assess airway hyperresponsiveness (PC₂₀ testing) |
| PGF₂α analogs (e.g., carboprost) | Direct smooth muscle contraction; contraindicated in asthma |
| Morphine / opioids | Histamine release from mast cells → reflex bronchoconstriction |
— Miller's Anesthesia, 10e; Katzung's Basic and Clinical Pharmacology, 16e
Neural Control of Airway Smooth Muscle
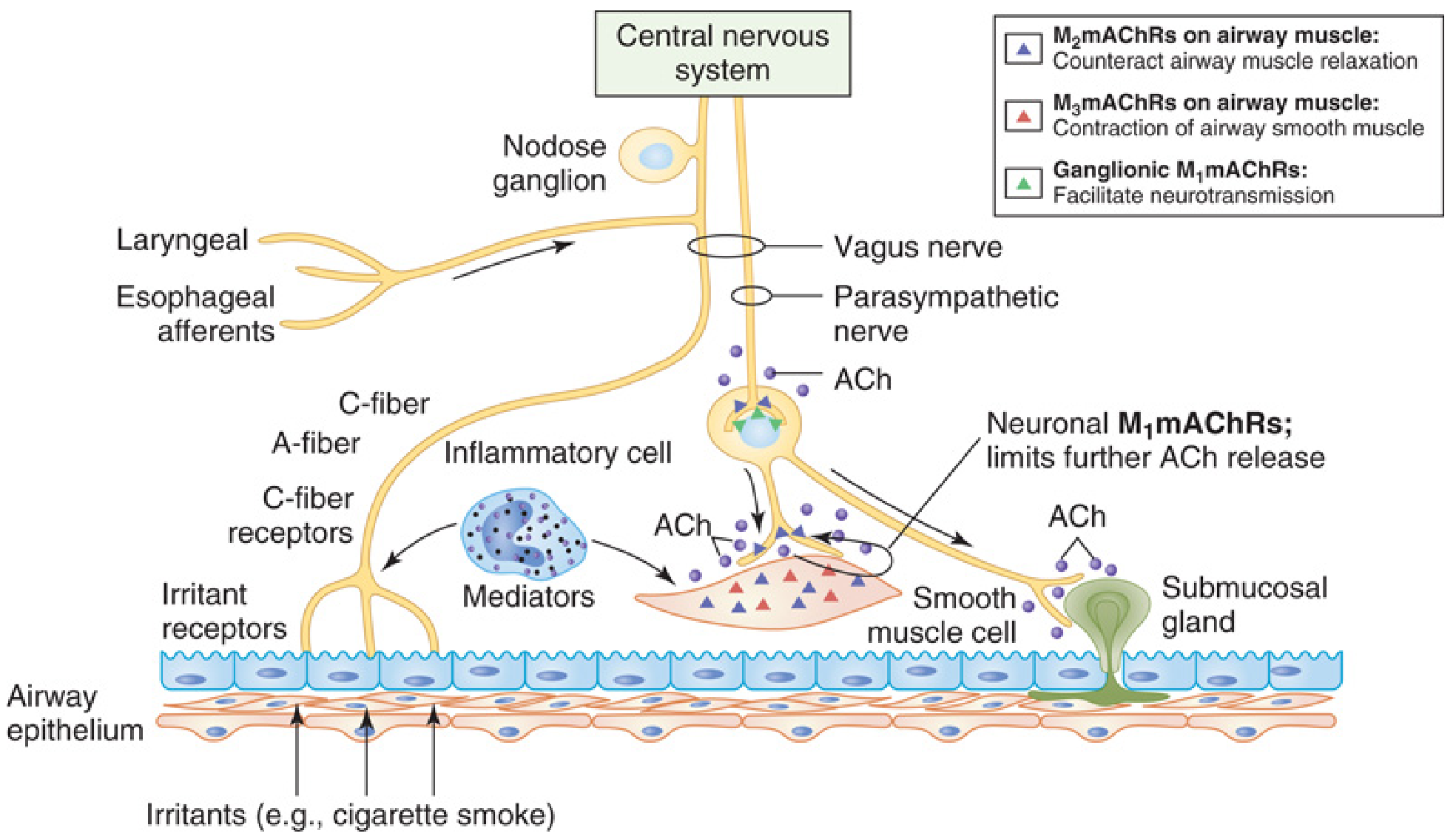
Fig. 19.1 — Control of airway smooth muscle. Irritants and inflammatory mediators activate afferent receptors and trigger ACh release via vagal reflex. M₃ receptors on smooth muscle cause contraction; M₂ autoreceptors limit further ACh release. — Miller's Anesthesia, 10e, p. 2067
Summary Table
| Category | Agent | Receptor/Mechanism |
|---|---|---|
| Biogenic amine | Histamine | H1 → ↑Ca²⁺ |
| Lipid mediator | LTC₄, LTD₄, LTE₄ | CysLT1/CysLT2 receptors |
| Lipid mediator | PGF₂α, TXA₂, PGD₂ | TP/FP/DP2 receptors |
| Neurotransmitter | Acetylcholine | M3 → smooth muscle contraction |
| Neuropeptide | Substance P | NK1/NK2 receptors |
| Peptide | Bradykinin | B2 receptors |
| Pharmacological | Beta-blockers | Block β₂ |
| Pharmacological | Anticholinesterases | ↑ACh at M3 |
| Physiological | Hypocapnia | Airway smooth muscle directly |
Understanding these mechanisms is essential for managing asthma, COPD exacerbations, anaphylaxis, and perioperative bronchospasm.
