Ovarian and uterine changes which causes primary dysmennorhhea
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the complete answer:
Primary Dysmenorrhea: Ovarian and Uterine Changes
Primary dysmenorrhea refers to painful menstruation without underlying pelvic pathology. It appears within 1-2 years of menarche, once ovulatory cycles are established, and affects up to 60% of menstruating women.
The Role of the Ovary (Hormonal Trigger)
The ovary is the upstream initiator of primary dysmenorrhea through its luteal-phase progesterone production:
- Ovulatory cycle required: Primary dysmenorrhea occurs almost exclusively in ovulatory cycles. A corpus luteum must form and secrete progesterone.
- Progesterone primes the endometrium: During the luteal phase, progesterone stimulates prostaglandin synthetase activity in endometrial cells, priming the tissue for prostanoid production.
- Progesterone withdrawal triggers the cascade: At the end of the luteal phase, falling progesterone levels trigger lytic enzymatic action in the endometrium, releasing membrane phospholipids. These are converted to arachidonic acid, which enters the COX (cyclooxygenase) pathway.
Note: Ovarian ischemia itself is not responsible for primary dysmenorrhea - the ovary's contribution is purely hormonal (progesterone production and withdrawal).
The Prostaglandin Biosynthesis Pathway
The diagram below shows how arachidonic acid, released from cellular phospholipids, feeds into both the COX and lipoxygenase pathways:
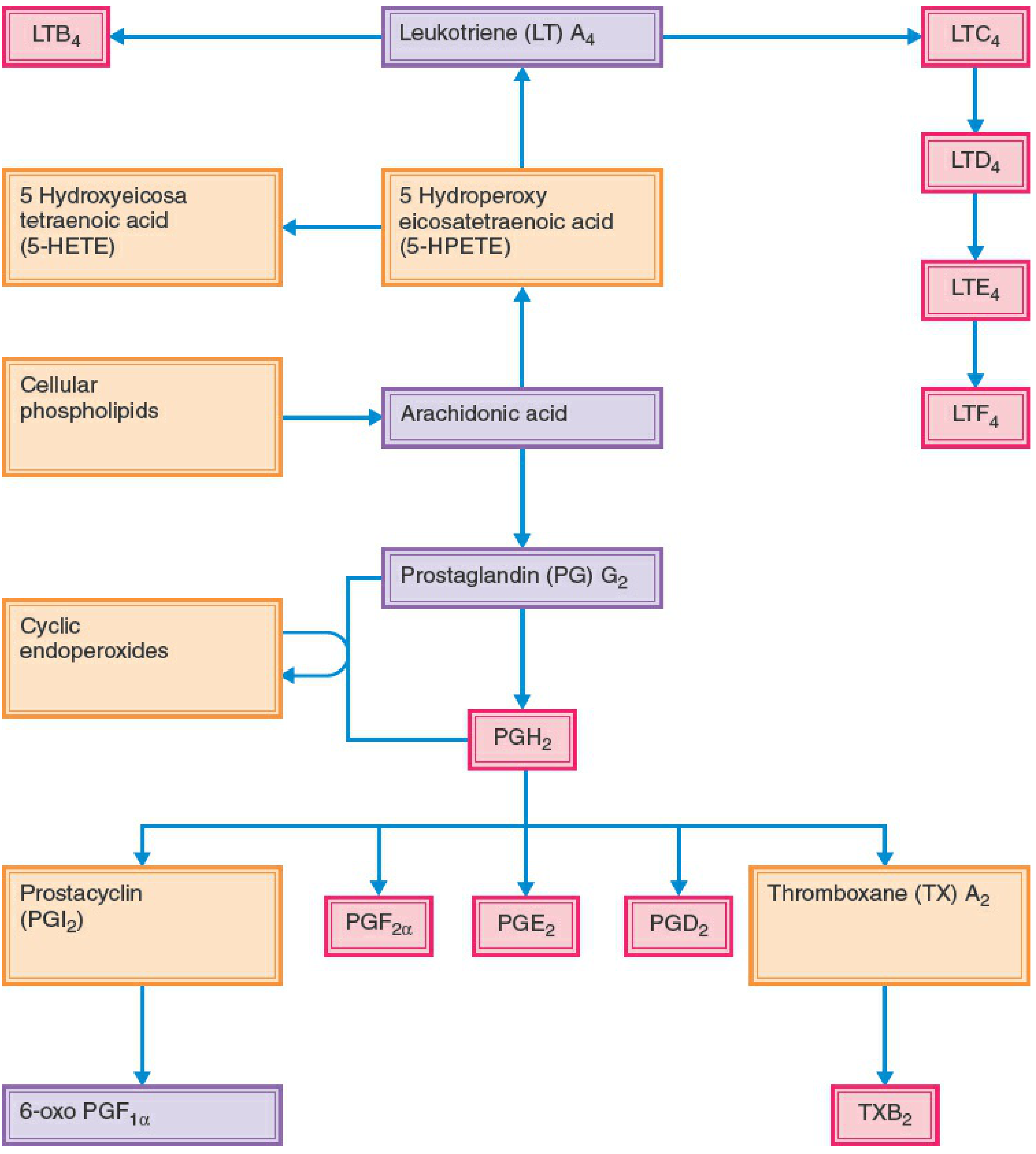
Key products from arachidonic acid that are elevated in primary dysmenorrhea:
- PGF2α - potent uterine vasoconstrictor and myometrial stimulant (most important)
- PGE2 - also a uterotonic
- Thromboxane A2 (TXA2) - vasoconstrictor
- Leukotrienes (via the lipoxygenase branch)
Women with primary dysmenorrhea have upregulated COX enzyme activity and elevated prostanoid synthase activity, leading to excessive prostanoid production compared to asymptomatic women.
Uterine Changes in Primary Dysmenorrhea
The excessive prostanoids cause several interrelated uterine changes:
| Change | Mechanism |
|---|---|
| Increased myometrial contractility | PGF2α and PGE2 directly stimulate uterine smooth muscle |
