C section
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information from two authoritative textbooks. Here's a thorough summary:
Cesarean Section (C-Section): Indications & Contraindications
Definition
Cesarean section is the operative delivery of an infant, usually performed to decrease the risk of perinatal morbidity and mortality. The term derives from the Latin caedere ("to cut"). In the United States, C-sections currently account for approximately 15–35% of all deliveries (varying by institution).
Indications
Maternal Indications
| Category | Examples |
|---|---|
| Prior uterine surgery | Repeat cesarean (patient declines/fails trial of labor); prior classical uterine incision (vertical); previous extensive myomectomy or uterine reconstruction |
| Hemorrhage / placenta | Placenta previa (central or partial); placental abruption; antepartum hemorrhage |
| Pelvic/anatomic obstruction | Contracted pelvis / cephalopelvic disproportion; obstructive pelvic, vaginal, or vulvar tumors or condylomata; cervical cancer |
| Hypertensive disorders | Severe hypertension or severe preeclampsia |
| Labor failure | Maternal exhaustion; arrest of labor; failed postdates induction; dysfunctional uterine activity |
| Infection | Active maternal herpes simplex genital infection with ruptured membranes |
| Other | Maternal thrombocytopenia; labor intolerance from medical disease; uterine rupture; previous vaginal reconstruction |
Fetal Indications
| Category | Examples |
|---|---|
| Malpresentation | Breech presentation; transverse or oblique lie; brow or face presentation |
| Fetal distress | Nonreassuring fetal heart rate; umbilical cord prolapse with fetal bradycardia |
| Fetopelvic relations | Fetopelvic disproportion; abnormal fetopelvic relations |
| Failed instrumental delivery | Failed trial of forceps or vacuum; deep transverse arrest |
| Special fetal conditions | Very low birth weight (<1,500 g); macrosomia (estimated fetal weight >4,500 g, or >4,000 g in a diabetic mother); multiple gestation with nonvertex first twin |
| Maternal infection risk to fetus | Maternal HIV infection |
| Other | Certain fetal anomalies |
Emergency / Urgent Indications
- Fetal distress
- Umbilical cord prolapse with fetal bradycardia
- Maternal hemorrhage
- Impending maternal death
- Perimortem cesarean
- Uterine rupture
Contraindications
There are no absolute contraindications to cesarean section. Because it is considered a life-saving procedure in many circumstances, the only recognized absolute contraindication is patient refusal after the consequences have been clearly explained and accepted by the mother.
Relative contraindications include:
- A breech or other fetal indication when vaginal delivery is safely feasible
- Situations where vaginal delivery carries less risk to mother or fetus (e.g., pulmonary arterial hypertension — cesarean may actually increase the risk of VTE and other medical complications in PAH patients compared to vaginal delivery)
Vaginal birth after cesarean (VBAC) is not a contraindication to cesarean in subsequent pregnancies, though previous low transverse cesarean is also not a contraindication to attempted vaginal birth.
Sources:
- Pfenninger and Fowler's Procedures for Primary Care, 3rd ed. — Ch. Cesarean Section, pp. 1133–1135
- Morgan and Mikhail's Clinical Anesthesiology, 7th ed. — Table 41–4, p. 1625
Explain me other points also
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a complete overview of the remaining aspects of cesarean section:
Cesarean Section — Complete Overview
2. Types of Uterine Incisions
There are three main types:
| Incision | Advantages | Disadvantages |
|---|---|---|
| Low Transverse (Kerr) — >90% of all C-sections | Lower uterine segment is thin and less vascular; heals well; least risk of future dehiscence | Risk of lateral extension into uterine vessels |
| Low Vertical (Krönig) | Useful if lower uterine segment is thick or has fibroids; preferred for transverse lie (back down) or fetal anomalies like hydrocephalus | Requires greater bladder separation; mandates repeat C-section if upper segment entered |
| Classic (Midline Vertical) | Fastest; best exposure; suitable for true emergencies | Greater blood loss; difficult 3-layer repair; 8× greater risk of dehiscence; increased rupture risk in subsequent pregnancies |
3. Surgical Technique (Low Transverse / Pfannenstiel)
Step-by-step:
- Positioning: Left lateral tilt (wedge or table tilt) to improve venous return and fetal oxygenation.
- Anesthesia: Regional (spinal or epidural) preferred; general for true emergencies.
