Clinical anatomy. physiology of the pharyns, Pharyngeal spaces. Acutediseases of the pharynx (primary and secondary angina). Peritonsillar abscess.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have sufficient material to compose a comprehensive, well-structured answer.
Clinical Anatomy & Physiology of the Pharynx, Pharyngeal Spaces, and Acute Pharyngeal Diseases
1. Clinical Anatomy of the Pharynx
The pharynx is a musculofascial half-cylinder that links the oral and nasal cavities in the head to the larynx and esophagus in the neck. It is a common pathway for both air and food. It attaches superiorly to the base of the skull and is continuous inferiorly with the esophagus at the level of vertebra C6. The two sides are united posteriorly in the midline by the pharyngeal raphe, which descends from the pharyngeal tubercle of the occipital bone.
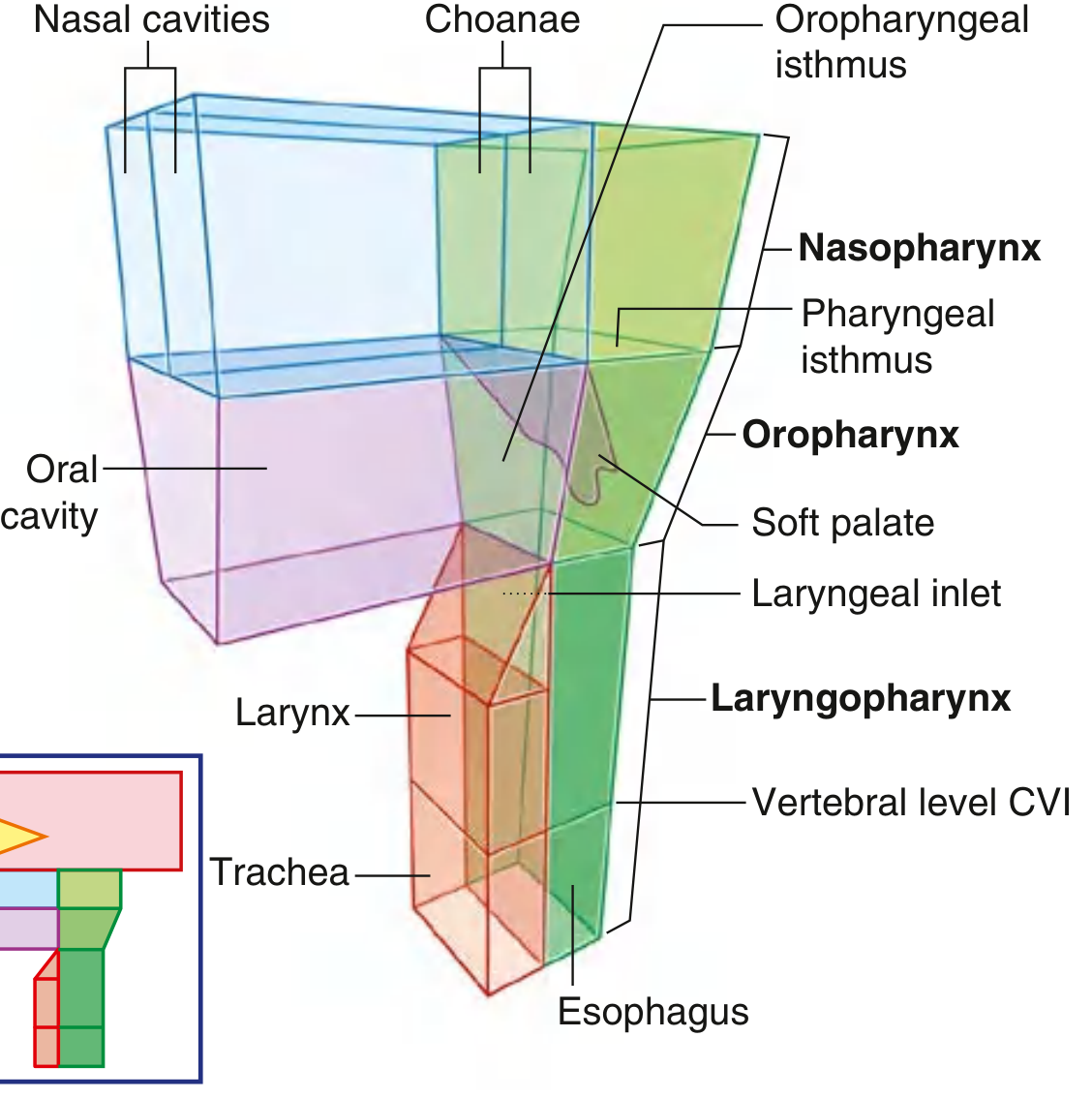
Subdivisions
| Region | Anterior Relationship | Key Structures |
|---|---|---|
| Nasopharynx | Choanae of nasal cavities | Adenoid (pharyngeal tonsil), opening of Eustachian tube (torus tubarius), fossa of Rosenmüller |
| Oropharynx | Oropharyngeal isthmus | Palatine tonsils, posterior 1/3 of tongue (lingual tonsil), soft palate, posterior pharyngeal wall |
| Laryngopharynx (hypopharynx) | Laryngeal inlet | Pyriform sinuses, post-cricoid region, posterior pharyngeal wall; continues to esophagus at C6 |
Muscular Wall
The pharyngeal wall consists of an outer circular layer (the constrictors) and an inner longitudinal layer:
- Constrictor muscles (three overlapping constrictor muscles):
- Superior constrictor — arises from the pterygomandibular raphe and medial pterygoid plate; forms the lateral wall of the oropharynx and is directly lateral to the palatine tonsil
- Middle constrictor — arises from the hyoid bone
- Inferior constrictor — arises from the thyroid and cricoid cartilages; its lowest fibers (cricopharyngeus) form the upper esophageal sphincter
- Longitudinal muscles: stylopharyngeus (CN IX), palatopharyngeus, salpingopharyngeus — these elevate the pharynx and larynx during swallowing
Nerve Supply
