Presentation for this case study in class.
Reading File
search_medical_text
acute pyelonephritis diagnosis clinical features management antibiotics
search_medical_image
acute pyelonephritis renal ultrasound pathology
GradeResponse
GradeResponse
Here is a complete, structured presentation you can use in class:
Case 1 – Acute Pyelonephritis
Role: Diagnosing Doctor
1. Patient Introduction
| Parameter | Finding |
|---|---|
| Age / Sex | 22-year-old female |
| Setting | Outpatient clinic |
| Chief complaints | High fever, chills, severe right lumbar pain |
| Duration | 2 days |
2. History of Present Illness
Systemic symptoms:
- Fever 39.2 °C, sudden onset
- Shaking chills, profuse sweating
- Nausea, complete loss of appetite
Urinary symptoms:
- Dysuria (burning sensation during micturition)
- Frequency
Pain characteristics:
- Right flank — constant, worsened by movement, non-radiating
- Non-radiating pain helps distinguish this from ureteral colic (which typically radiates to the groin)
3. Physical Examination
| Finding | Value / Result |
|---|---|
| General appearance | Acutely ill |
| Heart rate | 110 bpm (tachycardia) |
| Blood pressure | 115/70 mmHg |
| Respiratory rate | 20 breaths/min |
| Right CVA tenderness | Marked |
| Pasternatsky's sign | Positive (percussion reproduces pain) |
| Left kidney | Non-tender |
| Suprapubic tenderness | Absent |
| Lungs | Clear |
Key sign — Pasternatsky's sign: fist percussion over the costovertebral angle reproduces flank pain. Positive in renal parenchymal involvement (pyelonephritis, renal abscess). Absent suprapubic tenderness helps rule out a primary bladder pathology.
4. Differential Diagnosis
| Diagnosis | Supporting features | Against |
|---|---|---|
| Acute pyelonephritis | Fever, CVA tenderness, dysuria, frequency | — |
| Urolithiasis with obstruction | Flank pain, nausea | Pain usually colicky & radiates; no fever expected unless infected |
| Lower UTI (cystitis) | Dysuria, frequency | No fever, no CVA tenderness expected in isolated cystitis |
5. Investigations Ordered
Rationale: to confirm upper vs. lower tract infection, identify causative organism, and rule out obstruction/abscess.
- Complete blood count (CBC)
- C-reactive protein (CRP)
- Procalcitonin
- Urinalysis
- Urine culture + antibiotic susceptibility testing
- Renal ultrasound
6. Results Summary
Lab Results
| Test | Result | Interpretation |
|---|---|---|
| WBC | 15 × 10⁹/L | Leukocytosis — active bacterial infection |
| CRP | 120 mg/L | Markedly elevated — significant inflammation |
| Procalcitonin | 0.15 ng/mL | Normal — no systemic sepsis/bacteremia |
| Urine WBC | 40–50 /HPF | Pyuria — hallmark of UTI |
| Urine nitrites | Moderate | Gram-negative bacteriuria (e.g., E. coli) |
| Urine protein | 0.33 g/L (trace) | Mild — reactive, not nephrotic |
| Urine bacteria | Numerous | — |
| Urine culture | E. coli >10⁵ CFU/mL | Confirmed causative organism |
| Susceptibility | Sensitive to ceftriaxone | Guides definitive therapy |
Normal procalcitonin (0.15 ng/mL) is an important finding — it suggests the infection is localized to the kidney without bacteremia or sepsis, supporting uncomplicated pyelonephritis.
Renal Ultrasound
Finding: Diffuse thickening of right renal parenchyma with preserved corticomedullary differentiation; no hydronephrosis, no calculi.