Give ne assignment formet in deep and easy language or understanding language 1 - intro 2 definition 3 mechanism of action 4 indication 5 contradiction 6 side effects 7 adverse effects and 8 nursing management . Sab ka point by point dena
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Ab main aapko poora assignment format mein deta hoon — simple, clear aur point-by-point.
📝 ASSIGNMENT
Topic: BRONCHOCONSTRICTORS
Subject: Pharmacology / Respiratory Nursing
Format: Assignment (Deep & Easy Language)
1. INTRODUCTION (Parichay)
Humara respiratory system (saans lene ka system) hawa ko lungs tak pahunchata hai. Is kaam mein bronchi aur bronchioles (chhoti naaliyan) ka bohot bada role hota hai.
Jab yeh naaliyan tang (narrow) ho jaati hain, toh saans lena mushkil ho jaata hai. Is process ko bronchoconstriction kehte hain. Aur jis cheez ki wajah se yeh narrowing hoti hai — unhe Bronchoconstrictors kehte hain.
Simple example:
Jaise ek pipe ka valve band karo — paani ki flow kam ho jaati hai. Usi tarah bronchoconstrictors airway ki "nali" ko tang kar dete hain, aur hawa ki flow kam ho jaati hai.
Bronchoconstrictors naturally body mein bhi bante hain (jaise allergic reaction mein), aur kuch drugs bhi yeh kaam karte hain. Inhe samajhna ek nurse ke liye bohot zaroori hai — kyunki asthma, COPD, aur allergic reactions mein yahi mediators zimmedaar hote hain.
2. DEFINITION (Paribhasha)
Bronchoconstrictors woh substances hain jo bronchial smooth muscle (airway ki deewar mein maujood muscle) ko contract karate hain, jis se airway ki diameter kam ho jaati hai aur saans lene mein takleef hoti hai.
Yeh 3 taraf se ho sakta hai:
- Endogenous (body ke andar se): Histamine, Leukotrienes, Acetylcholine
- Exogenous/Drugs se: Beta-blockers, NSAIDs, Carbachol
- Physiological Stimuli se: Thanda mausam, dhool, dhuaan, GERD (acid reflux)
3. MECHANISM OF ACTION (Kaise Kaam Karte Hain)
Bronchoconstrictors alag-alag tareekon se kaam karte hain. Neeche har important bronchoconstrictor ka mechanism diya gaya hai:
🔹 A. Histamine
- Allergic reaction hone par mast cells se histamine release hoti hai
- Histamine airway ki smooth muscle par H1 receptors se jud jaati hai
- Isse Phospholipase C activate hota hai → calcium (Ca²⁺) cells ke andar aata hai
- Calcium muscle ko contract karata hai → airway tang ho jaati hai
- Yahi process asthma aur anaphylaxis mein hoti hai
🔹 B. Acetylcholine (Parasympathetic Pathway)
- Brain se signal aata hai → vagus nerve active hoti hai
- Postganglionic nerves Acetylcholine (ACh) release karte hain
- ACh airway muscle par M3 muscarinic receptors se milti hai
- Isse smooth muscle contract hoti hai → bronchoconstriction
- M2 receptors autoreceptors hain — yeh aur ACh release rokne ki koshish karte hain
Yahi wajah hai ki anticholinergic drugs (jaise Ipratropium) bronchoconstriction rokti hain
🔹 C. Leukotrienes (LTC₄, LTD₄, LTE₄)
- Arachidonic acid se Lipoxygenase enzyme ke zariye bante hain
- Mast cells aur eosinophils inhe release karte hain
- Airway smooth muscle par CysLT1/CysLT2 receptors se attach hote hain
- Histamine se 1000 guna zyada powerful bronchoconstrictors hain
- Alag se mucus secretion bhi badhate hain → aur zyada blockage
- Asthma mein yeh dominant mediators hain
🔹 D. Prostaglandins (PGF₂α, TXA₂, PGD₂)
- COX pathway se arachidonic acid se bante hain
- Airway smooth muscle par TP/FP receptors se kaam karte hain
