Blood supply of heart
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I have comprehensive data from authoritative textbooks. Now I'll compose the full answer:
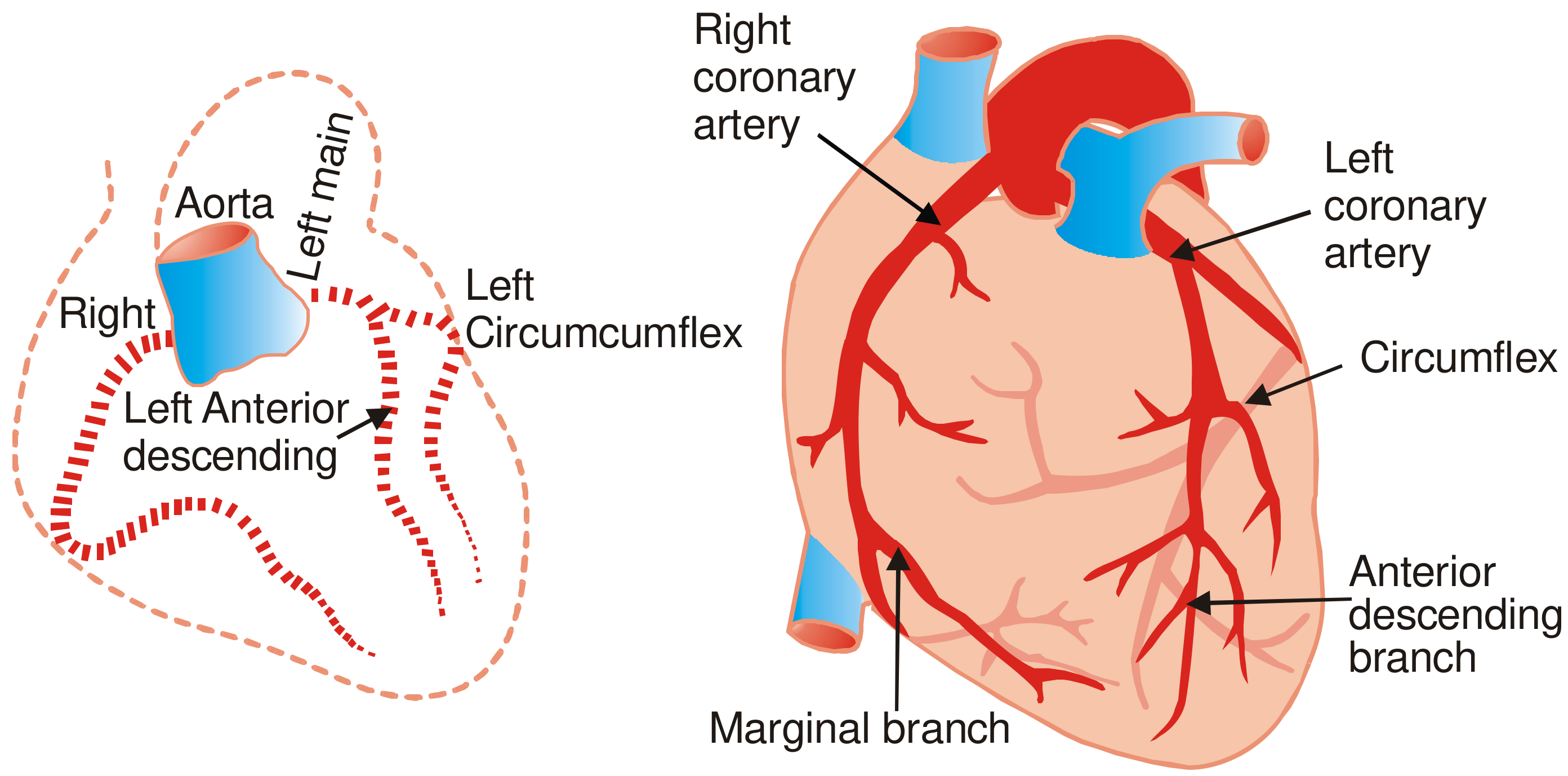
Blood Supply of the Heart
The heart receives its entire arterial supply from the right and left coronary arteries, which arise from the ascending aorta just above the aortic valve (from the right and left aortic sinuses of Valsalva). Blood flows from epicardial to endocardial vessels. Venous return goes primarily through the coronary sinus into the right atrium.