- Motor: pharyngeal plexus (CN IX, X) — all muscles except stylopharyngeus (CN IX alone)
- Sensory: nasopharynx — CN V2; oropharynx — CN IX (glossopharyngeal); hypopharynx — CN X (internal laryngeal branch)
Blood Supply
- Ascending pharyngeal artery (branch of external carotid), tonsillar branch of facial artery, dorsal lingual artery, greater palatine artery
Lymphoid Ring (Waldeyer's Ring)
A ring of lymphoid tissue surrounding the pharyngeal inlet, comprising:
- Pharyngeal tonsil (adenoid) — nasopharynx roof
- Tubal tonsils — around Eustachian tube openings
- Palatine tonsils (the "tonsils") — tonsillar fossae of oropharynx
- Lingual tonsils — posterior tongue base
2. Physiology of the Pharynx
The pharynx serves three major physiological functions:
Deglutition (Swallowing)
The pharyngeal phase of swallowing is rapid (~1 second) and involuntary:
- The soft palate elevates (levator veli palatini) to close the pharyngeal isthmus, sealing off the nasopharynx and preventing nasopharyngeal regurgitation
- The pharyngeal constrictors contract in a sequential superoinferior wave, propelling the bolus
- The larynx is elevated (longitudinal muscles), the epiglottis deflects posteriorly, and the vocal folds adduct to protect the airway
- The cricopharyngeus (UES) relaxes to allow entry of the bolus into the esophagus
Respiratory Function
The pharynx is the shared aerodigestive passage; the soft palate acts as a "flutter valve" — it swings up to seal the nasopharynx from the oropharynx (during swallowing) and down to seal the oropharynx from the oral cavity.
Phonation & Resonance
The pharyngeal cavity acts as a resonating chamber for voice. Velopharyngeal closure (soft palate against posterior pharyngeal wall) is essential for non-nasal speech sounds.
Eustachian Tube Regulation
The nasopharynx contains the pharyngeal openings of the Eustachian tubes; the salpingopharyngeus and tensor veli palatini regulate middle ear pressure equalization during swallowing and yawning.
3. Pharyngeal Spaces
The pharynx is surrounded by several fascially defined potential spaces that are clinically important as routes for spread of infection.