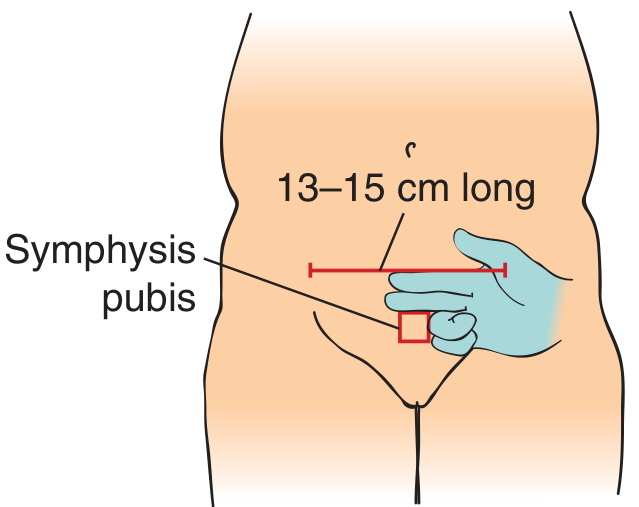
- Skin incision: Pfannenstiel (horizontal) incision ~13–15 cm, two fingerbreadths above the symphysis pubis.
- Fascial incision: Carried down through subcutaneous fat; fascia incised horizontally in midline, then extended laterally with curved Mayo scissors.
- Muscle separation: Rectus muscles bluntly separated in the midline.
- Peritoneum: Tented with hemostats and incised with scalpel; extended vertically — kept above the bladder/urachus.
- Bladder flap: Peritoneum over the lower uterine segment picked up and incised laterally (~12 cm); bladder retracted inferiorly with DeLee blade.
- Uterine incision: Low transverse hysterotomy made in the lower uterine segment; extended with bandage scissors (two fingers placed under incision to protect the fetus).
- Delivery of infant: Fetal head elevated out of the uterus (wrist kept straight); fundal pressure applied by assistant; cord clamped and cut.
- Delivery of placenta: Placenta removed by cord traction or manual extraction.
- Uterine inspection: Inner endometrium cleaned of clots and membranes; cervix dilated if closed.
- Hysterotomy closure: Running locked stitch of 0 chromic suture (one or two layers); endometrial layer not included.
- Abdominal inspection: Tubes, ovaries inspected; irrigation of pouch of Douglas and abdominal cavity.
- Tubal ligation (if desired) can be performed at this stage.
- Fascia closure: Running stitch with 1-0 Vicryl, sutures ≤1 cm apart.
- Skin closure: Subcutaneous fat irrigated; skin closed (stapler or suture).
4. Anesthesia
- Spinal anesthesia is the preferred technique for elective C-sections in the US (rapid onset, reliable).
- Epidural is used when a catheter is already in place from labor.
- Combined spinal-epidural (CSE) combines rapid onset of spinal with the flexibility of epidural top-up.
- General anesthesia is reserved for true emergencies, patient refusal of regional, or failed regional block.
Why regional is preferred over general:
- Less neonatal drug exposure
- Reduced risk of maternal pulmonary aspiration
- Less hemodynamic instability
- Mother is awake for the birth
- Spinal opioids provide excellent postoperative analgesia
Deaths from general anesthesia in obstetrics relate mainly to failed intubation, failed ventilation, or aspiration pneumonitis.