Arterial Supply
Diagrams
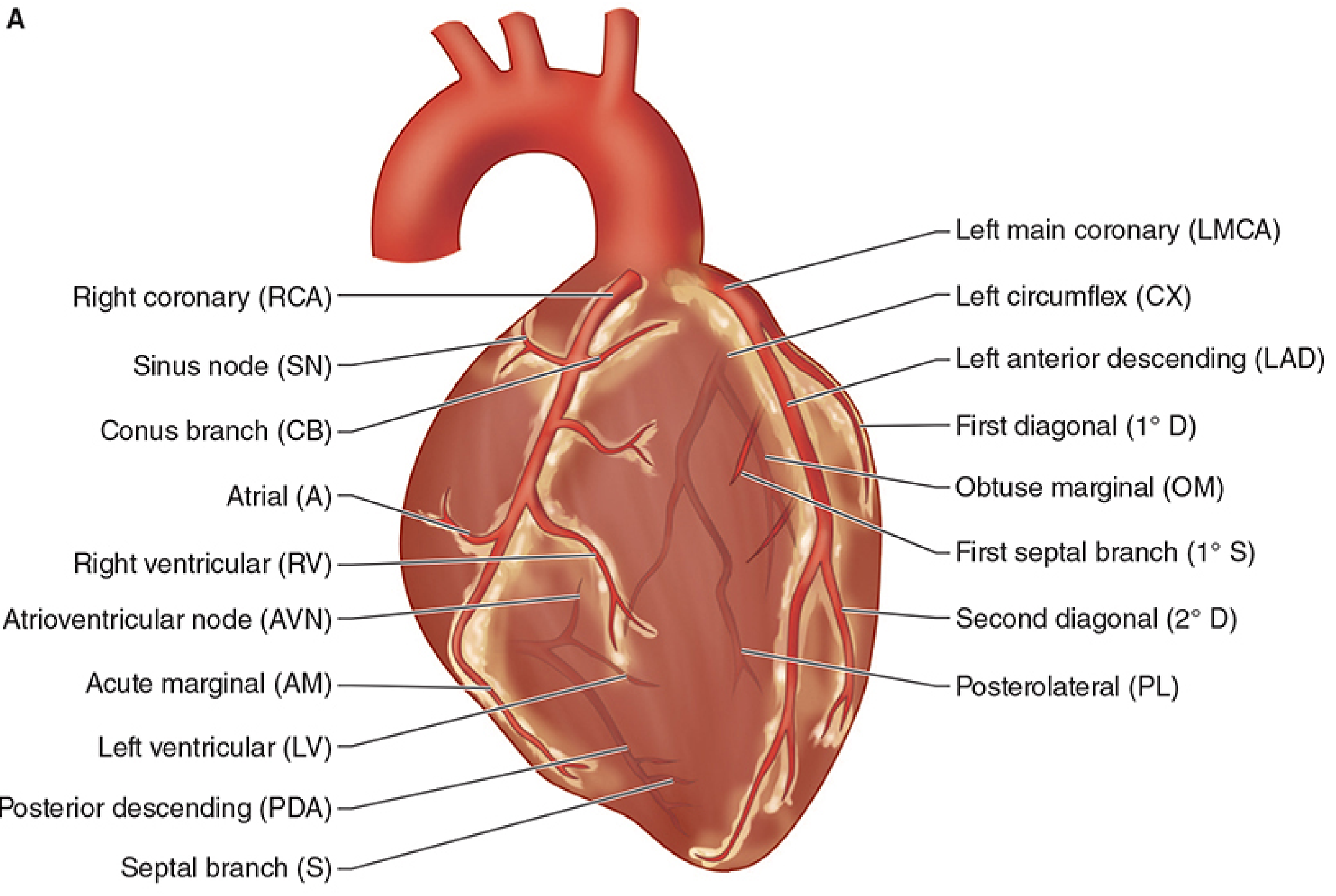
1. Right Coronary Artery (RCA)
- Arises from the right aortic sinus of the ascending aorta
- Passes anteriorly, then descends in the right atrioventricular (coronary) sulcus between the right atrium and right ventricle
- Continues posteriorly onto the diaphragmatic surface and base of the heart
Branches of the RCA:
| Branch | Supply |
|---|---|
| SA nodal branch | Early atrial branch; passes posteriorly around SVC to supply the sinoatrial node (60% of individuals) |
| Conus branch | Supplies the infundibulum (outflow tract) of the right ventricle |
| Right atrial branches | Right atrium |
| Right marginal branch (acute marginal) | Runs along the inferior (acute) margin to the apex; supplies the anterior surface of the right ventricle |
| AV nodal branch | Small branch to the atrioventricular node before the terminal branch |
| Posterior descending artery (PDA) / Posterior interventricular branch | Lies in the posterior interventricular sulcus; supplies the posterior third of the interventricular septum, the inferior wall |
Territories supplied by RCA:
- Right atrium and right ventricle
- SA node (60%) and AV node (85-90%)
- Interatrial septum
- A portion of the left atrium
- Posteroinferior one-third of the interventricular septum
- Inferior and posterior wall of the left ventricle
2. Left Coronary Artery (LCA)
- Arises from the left aortic sinus of the ascending aorta
- Passes between the pulmonary trunk and the left auricle
- After a short course (left main stem, ~1-2 cm), it bifurcates into two major branches:
a) Left Anterior Descending (LAD) / Anterior Interventricular Artery
- Descends in the anterior interventricular sulcus toward the apex
- Wraps around the apex in most individuals to reach the inferior interventricular sulcus
| Branch | Supply |
|---|---|
| Septal perforating branches | Anterior 2/3 of interventricular septum; bundle of His |
| Diagonal branches | Anterior and lateral walls of LV |
| First diagonal | Supplies anterior papillary muscle of mitral valve (dual supply with CX) |
Territory: Anterior wall of LV, anterior 2/3 of interventricular septum, apex
b) Left Circumflex Artery (CX / LCx)
- Curves in the left atrioventricular sulcus around the left side of the heart
| Branch | Supply |
|---|---|
| Obtuse marginal branches | Lateral wall of LV |
| Left atrial branches | Left atrium |
| SA nodal branch | In ~40% of individuals |
| AV nodal branch | In 10-15% (when not RCA-dominant) |
Territory: Left atrium, lateral wall of LV, posterolateral LV
Dominance
Coronary dominance is determined by which artery gives rise to the posterior descending artery (PDA):
| Type | Prevalence | PDA from |