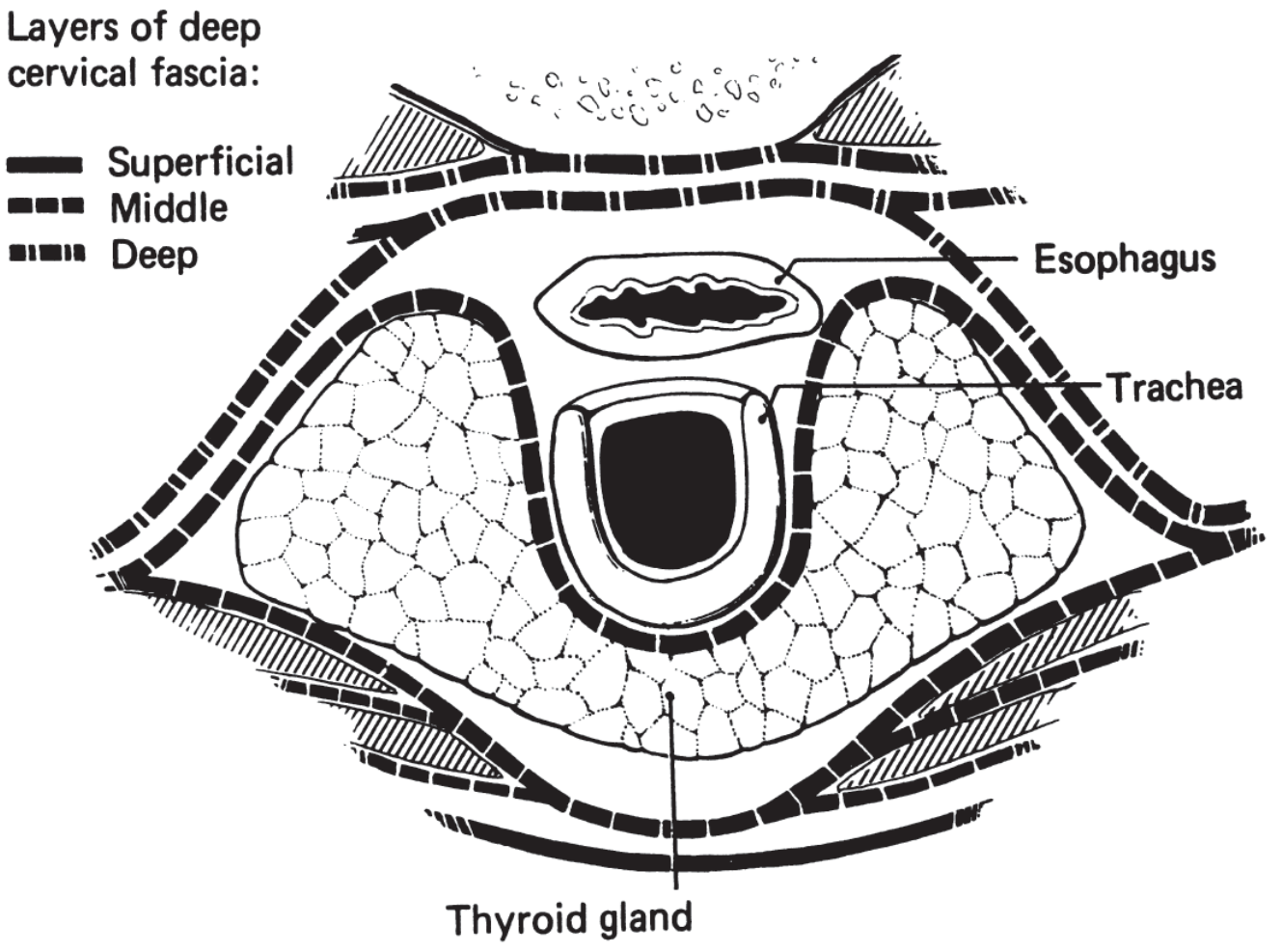
Key Deep Neck Spaces
| Space | Boundaries | Contents | Communicates With |
|---|---|---|---|
| Peritonsillar | Medial: palatine tonsil; Lateral: superior constrictor | Loose connective tissue; tonsillar branches of lingual, facial, ascending pharyngeal vessels | Parapharyngeal |
| Parapharyngeal | Superior: middle cranial fossa base; Inferior: hyoid; Anterior: pterygomandibular raphe; Posterior: prevertebral fascia; Medial: superior constrictor; Lateral: deep lobe of parotid + medial pterygoid | Fat, lymph nodes, internal maxillary artery, auriculotemporal/lingual/inferior alveolar nerves, deep lobe parotid, internal carotid, internal jugular, CN IX–XII, superior cervical sympathetic | Peritonsillar, submandibular, visceral, retropharyngeal, carotid, masticator, parotid spaces |
| Retropharyngeal | Between posterior visceral fascia (buccopharyngeal) and alar fascia; extends from skull base to T1–T2 | Loose connective tissue, lymph nodes of Rouvière (present in children <5 yr) | Danger space, mediastinum (allows inferior spread) |
| Submandibular | Superior: floor of mouth mucosa; Inferior: digastric; divided by mylohyoid into sublingual (superior) and submaxillary (inferior) compartments | Submandibular gland, Wharton duct, lingual nerve, hypoglossal nerve, facial vessels | Parapharyngeal, sublingual |
The parapharyngeal space is the central crossroads — virtually all deep neck spaces communicate with it, making it the key space for spread of infection from peritonsillar, dental, and pharyngeal sources.