5. Complications
Intraoperative (~2% of cases)
| Complication | Notes |
|---|---|
| Hemorrhage | Most common serious intraoperative risk |
| Bladder injury | Occurs in 1–2 per 1,000 deliveries; 10× more common in C-section than instrumental vaginal delivery |
| Bowel injury | Often associated with adhesions from prior surgeries |
| Anesthesia accidents | Failed intubation, aspiration pneumonitis, drug reactions |
| Amniotic fluid embolism | Rare, usually not preventable |
| Air embolism | Rare |
| Uterine artery laceration | From lateral extension of the hysterotomy |
Postoperative (Maternal)
| Complication | Key Points |
|---|---|
| Endomyometritis | Polymicrobial; fever, uterine tenderness, malodorous lochia; treat with IV clindamycin + gentamicin |
| Wound infection | Occurs in ≤3% with prophylactic antibiotics; 25–30% caused by S. aureus; obesity is a major risk factor |
| Necrotizing fasciitis | Rare but potentially fatal; more common in obese patients |
| Urinary tract infection | Bacteriuria in ~11%; related to urethral catheterization |
| Deep vein thrombosis (DVT) | 1–2% of C-section patients; pulmonary embolism is a major cause of maternal death |
| Wound hematoma | From faulty hemostasis; treated by drainage |
| Atelectasis | Common respiratory complication |
| Adynamic ileus / bowel dysfunction | Ogilvie syndrome, sigmoid volvulus possible |
Neonatal Complications
- Fetal asphyxia from maternal hypotension (uteroplacental hypoperfusion)
- Neonatal respiratory morbidity — inversely related to gestational age at delivery; greatly increased at 37–38 weeks (elective C-section)
- Scalpel lacerations (rare)
Long-Term Complications
| Complication | Notes |
|---|---|
| Repeat cesarean | >75% incidence in subsequent pregnancies |
| Uterine rupture | 0.5–1.0% risk during trial of labor after low transverse C-section (TOLAC); much higher after classic incision |
| Placenta previa/accreta | 2–3× increased risk in next pregnancy; risk rises with each additional C-section |
| Ectopic pregnancy | Increased risk; uterine scar ectopics reported |
| Infertility | Related to fallopian tube damage from postpartum infection |
| Bowel obstruction | From intraabdominal adhesion formation |
6. Postoperative Care & Recovery
Immediate postoperative orders include:
- IV fluids: Lactated Ringer's with 20 units oxytocin at 125 mL/hr (uterine tone)
- Early ambulation: Out of bed as tolerated (reduces DVT risk)
- Diet: Clear liquids initially, advance as tolerated
- Foley catheter: Removed after 24 hours once patient is ambulating and urine is clear
- CBC on postoperative day 1
Pain management:
- PCA pump × 24 hours (preferred)
- IV morphine 2 mg q6h PRN if not tolerating oral
- Oral opioids (oxycodone/acetaminophen or hydromorphone) once tolerating PO
- Spinal opioids provide excellent postoperative analgesia when used intraoperatively
Symptom management:
- Promethazine or ondansetron for nausea
- Simethicone + bisacodyl for gas and constipation
- Docusate/sennosides as stool softeners
- RhoGAM if patient is Rh-negative
Wound care:
- Keep incision clean and dry
- Avoid coverage by skin folds (moisture → infection risk)
- Notify provider for: pus from wound, fever, painful urination, dyspnea, increasing pain
Warning signs requiring immediate attention:
- Temperature > 100.4°F
- Pulse > 110 bpm
- Increasing uterine tenderness
- Foul-smelling or excessive lochia
- Excessive vaginal bleeding
Follow-up: Wound check within 1–2 weeks postoperatively.
Sources:
- Pfenninger and Fowler's Procedures for Primary Care, 3rd ed. — Ch. 162, Cesarean Section, pp. 1133–1142
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice — Ch. 40, pp. 958–962
- Morgan and Mikhail's Clinical Anesthesiology, 7th ed. — Ch. 41, pp. 1624–1626
Pre operative care in c section
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Now I have comprehensive information from three authoritative textbooks. Here is a complete, organized response:
Preoperative Care in Cesarean Section
1. Preanesthetic Evaluation
A focused preanesthetic evaluation should be completed as early as possible and must include:
- Maternal health history — medical and surgical history, previous anesthesia, obstetric history
- Vital signs
- Airway assessment — critical because difficult intubation is a leading cause of anesthetic death in obstetrics
- Back examination — to assess suitability for regional anesthesia
- Body mass index (BMI) — obesity increases risk of almost all pregnancy complications (gestational hypertension, preeclampsia, gestational diabetes, large-for-gestational-age infants, congenital defects) and directly affects anesthesia management
- Laboratory tests — hemoglobin/hematocrit; additional labs (cardiac, hepatic, endocrine function) as clinically indicated
All obstetric patients are considered to have a full stomach regardless of reported fasting time, because pregnancy delays gastric emptying.
2. Fasting (NPO) Guidelines
| Meal Type | Minimum Fasting Period |
|---|---|
| Clear liquids | Small amounts allowed during uncomplicated labor |
| Light meal | 6 hours before elective C-section |
| Heavy (fatty) meal | 8 hours before elective C-section |
Note: For emergency C-sections, fasting status is usually unknown — aspiration precautions are always applied.