|---|---|---|
| Right dominant | ~85% | RCA |
| Left dominant | ~8-10% | Circumflex (LCx) |
| Co-dominant / balanced | ~5-7% | Both RCA and LCx |
In right dominant circulation, the RCA gives rise to the PDA, supplying the posterior septum and inferior LV wall. In left dominant circulation, the CX wraps around the AV groove and continues as the PDA, supplying most of the posterior septum and inferior wall.
Blood Supply to Conducting System
| Structure | Primary supply | Secondary supply |
|---|---|---|
| SA node | RCA (60%) | LAD (40%) |
| AV node | RCA (85-90%) | LCx (10-15%) |
| Bundle of His | PDA + LAD (dual) | - |
| Left bundle branch | LAD (septal perforators) | PDA |
| Right bundle branch | LAD | - |
| Anterior papillary muscle (mitral) | LAD diagonal + CX marginal (dual) | - |
| Posterior papillary muscle (mitral) | PDA only | - (vulnerable to ischemia!) |
The posterior papillary muscle, supplied only by the PDA, is particularly vulnerable to ischemic dysfunction.
Venous Drainage
Blood returns to the right atrium via three routes:
-
Coronary sinus - the main channel; located in the coronary sulcus on the posterior surface; receives most of the cardiac venous drainage; empties into the right atrium between the IVC opening and the right AV orifice
- Great cardiac vein - runs with the LAD in the anterior interventricular sulcus
- Middle cardiac vein - runs with the PDA in the posterior interventricular sulcus
- Small cardiac vein - runs with the right marginal artery
- Left marginal vein / Oblique vein of Marshall - drains the left atrium and posterior LV
-
Anterior cardiac veins - drain directly into the right atrium (2-3 small veins from the anterior RV surface)
-
Thebesian veins (venae cordis minimae) - tiny veins that drain small amounts of blood directly into all chambers of the heart
Clinical Correlates
- LAD occlusion ("widow maker") - most common site of fatal MI; causes anterior STEMI, septal and apical infarction
- RCA occlusion - inferior STEMI; may involve SA and AV nodes causing arrhythmias (bradycardia, heart blocks)
- Frequency of fatal coronary stenosis (P.C. Dikshit, Forensic Medicine): Anterior interventricular (LAD) 45-64% > Right main coronary 24-46% > Left circumflex 3-10% > Left main 0-10%
- Referred pain (T1-T4): Visceral afferents follow sympathetic fibers entering the spinal cord at T1-T4, producing referred pain to the chest, left arm, jaw, and shoulder
- CABG uses the great saphenous vein, internal thoracic artery, or radial artery as bypass grafts
Sources: Gray's Anatomy for Students; Morgan & Mikhail's Clinical Anesthesiology, 7e; P.C. Dikshit Textbook of Forensic Medicine and Toxicology; Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.