4. Acute Diseases of the Pharynx
4A. Primary Angina (Acute Tonsillitis / Pharyngitis)
"Primary angina" refers to acute inflammation of the tonsils and/or pharynx as the primary (de novo) disease process, not secondary to systemic illness.
Acute Pharyngotonsillitis
Etiology:
- Most common: Group A beta-hemolytic Streptococcus (GABHS) — Streptococcus pyogenes
- Viral: adenovirus (most common overall cause of pharyngitis), EBV (infectious mononucleosis), HSV, parainfluenza, rhinovirus
- Other bacterial: Staphylococcus aureus, Haemophilus influenzae, Fusobacterium necrophorum
Clinical features:
- Sore throat, odynophagia, fever (often >38.5°C)
- Tonsillar erythema and exudate (follicular or membranous)
- Tender cervical lymphadenopathy (jugulodigastric nodes)
- Uvular erythema and edema
Centor/McIsaac criteria for GABHS (1 point each):
- Tonsillar exudate
- Tender anterior cervical lymphadenopathy
- Fever (history or measured)
- Absence of cough (+1 for age <15; −1 for age >45)
Diagnosis: Rapid strep antigen test; throat culture (gold standard)
Treatment:
- Bacterial: Penicillin V or amoxicillin × 10 days (first-line); clindamycin or azithromycin in penicillin allergy
- Symptomatic: NSAIDs, corticosteroids (single-dose dexamethasone reduces duration of pain)
- Viral: supportive care
Acute Follicular vs. Lacunar Tonsillitis
- Follicular: white-yellow spots at tonsillar crypts (purulent follicles)
- Lacunar: coalescing exudate covering tonsillar surface within crypts (lacunae)
- Phlegmonous (parenchymal): diffuse tonsillar infiltration — precursor to abscess
4B. Secondary Angina
"Secondary angina" describes tonsillopharyngeal inflammation as a manifestation of a systemic disease — the tonsils/pharynx are involved secondarily.
Key causes:
| Disease | Characteristic Features |
|---|---|
| Infectious mononucleosis (EBV) | Severe membranous tonsillitis, posterior cervical lymphadenopathy, hepatosplenomegaly, heterophile antibodies (Monospot), atypical lymphocytes; treat with corticosteroids — avoid ampicillin (maculopapular rash) |
| Agranulocytosis (drug-induced, hematological) | Necrotic/ulcerated tonsils without suppuration, high fever, no pus; neutropenia on CBC; treat underlying cause |
| Diphtheria (Corynebacterium diphtheriae) | Tough grey-white pseudomembrane extending beyond tonsil margins (bleeds on removal), bull-neck lymphadenopathy, toxin-mediated myocarditis and neuropathy; treat with antitoxin + penicillin/erythromycin |
| Vincent's angina (acute necrotizing ulcerative tonsillitis) | Mixed fusospirochetal infection (Fusobacterium + Borrelia vincenti); unilateral necrotic ulcer with grayish membrane, foul odor, no significant fever; treat with penicillin + metronidazole |
| Scarlet fever | GABHS pharyngitis + sandpaper rash, strawberry tongue, Pastia lines |
| Leukemia/lymphoma | Tonsillar enlargement with ulceration; pancytopenia; bone marrow biopsy |
| Syphilis | Painless ulcer (primary chancre on tonsil) or mucous patch (secondary) |
5. Peritonsillar Abscess
Peritonsillar abscess (PTA) is the most common deep neck space infection in adults and represents the most frequent complication of acute tonsillitis.
