Drugs for acute attack of migraine. I have taken naxdom 500 already
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
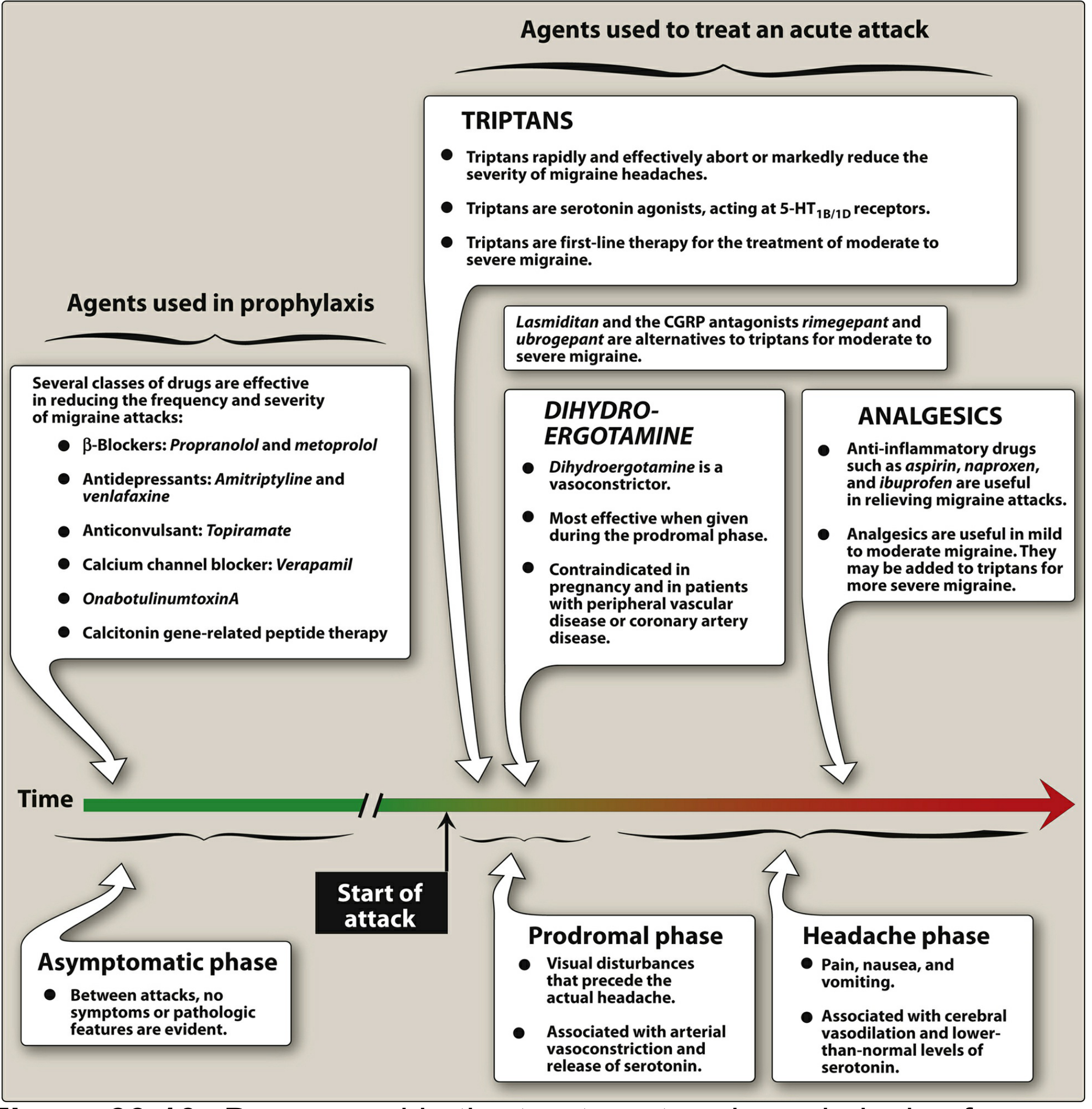
Here is a structured overview of drugs for acute migraine, with context on Naxdom 500 (naproxen sodium 500 mg + domperidone), which you've already taken.