- Muscle contraction → bronchoconstriction
- NSAIDs lene par COX block hota hai → zyada leukotrienes bante hain → bronchoconstriction worse hoti hai (Aspirin-Exacerbated Respiratory Disease)
🔹 E. Beta-Blockers (Drug-Induced)
- Normal mein β₂ receptors airway ko relax rakhte hain (bronchodilation)
- Non-selective beta-blockers (jaise Propranolol) β₂ receptors block kar dete hain
- Bronchodilation band → bronchoconstriction dominant ho jaati hai
- Asthma patients mein jaan lewa ho sakta hai
🔹 F. Substance P (Tachykinins)
- Inhaled irritants (dhuaan, dhool) C-fiber nerve endings ko stimulate karte hain
- Substance P release hoti hai
- Yeh directly smooth muscle ko contract karati hai
4. INDICATIONS (Kab Use Kiya Jata Hai)
Bronchoconstrictors mostly diagnostic purposes aur research mein use hote hain, treatment mein nahi.
| # | Indication | Drug | Purpose |
|---|---|---|---|
| 1 | Bronchial Provocation Test | Methacholine, Histamine | Airway hyperresponsiveness diagnose karna (asthma confirm karna) |
| 2 | Glaucoma ka treatment | Carbachol (topically) | Intraocular pressure kam karna |
| 3 | Postoperative ileus | Bethanechol | GI motility badhana (airway effect side effect hai) |
| 4 | GERD aur carcinoid syndrome | — | Bronchoconstriction ek clinical feature hai |
| 5 | Pharmacology research/labs | Carbachol, Histamine | Airway smooth muscle ka study |
Yaad rakhein: Bronchoconstrictors ke induced effects ko treat karna (bronchodilators dena) — yeh nursing practice mein zyada kaam aata hai.
5. CONTRAINDICATIONS (Kab Nahi Dena Chahiye)
| # | Contraindication | Reason |
|---|---|---|
| 1 | Asthma patients | Bronchoconstriction severe ho sakti hai, death bhi possible |
| 2 | COPD patients | Already narrowed airways — aur tang hone se respiratory failure |
| 3 | Active bronchospasm | Condition aur worse ho jayegi |
| 4 | Severe cardiovascular disease | Vagal stimulation → bradycardia, hypotension |
| 5 | Pregnancy | PGF₂α analogs uterus contract karte hain + fetal distress |
| 6 | Hypersensitivity/Anaphylaxis history | Histamine release ya allergic cascade trigger ho sakta hai |
| 7 | Peptic ulcer disease | Muscarinic agonists (carbachol) acid secretion badhate hain |
| 8 | Urinary obstruction | Carbachol bladder contraction badha sakta hai |
6. SIDE EFFECTS (Samanye Prabhav — Common Effects)
Yeh effects chhote hote hain aur aksar khatam ho jaate hain:
| # | Side Effect | Wajah |
|---|---|---|
| 1 | Wheezing | Airway narrow hona |
| 2 | Cough | Airway irritation |
| 3 | Chest tightness | Smooth muscle contraction |
| 4 | Shortness of breath (dyspnea) | Reduced airflow |
| 5 | Nasal congestion | Vasodilation + mucus |
| 6 | Increased mucus secretion | Leukotrienes/muscarinic effects |
| 7 | Nausea / Vomiting | Muscarinic GI effects |
| 8 | Diarrhea | GI smooth muscle contraction |
| 9 | Salivation / Lacrimation | Parasympathetic overstimulation |
| 10 | Sweating | Cholinergic stimulation |
| 11 | Headache | Histamine-induced vasodilation |
7. ADVERSE EFFECTS (Gambhir/Serious Effects)
Yeh zyada dangerous hote hain aur turant management chahiye:
| # | Adverse Effect | Details |
|---|---|---|
| 1 | Severe Bronchospasm | Airway complete band ho sakti hai → respiratory failure |
| 2 | Anaphylaxis | Histamine massive release → life-threatening allergic reaction |
| 3 | Hypotension | Histamine → vasodilation → BP drop → shock |