Pathophysiology
PTA is a purulent infection of the Weber glands (minor salivary glands) in the potential space between the tonsil capsule and the superior constrictor muscle. It most commonly forms in the superior pole of the peritonsillar space. It usually follows an episode of acute tonsillitis but can arise de novo.
Microbiology: polymicrobial — aerobic (Streptococcus pyogenes, Staphylococcus aureus, H. influenzae) and anaerobic (Fusobacterium, Prevotella, Peptostreptococcus) organisms.
Clinical Features
- Trismus — the hallmark sign (spasm of pterygoid muscles due to proximity of superior constrictor; best single clinical indicator)
- Severe unilateral throat pain, often with referred otalgia (via CN IX/X)
- "Hot potato" (muffled) voice — velopharyngeal dysfunction from soft palate swelling
- Dysphagia and drooling
- High fever, malaise
- Uvular deviation to the contralateral side
- Unilateral peritonsillar bulge with displacement of the tonsil medially and inferiorly
- Ipsilateral jugulodigastric lymphadenopathy
Diagnosis
- Clinical in most cases
- Needle aspiration — both diagnostic and therapeutic; pus confirms abscess vs. cellulitis (peritonsillar cellulitis does not yield pus)
- CT scan of neck with contrast — not routinely required but indicated if: clinical picture is unclear, spread to parapharyngeal/retropharyngeal space is suspected, or patient cannot open mouth for examination. CT distinguishes abscess (rim-enhancing fluid collection) from phlegmon.
Treatment
- Drainage — mainstay of treatment:
- Needle aspiration (office procedure, high success rate)
- Incision and drainage (I&D) under local anesthesia
- Quinsy tonsillectomy (tonsillectomy during acute infection — used when I&D fails or severe trismus)
- Intravenous antibiotics — broad-spectrum covering streptococci and anaerobes (e.g., ampicillin-sulbactam, or penicillin + metronidazole); clindamycin for penicillin allergy
- Corticosteroids (IV dexamethasone) — reduce inflammation, pain, and trismus; shorten hospital stay
- Hydration and analgesia
Recurrence rate: ~17%. Tonsillectomy is recommended after a second episode of PTA, or in children with recurrent tonsillitis.
Complications
| Complication | Mechanism |
|---|---|
| Parapharyngeal abscess | Rupture of PTA through superior constrictor into parapharyngeal space |
| Retropharyngeal abscess | Further posterior spread |
| Mediastinitis | Inferior spread via retropharyngeal/danger space — life-threatening |
| Airway obstruction | Progressive swelling displacing tongue base; emergency |
| Jugular vein thrombophlebitis | Lemierre syndrome (Fusobacterium necrophorum septic thrombophlebitis of internal jugular vein) |
| Carotid artery erosion / pseudoaneurysm | Rare, catastrophic |
| Aspiration pneumonia | Abscess rupture |
| Endocarditis / septicemia | Bacteremia |
| Nephritis | Streptococcal antigen-mediated |
Summary Table: Acute Pharyngeal Diseases
| Condition | Key Organism | Hallmark Feature | Treatment |
|---|---|---|---|
| Streptococcal tonsillitis | GABHS | Exudate, tender LN, no cough | Penicillin V × 10 days |
| Infectious mononucleosis | EBV | Membranous tonsillitis + splenomegaly | Supportive; steroids; avoid ampicillin |
| Diphtheria | C. diphtheriae | Grey pseudomembrane beyond tonsil margin | Antitoxin + antibiotic |
| Vincent's angina | Fusobacterium + spirochetes | Unilateral necrotic ulcer, foul odor | Penicillin + metronidazole |
| Agranulocytosis | — (secondary) | Necrotic tonsils, no pus, severe neutropenia | Treat underlying cause |
| Peritonsillar abscess | Polymicrobial | Trismus + uvular deviation + muffled voice | Drain + IV antibiotics ± steroids |
Sources: Gray's Anatomy for Students (Elsevier, 2023); K.J. Lee's Essential Otolaryngology, 11e; Cummings Otolaryngology Head and Neck Surgery, 7e
This is a shared conversation. Sign in to Orris to start your own chat.