Drugs for Acute Migraine Attack
What you've already taken: Naxdom 500
Naproxen sodium 500 mg + Domperidone 10 mg
- Naproxen is an NSAID — a nonspecific analgesic that reduces migraine pain via prostaglandin inhibition
- Domperidone treats the nausea/vomiting that accompanies migraine and also improves gastric motility (which is impaired during attacks, slowing oral drug absorption)
- This is a first-line option for mild-to-moderate migraine
Step-up options if Naxdom is insufficient
1. Triptans (migraine-specific, first-line for moderate-to-severe)
5-HT₁B/1D receptor agonists — cause cranial vasoconstriction and inhibit release of vasoactive neuropeptides (CGRP, substance P)
| Drug | Dose | Notes |
|---|---|---|
| Sumatriptan | 50–100 mg oral / 6 mg SC / 20 mg nasal | Prototype; fastest SC onset |
| Rizatriptan | 10 mg oral (wafer) | Rapid onset; good for nausea |
| Zolmitriptan | 2.5–5 mg oral or nasal spray | Nasal useful if vomiting |
| Naratriptan | 2.5 mg | Slower onset, fewer side effects, longer half-life |
| Eletriptan | 40–80 mg | Highly effective |
| Frovatriptan | 2.5 mg | Longest half-life; useful for menstrual migraine |
| Almotriptan | 12.5 mg | Well tolerated |
Triptans abort or markedly reduce migraine in ~70% of patients. They can be combined with an NSAID (like naproxen) for better efficacy — so a triptan + your Naxdom is a valid combination.
Contraindications: Coronary artery disease, uncontrolled hypertension, prior stroke, peripheral vascular disease, basilar/hemiplegic migraine.
2. Ergot Alkaloids
- Dihydroergotamine (DHE) — IV/IM/nasal spray; most effective during the prodromal phase; vasoconstrictor; contraindicated in pregnancy and vascular disease
- Ergotamine + caffeine (oral/rectal) — older option, more side effects
3. Other NSAIDs / Analgesics
If you need to add or switch:
- Ibuprofen 400–800 mg
- Aspirin 900–1000 mg (often with metoclopramide)
- Ketorolac IM — useful if oral route compromised by vomiting
- Indomethacin — particularly useful for indomethacin-responsive variants
⚠️ Since you've already taken naproxen (Naxdom), do not add another NSAID — combining NSAIDs increases GI and renal risk.
4. Antiemetics (standalone or adjunct)
- Metoclopramide 10 mg IV/IM/oral — also has mild analgesic benefit; enhances absorption of co-administered drugs
- Prochlorperazine 10 mg IM — can abort the attack on its own
- Domperidone — you already have this in Naxdom
5. Newer Agents (if triptans contraindicated or fail)
- Lasmiditan — 5-HT₁F agonist (ditan); no vasoconstriction → safe in cardiovascular disease
- Rimegepant / Ubrogepant — CGRP receptor antagonists; effective acute options, also usable for prevention
Practical Approach
You've taken Naxdom 500. Next steps depend on response:
- If mild-moderate and improving → rest in a dark, quiet room; stay hydrated; wait 1–2 hours
- If not improving in 1 hour → add a triptan (e.g., sumatriptan 50 mg or rizatriptan 10 mg)
- If vomiting prevents oral intake → use zolmitriptan nasal spray or sumatriptan SC
- In ER/clinic setting → IV metoclopramide or IM ketorolac are highly effective
Sources: Lippincott Illustrated Reviews: Pharmacology; Bradley and Daroff's Neurology in Clinical Practice; Goodman & Gilman's Pharmacological Basis of Therapeutics
Note: This is for educational purposes. For ongoing or worsening symptoms, please consult a healthcare provider.
This is a shared conversation. Sign in to Orris to start your own chat.