| 4 | Bradycardia | Vagal/muscarinic stimulation → heart rate kam hona |
| 5 | Respiratory Arrest | Extreme bronchoconstriction → patient saans nahi le sakta |
| 6 | Pulmonary Hypertension | Chronic hypoxic vasoconstriction → right heart failure |
| 7 | Status Asthmaticus | Continuous severe asthma attack jo bronchodilators se nahi khuLta |
| 8 | Urinary retention | Carbachol/muscarinic agonists → bladder problems |
| 9 | Seizures (rare) | Cholinergic toxicity mein CNS involvement |
| 10 | Death | Propranolol in asthma — β₂ block → fatal bronchospasm (reported in literature) |
"Propranolol is contraindicated in patients with bronchial asthma. Death by asphyxiation has been reported." — Lippincott Illustrated Reviews: Pharmacology
8. NURSING MANAGEMENT (Nurse Ki Zimmedari)
Nurse ka kaam sirf dawai dena nahi — observe karna, rokna, aur emergency mein manage karna bhi hai.
🩺 A. Assessment (Muayana karna)
- Patient ki respiratory rate, depth, aur effort check karo
- Oxygen saturation (SpO₂) monitor karo — normal >95%
- Auscultation karo — wheezing, rhonchi sunai de rahi hai kya
- Peak Flow Meter reading lo asthma patients mein
- Patient se puchho — shortness of breath, chest tightness, cough hai kya
- Allergy history lo — kisi drug ya substance se reaction toh nahi
- Drug history lo — beta-blockers, NSAIDs, aspirin to use nahi ho rahi
- Triggers identify karo — dust, smoke, cold air, GERD, stress
🩺 B. Diagnosis (Nursing Diagnosis)
- Ineffective Airway Clearance — airway mein blockage hai
- Impaired Gas Exchange — O₂ aur CO₂ sahi se exchange nahi ho raha
- Activity Intolerance — saans ki takleef ki wajah se movement mushkil
- Anxiety — saans na aane ka darr
- Risk for Respiratory Failure — severe cases mein
🩺 C. Interventions (Kya Karna Chahiye)
Immediate Actions (Emergency mein):
- Patient ko upright (60–90°) position mein bithao — isse breathing easy hoti hai
- Oxygen therapy dena — mask/nasal cannula se O₂ dena — SpO₂ maintain karo
- Bronchodilator dena as prescribed — Salbutamol (Albuterol) nebulization sabse pehle
- IV access banao — emergency drugs dene ke liye
- Epinephrine (Adrenaline) — anaphylaxis mein 0.3–0.5 mg IM (doctor order par)
Ongoing Care:
6. Precipitating factors hataao — allergen, dhuaan, thanda paani, stress
7. Encourage deep breathing exercises — pursed lip breathing sikhao
8. Hydration maintain karo — fluids dena taki mucus thin ho aur nikal sake
9. Medications dena on time — inhaled corticosteroids, leukotriene antagonists
10. Vital signs monitor karo — har 15-30 min mein
11. Pulse oximetry lagao — continuous monitoring
12. Suction karo agar secretions zyada hain
🩺 D. Patient Education (Mareez Ko Sikhaana)
- Inhaler technique sahi se sikhao — MDI ya spacer ka use
- Triggers avoid karo: Dhuaan, dhool, cold air, pets, strong smells
- Medications kabhi band mat karo bina doctor se pooche
- Beta-blockers aur NSAIDs se bacho asthma patients mein
- GERD control karo — acid reflux asthma trigger kar sakta hai
- Action plan do — kaun se symptoms mein doctor ke paas jaana hai
- Peak flow meter use karna sikhao — apni condition monitor karne ke liye
- Stress management — deep breathing, meditation (but over-relaxation se vagal tone na badhe)
🩺 E. Evaluation (Result Check karna)
- Kya patient ki saans normal ho gayi?
- SpO₂ 95% se upar hai?
- Wheezing kam hui ya band ho gayi?