| Dysrhythmic contraction pattern | Uncoordinated, high-frequency contractions (unlike normal labor) |
| Elevated basal uterine tone | Resting pressure between contractions is abnormally high |
| High-amplitude active pressure | Intrauterine pressures can exceed 150-180 mmHg (normal: 50-80 mmHg) |
| Decreased uterine blood flow | Sustained contractions compress the myometrial vasculature |
| Vasoconstriction of uterine artery branches | PGF2α and TXA2 act on the intramyometrial branches of the uterine artery |
| Myometrial ischemia | Reduced blood flow leads to anaerobic metabolism and lactic acid accumulation |
| Uterine hypoxia ("uterine angina") | Oxygen debt in the myometrium - the direct cause of cramping pain |
| Increased peripheral nerve hypersensitivity | Prostanoids sensitize sensory nerve endings, lowering the pain threshold |
The vasoconstriction takes place specifically in the branches of the uterine artery - not in pelvic veins, and not due to ovarian ischemia.
Summary of the Cascade
Ovulatory cycle → Progesterone (luteal phase)
↓
Progesterone withdrawal (late luteal)
↓
Phospholipid release from endometrial cells
↓
Arachidonic acid ← Phospholipase A2
↓ (COX pathway, upregulated)
PGG2 → PGH2 → PGF2α, PGE2, TXA2
↓
Uterine smooth muscle hypercontractility
+ Uterine artery branch vasoconstriction
↓
Myometrial ischemia + hypoxia
↓
PAIN (dysmenorrhea)
Clinical Correlation
- Pain begins a few hours before or just after onset of menses, peaks with heaviest flow, and lasts 48-72 hours
- Character: colicky, suprapubic cramping, similar to labor pains
- Systemic effects (nausea, diarrhea, headache, syncope) are also prostaglandin-mediated
- Pelvic organs are structurally normal on examination - no pathology
Therapeutic implication: NSAIDs (COX inhibitors) block the entire prostanoid cascade at the arachidonic acid step, reducing uterine tone and ischemia. Oral contraceptives work by suppressing ovulation, removing the progesterone-withdrawal trigger and limiting prostanoid release.
Sources: Berek & Novak's Gynecology; Goldman-Cecil Medicine, International Edition; Swanson's Family Medicine Review
This is a shared conversation. Sign in to Orris to start your own chat.