This is what ultrasound findings in acute pyelonephritis can look like:
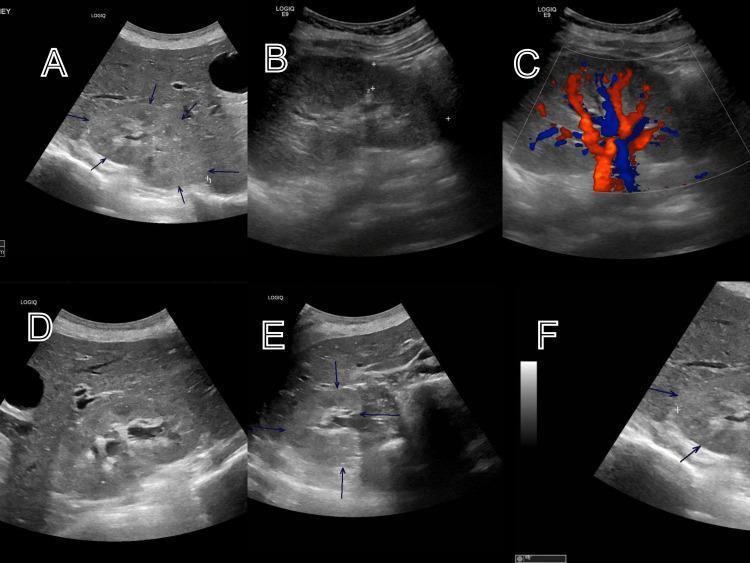
Ultrasound panels showing classic sonographic markers of renal infection: parenchymal echogenicity changes, mild enlargement, increased Doppler flow, and perirenal edema.
The absence of hydronephrosis rules out obstructive uropathy, and no calculi rules out urolithiasis as the primary cause.
7. Final Diagnosis
Acute uncomplicated pyelonephritis (right kidney) Causative organism: Escherichia coli >10⁵ CFU/mL
Criteria met:
- Upper UTI symptoms (fever, CVA tenderness) + lower UTI symptoms (dysuria, frequency)
- Pyuria + bacteriuria on urinalysis
- Positive urine culture
- Ultrasound: renal parenchymal changes, no obstruction
8. Management
Inpatient Phase
| Intervention | Detail |
|---|---|
| Empiric antibiotics | Ceftriaxone 1 g IV twice daily |
| Antibiogram review | Same agent continued (susceptible) |
| IV fluids | 0.9% saline — rehydration |
| Antipyretic | Acetaminophen |
| Oral hydration | Encouraged |
Why ceftriaxone? It is a 3rd-generation cephalosporin with excellent gram-negative coverage, good renal tissue penetration, and reliable activity against E. coli. Per guidelines (Recurrent UTI in Adult Women, p. 8), nitrofurantoin and fosfomycin are not appropriate for pyelonephritis (inadequate tissue levels), and TMP-SMX is avoided empirically due to high resistance rates.
Response & Step-Down
- Clinical improvement within 48 hours (fever resolved, pain decreased, tolerating oral intake)
- Completed 7-day IV ceftriaxone course
- Discharged on oral cefixime × 3 days (step-down therapy)
9. Follow-Up Plan
| Timepoint | Action |
|---|---|
| 2 weeks post-discharge | Control urinalysis |
| 1 month post-discharge | Repeat renal ultrasound |
Patient education:
- Complete the full antibiotic course
- Maintain adequate hydration
- Avoid hypothermia
- Evaluate for chronic infectious foci (dental, tonsillar)
- Seek early medical attention if symptoms recur
10. Key Teaching Points
- Pyelonephritis = upper UTI — distinguished from cystitis by systemic signs (fever, chills) and costovertebral angle tenderness.
- Positive Pasternatsky's sign is a bedside clue pointing to renal parenchymal involvement.
- Normal procalcitonin in the setting of elevated CRP and WBC suggests localized (not systemic/septic) infection.
- E. coli is the most common causative organism in community-acquired pyelonephritis.
- Ultrasound is used to rule out obstruction and abscess — not to confirm pyelonephritis per se.
- Nitrofurantoin and fosfomycin are contraindicated in pyelonephritis — they do not achieve adequate renal tissue concentrations.
- Step-down from IV to oral is appropriate once the patient is afebrile and tolerating oral intake.
This covers the full arc from presentation through discharge. Good luck with your class!
This is a shared conversation. Sign in to Orris to start your own chat.