- Patient comfortable feel kar raha hai?
- Anxiety kam hui?
- Patient ne triggers avoid karna seekh liya?
📌 SUMMARY TABLE
| Topic | Key Points |
|---|---|
| Definition | Airway narrow karne wale substances |
| Main Bronchoconstrictors | Histamine, Leukotrienes, ACh, PGF₂α, Substance P |
| Mechanism | Smooth muscle contraction via receptors + Ca²⁺ release |
| Indications | Bronchial provocation test, glaucoma (carbachol) |
| Contraindications | Asthma, COPD, pregnancy, cardiac disease |
| Side Effects | Wheezing, cough, mucus, nausea, headache |
| Adverse Effects | Severe bronchospasm, anaphylaxis, respiratory arrest, death |
| Nursing Priority | Upright position + O₂ + bronchodilator + monitor SpO₂ |
References:
- Miller's Anesthesia, 10th Edition
- Katzung's Basic & Clinical Pharmacology, 16th Edition
- Lippincott Illustrated Reviews: Pharmacology
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Fishman's Pulmonary Diseases and Disorders
Yeh assignment complete hai — intro se le kar nursing management tak har ek cheez point-by-point, simple language mein cover ki gayi hai. Agar kisi bhi heading ko aur expand karna ho ya diagram chahiye ho, bata dena! 🙂
In English
📝 ASSIGNMENT
Topic: BRONCHOCONSTRICTORS
Subject: Pharmacology / Respiratory Nursing
1. INTRODUCTION
The human respiratory system is responsible for delivering oxygen to the body and removing carbon dioxide. This process depends on the airways — the bronchi and bronchioles — remaining open and clear for air to pass through freely.
Under certain conditions, the smooth muscles surrounding the airways contract, causing the airways to become narrow. This narrowing is called bronchoconstriction, and it makes breathing difficult or even impossible.
The agents responsible for causing this narrowing are called Bronchoconstrictors.
They can be:
- Natural body chemicals (released during allergic reactions or inflammation)
- Drugs (that narrow airways as a main or side effect)
- Physical triggers (cold air, smoke, stress)
Understanding bronchoconstrictors is essential for nurses because conditions like asthma, COPD, anaphylaxis, and perioperative bronchospasm are all directly linked to these agents.
Think of it this way: Airways are like a water pipe. Bronchoconstrictors are like squeezing that pipe — less air can pass through, causing breathlessness, wheezing, and chest tightness.
2. DEFINITION
Bronchoconstrictors are substances (endogenous or exogenous) that cause contraction of bronchial smooth muscle, resulting in narrowing of the airway lumen, reduced airflow, and difficulty in breathing.
Types:
| Type | Examples |
|---|---|
| Endogenous (produced inside the body) | Histamine, Leukotrienes, Acetylcholine, Prostaglandins, Bradykinin, Substance P |
| Exogenous/Pharmacological (drugs) | Beta-blockers, NSAIDs, Carbachol, Methacholine, Neostigmine |
| Physiological/Environmental | Cold air, smoke, dust, hypocapnia, acid reflux (GERD) |
3. MECHANISM OF ACTION
Different bronchoconstrictors work through different pathways. All of them, however, ultimately lead to smooth muscle contraction and airway narrowing.
🔹 A. Histamine
- During an allergic reaction, mast cells are activated and release histamine
- Histamine binds to H1 receptors on bronchial smooth muscle
- This activates Phospholipase C and Protein Kinase C (PKC)
- These enzymes trigger release of calcium (Ca²⁺) from intracellular stores
- Calcium causes smooth muscle to contract → airway narrows
- Additionally, histamine stimulates vagal afferent nerves → reflex bronchoconstriction
- The enzyme histamine N-methyltransferase in the airway epithelium helps break down histamine and provides some natural protection
Key point: Volatile anesthetics (halothane, sevoflurane, isoflurane) can inhibit histamine-induced bronchoconstriction — important in anesthesia nursing.
🔹 B. Acetylcholine (Parasympathetic/Vagal Pathway)
- A stimulus (irritant, emotion, cold air) activates the vagus nerve
- Preganglionic fibers synapse at parasympathetic ganglia in the airway wall
- Postganglionic fibers release Acetylcholine (ACh)
- ACh binds to M3 muscarinic receptors on airway smooth muscle → contraction
- ACh also binds to M1 receptors at ganglia → facilitates neurotransmission
- M2 receptors on nerve endings act as autoreceptors → try to limit further ACh release
- Net result: bronchoconstriction + increased mucus secretion
This is the dominant neural pathway for bronchoconstriction. Anticholinergic drugs (Ipratropium, Tiotropium) block M3 receptors and are used as bronchodilators.