3. Aspiration Prophylaxis
Pregnancy increases the risk of gastroesophageal reflux and aspiration pneumonitis. A combination of the following is used:
| Drug | Dose | Mechanism |
|---|---|---|
| Sodium citrate (nonparticulate antacid) | 15–30 mL of 0.3 M solution orally every 30 min | Neutralizes gastric acid; raises gastric pH >2.5 immediately |
| Ranitidine (H₂-blocker) | 100–150 mg orally or 50 mg IV | Reduces gastric acid volume and pH (no effect on existing gastric contents) |
| Metoclopramide | 10 mg orally or IV | Accelerates gastric emptying; decreases gastric volume; increases lower esophageal sphincter tone |
| Omeprazole (PPI) | 40 mg orally the night before and morning of surgery | Highly effective for high-risk elective C-sections |
H₂ blockers and metoclopramide are especially recommended for high-risk patients and those expected to receive general anesthesia.
4. Informed Consent
Standard consent must be obtained covering the following risks:
- Complications of anesthesia
- Injury to the bladder or ureters
- Bowel injury
- Need for hysterectomy
- Hemorrhage requiring blood transfusion
- Infection
- Injury to the fetus (rare)
- Uterine rupture in future pregnancies
A separate consent for blood products in case of hemorrhage should also be obtained.
5. Antibiotic Prophylaxis
- Administer a single dose of antibiotic before the skin incision
- Ampicillin or first-generation cephalosporins (e.g., cefoxitin 1 g IV) are equally effective
- For penicillin-allergic patients: clindamycin 600 mg IV
- Adding azithromycin to cephalosporin prophylaxis for non-elective (emergency) cesarean deliveries significantly reduces the risk of postoperative endometritis and wound infections
- Multiple-dose regimens offer no advantage over single-dose treatment
- Prophylaxis reduces endometritis incidence from 5–15% (untreated) to much lower rates
6. Skin & Wound Preparation
- Remove hair from the incision line with clippers, not a razor (razor → increased infection risk)
- Clean the skin with chlorhexidine solution (superior to iodophor/betadine)
7. Positioning
- Left uterine displacement is mandatory in all third-trimester patients:
- A >15° wedge under the right hip, or a left tilt of the operating table
- Prevents aortocaval (vena caval) compression from the gravid uterus, which causes supine hypotension and reduces placental perfusion
- Reduces fetal asphyxia
8. IV Access & Fluid Management
- Establish adequate IV access
- Prehydration with 1,000 mL of normal saline or lactated Ringer's solution before regional (spinal/epidural) anesthesia is initiated
- Compensates for vasodilation from sympathetic blockade
- Helps prevent post-spinal hypotension
- Prophylactic vasopressors (continuous infusion) should be available for hypotension management
9. Monitoring Setup
- Standard monitors (ECG, pulse oximetry, capnography)
- Blood pressure measured every 1–3 minutes for the first 20 minutes after initiating anesthesia (neuraxial hypotension is the most common complication)
- Foley catheter insertion (bladder decompression before incision)
10. Anesthesia Choice
| Type | Preferred For |
|---|---|
| Spinal (subarachnoid block) | Elective C-section — most common in the US; rapid onset, reliable; hyperbaric 0.75% bupivacaine 12–13.5 mg |
| Epidural | When catheter already in place from labor; allows top-up dosing |
| Combined Spinal-Epidural (CSE) | Combines speed of spinal with flexibility of epidural |
| General anesthesia | True emergencies, failed/refused regional, certain maternal conditions |
Regional anesthesia is preferred because it avoids airway risks, reduces neonatal drug exposure, lowers operative blood loss, and allows the mother to be awake for birth.
11. Neonatal Resuscitation Team
- A neonatologist or skilled neonatal resuscitation provider must be notified and present, especially when C-section is performed for nonreassuring fetal status
- Appropriate neonatal resuscitation equipment must be ready in the delivery room
12. Typical Preoperative Orders Summary
| Order | Detail |
|---|---|
| IV access | Large-bore IV |
| IV fluids | 1 L lactated Ringer's preload |
| Antibiotic | Cefoxitin 1 g IV (or clindamycin 600 mg if penicillin allergy) |
| Antacid | Sodium citrate 30 mL PO |
| H₂-blocker/antiemetic | Ranitidine + metoclopramide as indicated |
| Foley catheter | Insert before incision |
| Left lateral wedge | Position before anesthesia induction |
| Blood consent | Signed separately |
| Neonatal team | Notified |
Sources:
- Morgan and Mikhail's Clinical Anesthesiology, 7th ed. — Ch. 41, pp. 1605–1606
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9th ed. — Ch. 41, p. 3495–3496
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice — Ch. 40, pp. 963–964; Ch. 48, p. 1134
- Pfenninger and Fowler's Procedures for Primary Care, 3rd ed. — Ch. 162, pp. 1133–1135
This is a shared conversation. Sign in to Orris to start your own chat.