🔹 C. Leukotrienes (LTC₄, LTD₄, LTE₄)
- Cell membranes contain arachidonic acid
- During inflammation, the enzyme 5-Lipoxygenase (5-LOX) converts it into cysteinyl leukotrienes
- Released by mast cells, eosinophils, and basophils
- Bind to CysLT1 and CysLT2 receptors on airway smooth muscle
- Cause powerful smooth muscle contraction → severe bronchoconstriction
- Additionally cause: mucus hypersecretion, mucosal edema, vascular permeability
- Are up to 1,000 times more potent than histamine
- Dominant mediators in chronic asthma
Blocked by: Montelukast, Zafirlukast (leukotriene receptor antagonists); Zileuton (5-LOX inhibitor)
🔹 D. Prostaglandins (PGF₂α, TXA₂, PGD₂)
- Also derived from arachidonic acid via the COX (Cyclooxygenase) pathway
- Released from mast cells and eosinophils
- Bind to TP, FP, and DP2 receptors on airway smooth muscle
- Cause direct smooth muscle contraction → bronchoconstriction
- NSAIDs block COX → arachidonic acid is diverted to lipoxygenase pathway → more leukotrienes → worse bronchoconstriction (this is the basis of Aspirin-Exacerbated Respiratory Disease)
PGE₂ is the exception — it causes bronchodilation, not constriction.
🔹 E. Beta-Blockers (Drug-Induced Mechanism)
- Normally, β₂ adrenergic receptors on airway smooth muscle maintain bronchodilation (relaxation)
- Non-selective beta-blockers (e.g., Propranolol) block both β₁ and β₂ receptors
- Blocking β₂ removes the bronchodilatory tone → bronchoconstriction dominates
- In asthmatic patients, this can be life-threatening
🔹 F. Substance P (Tachykinins)
- Inhaled irritants (dust, smoke, chemicals) stimulate C-fiber nerve endings in the airway
- These fibers release Substance P (a neuropeptide/tachykinin)
- Substance P directly acts on NK1/NK2 receptors on smooth muscle → contraction
- Also enhances the release of other mediators like histamine
🔹 G. Bradykinin
- Generated during inflammation and allergic reactions
- Stimulates rapidly adapting receptors in the airways
- Causes direct smooth muscle contraction and triggers vagal reflexes
- Also responsible for ACE inhibitor-induced cough and sometimes bronchospasm
4. INDICATIONS (When Are Bronchoconstrictors Used?)
Bronchoconstrictors are NOT used for therapeutic treatment. Their main clinical use is diagnostic and research-based.
| # | Indication | Drug Used | Purpose |
|---|---|---|---|
| 1 | Bronchial Provocation Test | Methacholine, Histamine | Diagnose asthma / airway hyperresponsiveness (PC₂₀ test) |
| 2 | Glaucoma | Carbachol (topical) | Reduce intraocular pressure (local use — does not affect lungs significantly) |
| 3 | Postoperative urinary retention / ileus | Bethanechol | Stimulate smooth muscle of bladder/GI tract (bronchoconstriction is an unwanted side effect) |
| 4 | Research / Laboratory studies | Carbachol, Histamine, Leukotrienes | Study airway smooth muscle physiology |
| 5 | Diagnosis of carcinoid syndrome | — | Bronchoconstriction is a clinical feature used in diagnosis |
Important: Nurses use this knowledge to manage the consequences of bronchoconstriction (e.g., asthma attack, anaphylaxis, drug reaction) rather than administer bronchoconstrictors themselves.
5. CONTRAINDICATIONS (When Should They Be Avoided?)
| # | Contraindication | Reason |
|---|---|---|
| 1 | Bronchial Asthma | Can trigger severe, potentially fatal bronchospasm |
| 2 | COPD (Chronic Obstructive Pulmonary Disease) | Already narrowed airways — further narrowing causes respiratory failure |
| 3 | Active bronchospasm | Will worsen the existing attack |
| 4 | Severe cardiovascular disease | Vagal stimulation causes bradycardia and hypotension |
| 5 | Second or third degree AV block | Adenosine and related agents are contraindicated |
| 6 | Pregnancy | PGF₂α analogs stimulate uterine contractions + risk of fetal distress |
| 7 | History of anaphylaxis | Risk of triggering massive mediator release |
| 8 | Peptic ulcer disease | Muscarinic agents (carbachol) increase gastric acid secretion |
| 9 | Urinary tract obstruction | Muscarinic agonists increase bladder pressure |
| 10 | Hypersensitivity to the agent | Allergic reaction risk |
6. SIDE EFFECTS (Common / Mild Effects)
These are expected, dose-related effects that are generally manageable:
| # | Side Effect | Cause |
|---|---|---|
| 1 | Wheezing | Airway narrowing |
| 2 | Cough | Airway irritation and mucus |
| 3 | Chest tightness | Smooth muscle contraction |
| 4 | Shortness of breath (Dyspnea) | Reduced airflow |
| 5 | Increased mucus secretion | Leukotrienes / muscarinic stimulation of submucosal glands |
| 6 | Nasal congestion | Mucosal vasodilation and edema |
| 7 | Nausea and vomiting | GI smooth muscle stimulation (muscarinic effect) |
| 8 | Diarrhea | Increased GI motility |
| 9 | Excessive salivation | Parasympathetic stimulation |
| 10 | Lacrimation (watery eyes) | Cholinergic overstimulation |
| 11 | Sweating | Cholinergic effect on sweat glands |
| 12 | Headache | Histamine-induced vasodilation |
| 13 | Flushing | Histamine vasodilation (seen in carcinoid syndrome) |
7. ADVERSE EFFECTS (Serious / Dangerous Effects)
These require immediate medical attention and nursing intervention:
| # | Adverse Effect | Details |
|---|---|---|
| 1 | Severe Bronchospasm | Complete airway closure → unable to breathe → emergency |
| 2 | Anaphylaxis | Massive histamine + mediator release → systemic allergic emergency |
| 3 | Severe Hypotension | Histamine vasodilation → cardiovascular collapse / shock |
| 4 | Bradycardia | Excessive vagal/muscarinic stimulation → heart rate dangerously low |
| 5 | Respiratory Failure | Extreme bronchoconstriction → CO₂ retention + hypoxia |
| 6 | Status Asthmaticus | Prolonged asthma attack unresponsive to bronchodilators |
| 7 | Pulmonary Hypertension | Chronic hypoxic vasoconstriction → right heart strain → right heart failure |
| 8 | Carcinoid Crisis | Severe flushing + life-threatening bronchoconstriction + hemodynamic instability |
| 9 | Urinary Retention | Muscarinic agonists → increased bladder tone + obstruction |
| 10 | Death | Propranolol given to asthmatic → complete β₂ blockade → fatal bronchospasm |
"Propranolol is contraindicated in patients with bronchial asthma. Death by asphyxiation has been reported for patients with asthma who inadvertently received the drug." — Lippincott Illustrated Reviews: Pharmacology
8. NURSING MANAGEMENT
The nurse plays a critical role in preventing, identifying, and managing bronchoconstriction. Nursing management follows the standard ADPIE framework.
🩺 A. Assessment
Respiratory Assessment:
- Assess respiratory rate, rhythm, and depth — normal 12–20 breaths/min
- Monitor oxygen saturation (SpO₂) continuously — normal >95%
- Auscultate lung sounds — listen for wheezing, crackles, or absent breath sounds
- Observe for use of accessory muscles (neck, chest, abdomen) — sign of respiratory distress
- Assess skin color — pallor or cyanosis indicates hypoxia
- Measure peak expiratory flow rate (PEFR) in asthma patients
History Taking:
7. Ask about known allergies — drugs, food, environmental
8. Review current medications — beta-blockers, NSAIDs, aspirin, cholinergic drugs
9. Identify triggers — cold air, dust, smoke, exercise, GERD, stress, animals
10. Note previous episodes — frequency, severity, hospitalizations
Vital Signs:
11. Record blood pressure — hypotension suggests anaphylaxis
12. Check heart rate — tachycardia (compensatory) or bradycardia (vagal)
13. Record temperature — infection can trigger bronchospasm
🩺 B. Nursing Diagnoses
- Ineffective Airway Clearance related to bronchospasm and excessive mucus secretion
- Impaired Gas Exchange related to narrowed airways and reduced alveolar ventilation
- Ineffective Breathing Pattern related to bronchoconstriction
- Activity Intolerance related to dyspnea and reduced oxygen availability
- Anxiety related to difficulty breathing and fear of suffocation
- Deficient Knowledge related to triggers, medications, and self-management
- Risk for Respiratory Failure in severe/uncontrolled bronchospasm
🩺 C. Planning & Interventions
🔴 Immediate / Emergency Interventions:
- Position the patient upright (60°–90°, Fowler's position) — gravity helps expand lungs and reduces work of breathing
- Administer supplemental oxygen via nasal cannula or mask — maintain SpO₂ >95%
- Administer prescribed bronchodilators immediately:
- Salbutamol (Albuterol) via nebulizer — first-line for acute bronchospasm
- Ipratropium bromide — anticholinergic bronchodilator (blocks M3 receptors)
- Establish IV access — for emergency drug administration
- Administer Epinephrine (Adrenaline) 0.3–0.5 mg IM in anaphylaxis — as per doctor's order
- Call the physician immediately if patient does not respond within minutes
- Prepare for intubation if respiratory failure is imminent
🟡 Ongoing / Supportive Care:
- Remove or eliminate the trigger — allergen, irritant, offending drug
- Administer IV corticosteroids as ordered — reduce airway inflammation
- Encourage pursed-lip breathing and controlled breathing techniques
- Ensure adequate hydration — oral or IV fluids thin the mucus secretions
- Perform chest physiotherapy / suction if secretions are blocking airways
- Monitor vital signs every 15–30 minutes during acute episode
- Attach pulse oximetry for continuous SpO₂ monitoring
- Reassure the patient — anxiety worsens bronchospasm by increasing respiratory rate
🩺 D. Patient & Family Education
- Teach correct inhaler technique — MDI with spacer or dry powder inhaler (DPI)
- Educate about triggers and how to avoid them:
- No smoking (active or passive)
- Avoid dust, pollen, animal dander, strong perfumes
- Avoid cold and dry air — use a scarf over mouth in winter
- Control GERD — eat small meals, avoid lying flat after eating
- Never stop medications suddenly — especially inhaled corticosteroids
- Avoid beta-blockers and NSAIDs/aspirin unless specifically approved by doctor
- Teach use of Peak Flow Meter — to monitor airway status at home daily
- Provide written Asthma Action Plan:
- Green zone (>80% peak flow) = routine medications
- Yellow zone (50–80%) = increase bronchodilator + call doctor
- Red zone (<50%) = emergency — go to hospital immediately
- Stress management — teach relaxation techniques carefully (note: excessive vagal activation can worsen bronchoconstriction)
- Regular follow-up — emphasize importance of scheduled clinic visits
🩺 E. Evaluation (Outcome Criteria)
The nursing interventions are considered successful when:
- ✅ Patient's SpO₂ returns to ≥95%
- ✅ Respiratory rate normalizes (12–20 breaths/min)
- ✅ Wheezing and chest tightness resolved or significantly reduced
- ✅ Patient able to speak in full sentences without breathlessness
- ✅ Peak flow returns to ≥80% of personal best
- ✅ Patient is calm and not anxious
- ✅ Patient can correctly demonstrate inhaler use
- ✅ Patient can identify personal triggers and explain how to avoid them
📌 QUICK SUMMARY TABLE
| Heading | Key Points |
|---|---|
| Definition | Substances causing airway smooth muscle contraction → narrowing |
| Main Bronchoconstrictors | Histamine, Leukotrienes (LTC₄/LTD₄/LTE₄), Acetylcholine, PGF₂α, TXA₂, Substance P, Bradykinin |
| Mechanism | Receptor binding → Ca²⁺ release → smooth muscle contraction → airway narrowing |
| Indications | Bronchial provocation test (methacholine/histamine), glaucoma (carbachol) |
| Contraindications | Asthma, COPD, active bronchospasm, cardiac disease, pregnancy |
| Side Effects | Wheezing, cough, mucus, nausea, sweating, headache |
| Adverse Effects | Severe bronchospasm, anaphylaxis, respiratory failure, status asthmaticus, death |
| Top Nursing Priority | Upright position + O₂ + bronchodilator + continuous SpO₂ monitoring |
References:
- Miller's Anesthesia, 10th Edition
- Katzung's Basic & Clinical Pharmacology, 16th Edition
- Lippincott Illustrated Reviews: Pharmacology
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Fishman's Pulmonary Diseases and Disorders
- Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.